
Abstract
Abstract
Background:
Patient-centered outcomes research (PCOR) methods and social learning theory (SLT) require intensive interaction between researchers and stakeholders. Advance care planning (ACP) is valuable before major surgery, but a systematic review found no extant perioperative ACP tools. Consequently, PCOR methods and SLT can inform the development of an ACP educational video for patients and families preparing for major surgery.
Objective:
The objective is to develop and test acceptability of an ACP video storyline.
Design:
The design is a stakeholder-guided development of the ACP video storyline. Design-thinking methods explored and prioritized stakeholder perspectives. Patients and family members evaluated storyboards containing the proposed storyline.
Setting/Subjects:
The study was conducted at hospital outpatient surgical clinics, in-person stakeholder summit, and the 2014 Maryland State Fair.
Measurements:
Measurements are done through stakeholder engagement and deidentified survey.
Results:
Stakeholders evaluated and prioritized evidence from an environmental scan. A surgeon, family member, and palliative care physician team iteratively developed a script featuring 12 core themes and worked with a medical graphic designer to translate the script into storyboards. For 10 days, 359 attendees of the 2014 Maryland State Fair evaluated the storyboards and 87% noted that they would be “very comfortable” or “comfortable” seeing the storyboard before major surgery, 89% considered the storyboards “very helpful” or “helpful,” and 89% would “definitely recommend” or “recommend” this story to others preparing for major surgery.
Conclusions:
Through an iterative process utilizing diverse PCOR engagement methods and informed by SLT, storyboards were developed for an ACP video. Field testing revealed the storyline to be highly meaningful for surgery patients and family members.
Background
P
For a Patient-Centered Outcomes Research Institute (PCORI)-funded study, our research group was tasked to develop and evaluate an educational, advance care planning (ACP) video for patients and family members preparing for major surgery. ACP offers individuals the opportunity to clarify their healthcare goals in preparation for future situations wherein they may be unable to make decisions.
According to the Centers for Disease Control and Prevention, 51 million inpatient surgeries were performed in the United States in 2010. 3 Postoperative admission to intensive care units (ICUs) is typically required after major surgeries 3 and is associated with increased morbidity and mortality. 4 Although multiple preoperative risk stratification tools exist,4–7 they cannot prospectively identify exactly which individual patients will experience significant postoperative complications. Given this uncertainty and the fact that >90% of severely ill ICU patients are not competent for medical decision making,8,9 patients pursuing major cancer surgery and their family members could benefit from preoperative ACP discussions.
ACP involves patients and their family members preparing for potential future loss of decision-making capacity. 10 In ACP, patients are encouraged to designate an alternative decision maker and communicate their values so that the latter is able to complete in-the-moment, values-based medical decision making, if needed. ACP decision support and educational tools can facilitate this contemplation and these conversations about a patient's goals and wishes surrounding potential medical conditions or situations. 11 Offering a standardized approach to inform patients and their family members about their healthcare choices and allowing patients and their clinicians to envision a similar disease trajectory, video ACP tools have effectively engaged and educated patients of varying ethnicities and health literacies in multiple clinical trials.12–16
Engaging patients when they are accessing healthcare may yield a biased sample, and thus researchers can consider opportunities to engage patients in their natural communities. To engage with patients and family members about video content and style in a nonmedical setting, we rented a booth at a State Fair.
Materials and Methods
An iterative PCOR process involving diverse stakeholders as well as SLT principles guided video storyline development. Design-thinking 17 methods explored and prioritized stakeholder perspectives, and the storyline was developed and then illustrated through storyboards. To evaluate the storyboards at the 2014 Maryland State Fair, patient and family member participants completed surveys asking about demographic information, as well as asking participants to rate their comfort in seeing this proposed video before major surgery, how helpful they believed it would be to see this proposed video before major surgery, and whether or not they would recommend a story like this to others preparing for major surgery. These three items were all on a nine-option Likert-type scale with responses ranging from very comfortable to very uncomfortable, very helpful to very unhelpful, and definitely recommend to definitely not recommend, respectively. Versions of this survey have been used in Volandes et al.'s studies assessing the impact of ACP videos in other settings.18–20
Part of the engagement process at the State Fair entailed asking participants to provide insights on what they perceived to be the most important purpose of the video, and thus what might be a desired outcome in a future study testing the effectiveness of the video for patients undergoing major surgery. The helpfulness and comfort level of these storyboards were included as criteria as it would be necessary that the video tool meets these two components. A separate working article details how feedback from the State Fair informed the selection of endpoints, or outcomes, for a future randomized control trial.
