
Abstract
Abstract
Background:
Most people prefer to die at home, yet most do not. Understanding factors associated with terminal hospitalization may inform interventions to improve care.
Objective:
Among patients with chronic illness receiving care in a multihospital healthcare system, we identified the following: (1) predictors of death in any hospital; (2) predictors of death in a hospital outside the system; and (3) trends from 2010 to 2015.
Design:
Retrospective cohort using death certificates and electronic health records.
Settings/Subjects:
Decedents with one of nine chronic illnesses.
Results:
Among 20,486 decedents, those most likely to die in a hospital were younger (odds ratio [OR] 0.977, confidence interval [CI] 0.974–0.980), with more comorbidities (OR 1.188, CI 1.079–1.308), or more outpatient providers (OR 1.031, CI 1.015–1.047); those with cancer or dementia, or more outpatient visits were less likely to die in hospital. Among hospital deaths, patients more likely to die in an outside hospital had lower education (OR 0.952, CI 0.923–0.981), cancer (OR 1.388, CI 1.198–1.608), diabetes (OR 1.507, CI 1.262–1.799), fewer comorbidities (OR 0.745, CI 0.644–0.862), or fewer hospitalizations within the system during the prior year (OR 0.900, CI 0.864–0.938). Deaths in hospital did not change from 2010 to 2015, but the proportion of hospital deaths outside the system increased (p < 0.022).
Conclusions:
Patients dying in the hospital who are more likely to die in an outside hospital, and therefore at greater risk for inaccessibility of advance care planning, were more likely to be less well-educated and have cancer or diabetes, fewer comorbidities, and fewer hospitalizations. These findings may help target interventions to improve end-of-life care.
Introduction
D
Identification of predictors of death in the hospital may help healthcare systems target interventions to reduce hospital deaths for those patients at highest risk. Existing literature on predictors of hospital death has not been updated recently,11–14 even though trends in site of death in the United States have shifted.15,16 In addition, many prior studies have focused only on cancer, dementia, or patients in hospice, with limited data on other chronically ill patients.12,16–18 Furthermore, recent large studies focus on international populations and may not be generalizable to the United States.17,19 Although there is an established, somewhat outdated, literature on predictors of death in a hospital, little has been published about the proportion of patients who have terminal hospitalizations in healthcare systems other than the one at which they previously received care, or about the predictors associated with such hospitalizations.
The first aim of this study was to determine the proportion of patients with chronic, life-limiting illness cared for in a multihospital academic healthcare system, who died in a hospital, as well as to identify the predictors associated with these hospital deaths. The second aim was to determine, among those who died in a hospital, the proportion who died in a hospital outside the healthcare system that had provided earlier care, and to identify the predictors of these “nonsystem” hospital deaths. Finally, we examined whether these proportions changed over time in a patterned way between 2010 and 2015.
Methods
Setting and study population
The setting was an integrated academic healthcare system, UW Medicine, comprising diverse care settings, including a university medical center, a county safety-net hospital, two community hospitals, a large clinic network, and a cancer care center. Annual patient volume exceeded 64,000 hospital admissions and 1.6 million outpatient and emergency department (ED) visits, predominantly serving the population from the greater Seattle and King County area in Washington state. The University of Washington Medical Center (UWMC) provides tertiary care for the surrounding region and had 450 beds and 50 intensive care unit (ICU) beds at the time of the study. The county safety-net hospital, Harborview Medical Center, is operated by the university and had 350 acute care beds and 94 ICU beds. This facility is the only Level 1 Trauma Center serving five states, and its mission population includes inner city poor, recent immigrants to the United States, and persons with HIV/AIDS. The two nonprofit acute care community hospitals, Valley and Northwest Medical Centers, had 303 and 281 acute care beds, respectively, and a total of 45 ICU beds. The university institutional review board assessed this project as not involving human subjects because all patients were deceased; a waiver of Health Insurance Portability and Accountability Act (HIPAA) consent was approved as required by Washington State law.