Results
At a stakeholder summit, a diverse group of patients, family members, palliative care clinicians, surgeons, anesthesiologists, and public health researchers evaluated and prioritized ACP tools identified through an environmental scan.21–23 Stakeholder opinion converged on the importance of (1) encouraging patients to designate an alternative decision maker; (2) advocating for patients and their family members to identify and communicate their personal values to that alternative decision maker, particularly regarding states they thought would be “worse than death”; (3) presenting real patient and family experiences and perspectives; (4) focusing on how people want to live rather than on end-of-life situations; and (5) normalizing the ACP process as one of many important tasks to complete before major surgery.
Informed by these and other data 24 and a conceptual model based on Roozenburg's empirical design cycle (Fig. 1), 25 a family member, surgeon, and palliative care physician team developed a narrative script; in the script, this team identified, selected, and featured 12 core themes (Table 1). A medical graphic designer and the study principal investigator (PI) translated these themes into 12 panel storyboards that featured text and photographs of hospital locations and patient and family member scenes (Fig. 2).
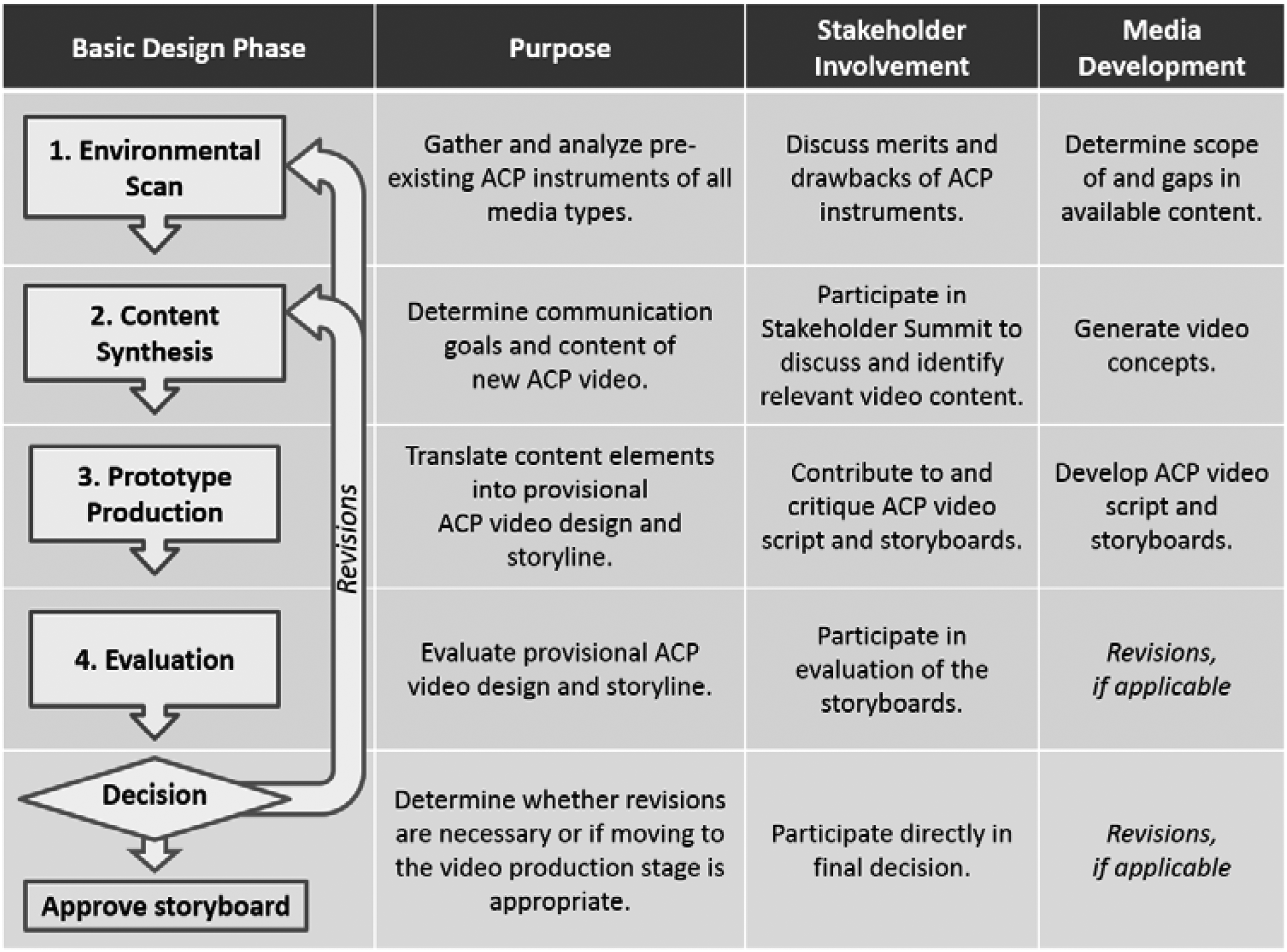
Conceptual model for storyboard development.