The study population was defined as patients with chronic illness who received care in the UW Medicine system and died in Washington State between 2010 and 2015. The criteria for system attribution were adapted from Dartmouth Atlas methodology 20 : at least one nonsurgical inpatient visit at an affiliated hospital in the two years before death or at least two outpatient visits from the same site in the last 32 months of life, with at least one visit occurring during the last 24 months of life. Nine chronic illnesses identified from ICD-9 coding in the electronic health record (EHR) were included: nonhematologic cancer, chronic pulmonary disease, coronary artery disease (CAD), congestive heart failure (CHF), chronic liver disease, chronic renal disease, dementia, diabetes, and peripheral vascular disease. Decedents were excluded if they were <18 years old at the time of death or if the death certificate indicated that death was due to “injury or poisoning emanating from an accident, suicide, homicide, or an undetermined source.”
Data sources
Data from Washington State death certificates were merged with the following information, extracted from the EHR: birthdate, gender, chronic illness diagnoses based on ICD9 coding, insurance status and healthcare system utilization between 1 and 13 months before death (including outpatient, inpatient, and ED visits), and a count of unique outpatient providers. We used 1–13 months so as not to overlap with the last month of life, but retain a one-year timeframe. Death certificate data included location and date of death, level of education, marital status, and race/ethnicity. If the date or location of death was not available from death certificate data, it was obtained from the EHR. Decedents without a known site of death from either source were excluded from analysis (n = 1582).
Outcomes
There were two outcomes of interest: death in any hospital and, among those who died in a hospital, death in a hospital outside the academic healthcare system.
Predictors
We examined the following predictors for their association with the two outcomes: decedent's age at death (as a continuous variable); gender; marital status (never married, currently married, or previously married); education level (an eight-category ordinal variable); race/ethnicity (white, African American, Native American, Asian, Pacific Islander, Hispanic, or other/mixed race); number of chronic illness diagnoses (three ordinal categories: 1, 2, and 3, or more); healthcare utilization between 1 and 13 months before death, including the number of hospital admissions, ED visits, outpatient visits, and unique outpatient providers; insurance status (private insurance, Medicare, Medicaid, military, other insurance type, and no apparent insurance [e.g., those listed as “self-pay” or with no listed insurance information]); and year of death.
Analysis
We used logistic regression models with restricted maximum likelihood estimation to assess the association of the predictors with death in any hospital and, among those who died in a hospital, with death in a hospital outside the academic health system. All predictors except year of death were included in each model simultaneously, with each model including those patients who had complete data on all predictors and the outcome. Analysis of the association between year of death and site of death included only the year-of-death predictor and actual confounders. To be considered an actual confounder, we required that addition of the variable into the bivariate model changed the year-of-death coefficient by at least 10%. Analyses were conducted with Mplus (www.statmodel.com). Given the multiple comparisons made in identification of predictors of death in the hospital or, among those who died in the hospital, of death in a hospital in the healthcare system, we considered a p-value ≤0.001 to connote statistical significance based on the Bonferroni correction. However, since analyses examining the trend over time did not include multiple potential predictors, we retained p < 0.05 to indicate statistical significance.
Results
Sample description
Decedent demographics and diagnostic characteristics by site of death are presented in Tables 1 and 2. There were 20,486 deaths in the state of Washington from 2010 to 2015 among individuals who met the inclusion criteria, including attribution to the healthcare system and known site of death. Overall, 57% of decedents were male (n = 11,709), 47% were married (n = 9715), and the average age at death was 66 years. About a third had private insurance (34%; n = 6917), and another 34% (n = 6895) had Medicare. The most common chronic illness was cancer (52%; n = 10,550), followed by COPD (27%; n = 5496) and CAD (26%; n = 5229). Diabetes and dementia were the least represented at 9% of the decedent population each (n = 1841 and 1920). The mean number of diagnoses was 1.9 per decedent.
Except where noted otherwise, the statistics presented are n (percentage of sample size for the column).
Missing data on race/ethnicity reduced the sample sizes to 12,006 and 7828.
Statistics presented are mean (SD).
Missing data on marital status reduced the sample sizes to 11,912 and 7776.
Missing data on education reduced the sample sizes to 11,820 and 7626.
CAD, coronary artery disease; CHF, congestive heart failure; CPD, chronic pulmonary disease; ED, emergency department; PVD, peripheral vascular disease; SD, standard deviation.
Except where noted otherwise, the statistics presented are n (percentage of sample size for the column).
Missing data on race/ethnicity reduced the sample sizes to 3917 and 3911.
Statistics presented are mean (SD).
Missing data on marital status reduced the sample sizes to 3881 and 3895.
Missing data on education reduced the sample sizes to 3754 and 3872.
UW, University of Washington.
Forty-one percent of deaths (n = 8461) occurred in a hospital setting. Among these, 46% (n = 3920) occurred in a hospital outside the academic healthcare system. Other sites of death included home (36%; n = 7279), nursing home (15%, n = 3121), inpatient hospice (6%, n = 1251), and miscellaneous other sites (2%, n = 374).
Patient and healthcare utilization characteristics associated with death in any hospital
Multipredictor analyses of patient and healthcare characteristics associated with death in any hospital were completed with a sample of 19,365 decedents; 1121 (5.5%) of the decedents were excluded due to missing data (education, marital status, or both) (Table 3). Predictors associated with a significantly greater odds of dying in a hospital included younger age (odds ratio [OR] 0.977 for each additional year of age, confidence interval [CI] 0.974–0.980), absence of a diagnosis of cancer (OR 0.411, CI 0.372–0.453) or dementia (OR 0.536, CI 0.471–0.612), presence of a diagnosis of CHF (OR 1.234, CI 1.113–1.368, p < 0.001), having a greater number of diagnoses (OR 1.188 for each additional diagnosis, CI 1.079–1.308), having fewer outpatient visits within the system in the prior year (OR 0.986 for each additional outpatient visit, CI 0.981–0.991), and having more outpatient providers in the healthcare system (OR 1.031 for each additional provider, CI 1.015–1.047). Race/ethnicity and marital status were also significantly associated with the odds of a hospital death, with minority racial/ethnic groups and currently married persons having somewhat greater odds of dying in a hospital than was true for their counterparts. Gender, level of education, insurance coverage, and usage of inpatient or ED care in the prior year were not significantly associated with death in a hospital.
Logistic regression model with all predictors included simultaneously, estimated with restricted maximum likelihood. Overall p for unordered categorical predictors was tested with the Wald test of parameter constraints. Model based on the sample of 19,365 patients for whom there were complete data on all predictors and the outcome.
The number of Dartmouth Atlas chronic conditions with which the patient had been diagnosed, measured with a three-category ordinal variable: 1 = 1 diagnosis, 2 = 2 diagnoses, 3 = 3 or more diagnoses.
Bold signifies p < 0.001.
CI, confidence interval; OR, odds ratio.
Characteristics associated with death in a hospital outside the healthcare system
Among patients who died in a hospital, the following characteristics were associated with significantly increased odds of dying in a hospital outside the healthcare system: having less education (OR 0.952 CI 0.923–0.981), having a diagnosis of cancer (OR 1.388, CI 1.198–1.608) or diabetes (OR 1.507, CI 1.262–1.799), not having a diagnosis of CHF (OR 0.641, CI 0.551–0.747), having fewer comorbid conditions (OR 0.745, CI 0.644–0.862), and having fewer admissions at system hospitals during the prior year (OR 0.900, CI 0.864–0.938) (Table 4). Race/ethnicity and marital status were also significantly associated with the odds of dying in a nonsystem hospital, with white non-Hispanics more likely than African Americans or Asians to die in nonsystem hospitals, and with currently or previously married persons more likely than the never married.
Logistic regression model with all predictors included simultaneously, estimated with restricted maximum likelihood. Overall p for unordered categorical predictors was tested with the Wald test of parameter constraints. Model based on sample of 7601 patients who died in a hospital and for whom there were complete data on all predictors and the outcome.
The number of Dartmouth Atlas chronic conditions with which the patient had been diagnosed, measured with a three-category ordinal variable: 1 = 1 diagnosis, 2 = 2 diagnoses, 3 = 3 or more diagnoses.
Bold signifies p < 0.001.
Trends in site of death over time
After adjustment for confounders, there were no significant linear patterns over the six-year period (2010–2015) in the odds of death in any hospital (Table 5). However, among hospital deaths, the odds of dying in a hospital outside the healthcare system increased over time (OR 1.032, CI 1.005–1.060). Figure 1 shows the percentage of all deaths that occurred in any hospital over time; Figure 2 shows the percentage of hospital deaths that occurred in nonsystem hospitals.