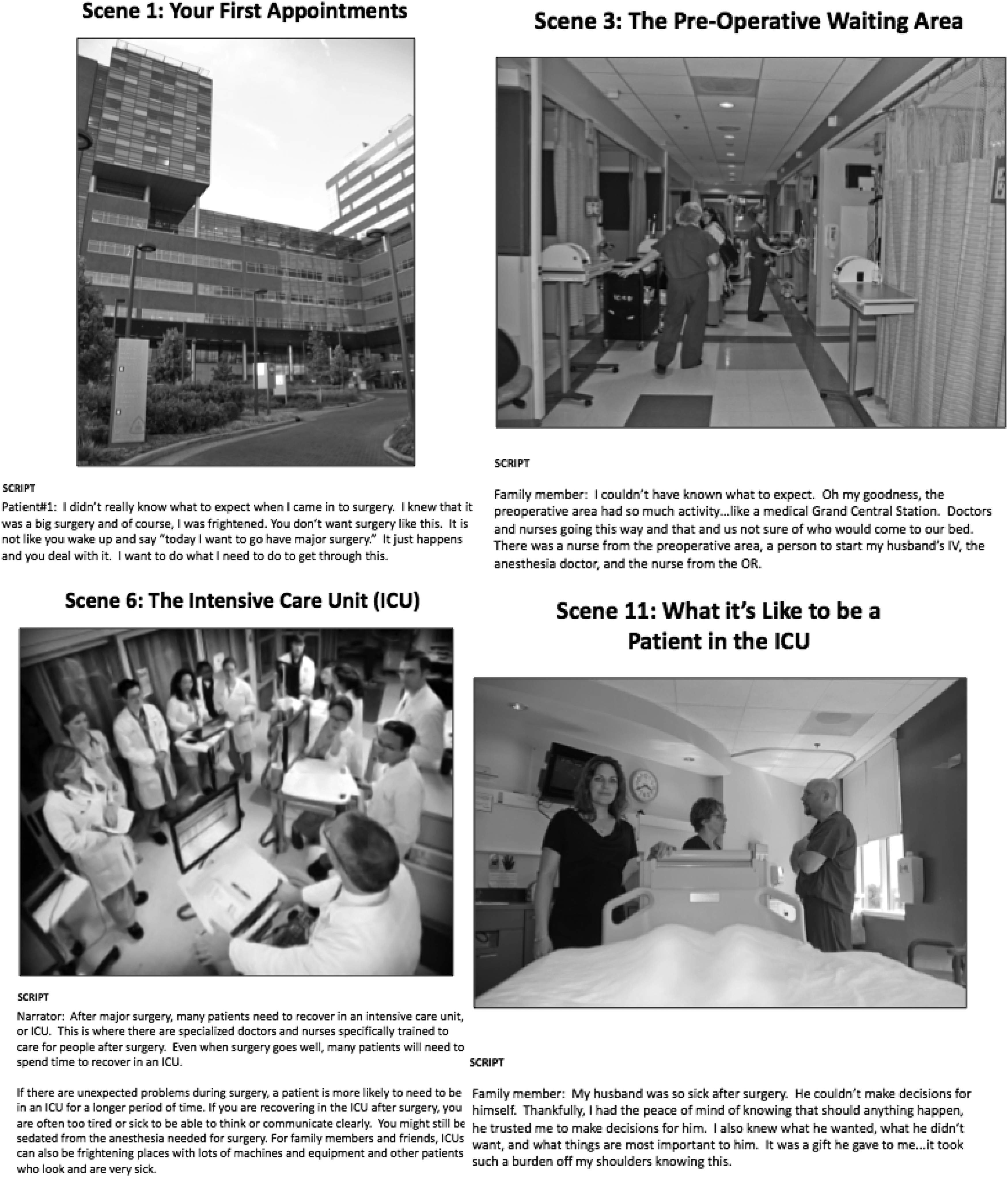
Examples of final storyboards.