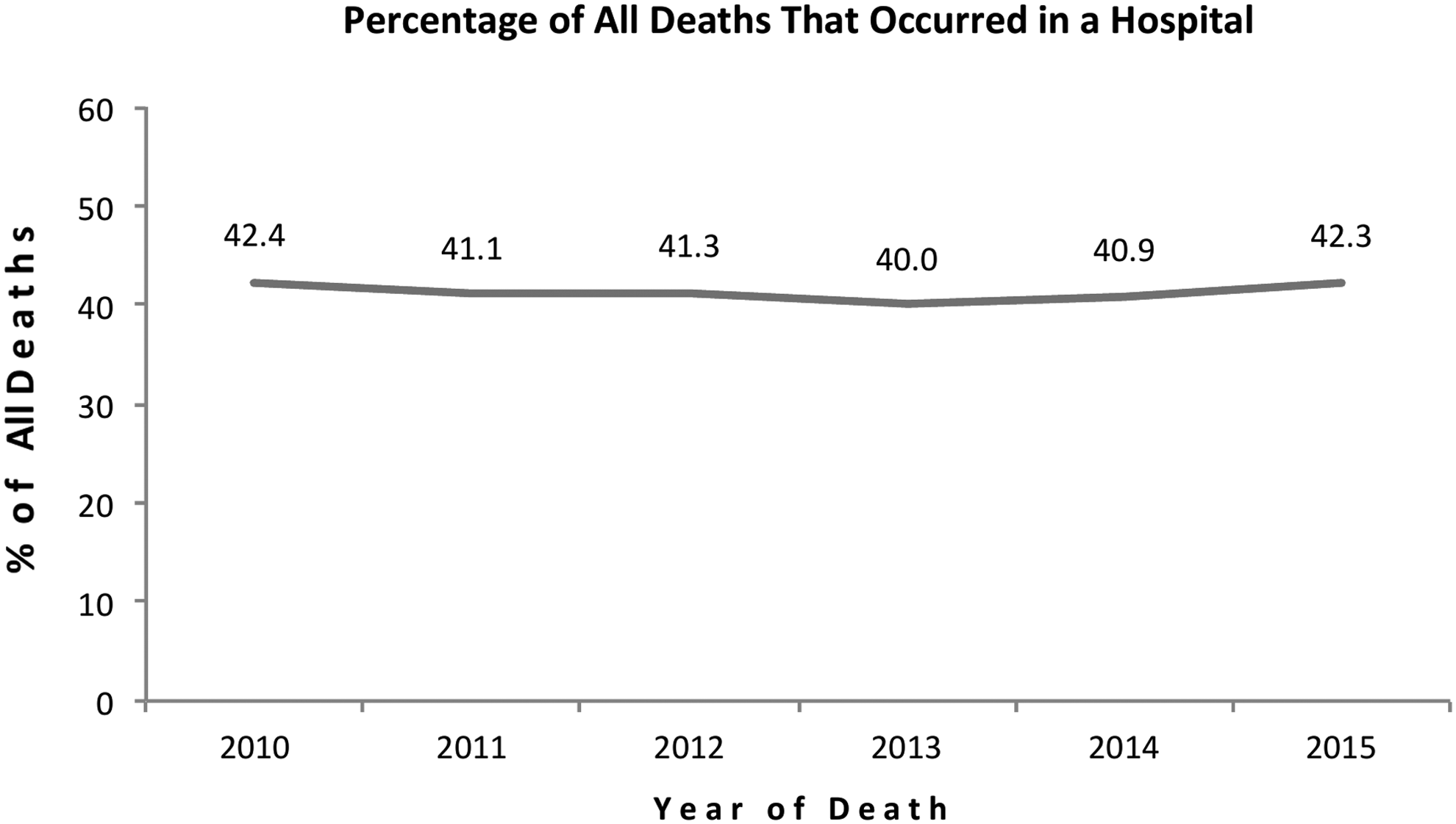
Percentage of all deaths that occurred in a hospital.