ICU, intensive care unit.
To facilitate engagement with self-identified surgical patients and family members in a natural community, we rented a booth at the 2014 Maryland State Fair. More than 400,000 people typically attend the Maryland State Fair for 11 days. Our booth displayed the storyboards with signage that encouraged individuals to speak with us if they, or a loved one, had undergone surgery. Individuals who approached us were encouraged to review the storyboards and complete a deidentified 10-item Likert scale survey regarding their perception of the storyline.
In 10 days, 359 attendees of the 2014 Maryland State Fair evaluated the storyboards and completed the survey (Table 2). Among respondents, 87% noted that they would be “very comfortable” or “comfortable” seeing this storyline before major surgery, 89% considered the storyline content “very helpful” or “helpful,” and 89% would “definitely recommend” or “recommend” the storyline to others preparing for major surgery.
Discussion
With a design process informed by SLT and using multiple techniques including an environmental scan, intensive and varied types of stakeholder engagement with use of design thinking, and storyboard generation and evaluation, the study team developed a story line for a video promoting ACP among surgery patients.
This story line was examined by a large sample of the lay public who felt that a video with this storyline would be acceptable and helpful to patients preparing for major surgery and that they would recommend this video to others. It is noteworthy that a few participants disliked the image of an intubated patient; this finding reinforced the importance of developing positive preoperative ACP tools, as had been previously expressed by some stakeholders and key informants. 23 This feedback provided the necessary information for the study investigators to decide to omit images of this kind from the final video storyline.
Given that the evaluation phase showed that the storyline was acceptable to patients and their loved ones, this study demonstrates the usefulness of applying the concepts and tools from SLT, patient centeredness, existing evidence, and elements of product design to the creation of a patient-centered ACP video. In particular, results from the environmental scan and concept synthesis phases provided a comprehensive understanding of relevant ACP content and then stakeholders provided their perspectives regarding the framing and selection of the ACP video content. Without this context, the prototype production phase would likely have produced inappropriate or irrelevant content, resulting in more revisions and, potentially, a less acceptable video to stakeholders. Although the specific approach to each step is unique to this preoperative ACP video tool, these steps can be easily generalized for the development of other patient-centered tools.
The current study represents a methodological contribution to the field of ACP. ACP is a patient-centered care process, reflective of individuals' own goals and wishes both within and outside of medical care settings; the storyboarding process allows for the same types of considerations to be made. Storyboarding engages stakeholders earlier in the process than would be otherwise possible. This article focused upon how our team developed our intervention tool. We have several subsequent working articles that detail the results of our randomized control trial conducted from July 2015 to September 2016 at nine surgical oncology clinics at Johns Hopkins Outpatient Center (target n = 90) and testing the effectiveness of this tool on patient–provider preoperative communication.
In addition, this study illustrates the application of SLT to PCOR studies. As SLT integrates behavioral and cognitive theories to facilitate knowledge transfer, 2 a video can provide an opportunity to model desired behaviors and encourage viewers to actively engage in those behaviors in line with SLT. Modeling was integrated into the video storyline by featuring patients describing the relevant ACP experiences identified during the stakeholder summit. This video storyboard also depicts a typical surgery experience alongside a discussion of ACP with multiple patient and caregiver voices aiming to normalize ACP behaviors in the context of a surgical setting. Not only was the importance of normalizing ACP suggested by our stakeholders, but also attempting to do so aligns with SLT theory for both learning about surgery and ACP and promoting ACP.
Conclusions
Engaging patients and family members in natural communities about ACP aid content is both feasible and informative. Through an iterative process utilizing diverse PCOR methods and informed by SLT, we developed storyboards for an educational ACP video and field tested them with a diverse group of individuals for 11 days at a State Fair. Innovative PCOR engagement approaches can facilitate development of patient education tools that are heavily informed by patients, families, and other key stakeholders and that may consequently be more relevant, meaningful, and effective.
Footnotes
Acknowledgments
This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Communication and Dissemination Research Award (CD–12–11–4362). R.A.A. was also supported by a Johns Hopkins School of Medicine Clinician Scientist Award. S.R.I. was supported by the Canadian Institutes of Health Research (146181).
Disclaimer
The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute, its Board of Governors, or Methodology Committee.
Author Disclosure Statement
No competing financial interests exist.