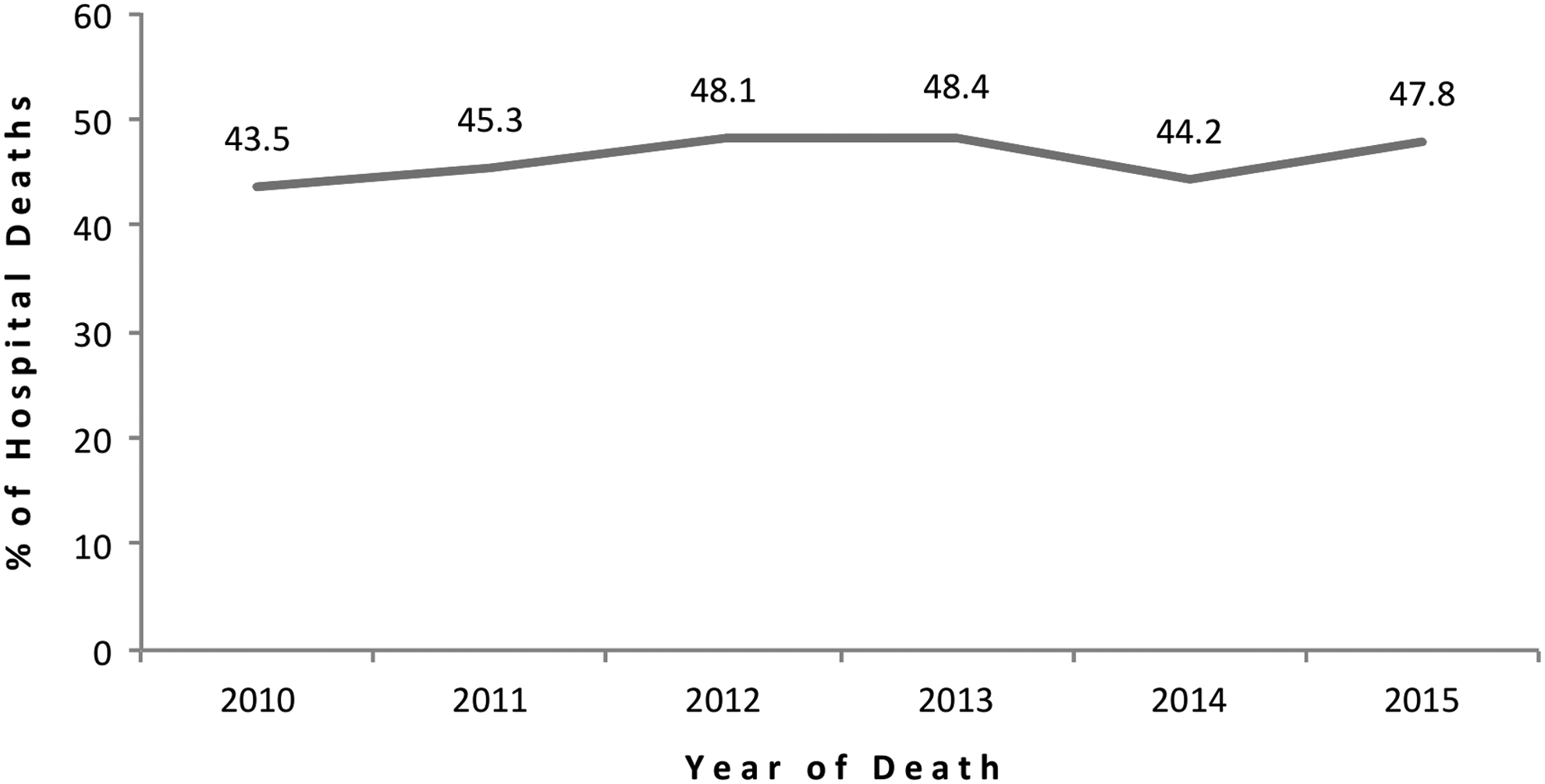
Percentage of all hospital deaths that occurred in a nonsystem hospital.
Logistic regression models, estimated with restricted maximum likelihood. Year of death (2010–2015) was entered as an ordinal predictor (coded 0–5).
When the p-value for the unadjusted model was <0.50, adjustment was made for any variable whose addition to the model with year of death as the only predictor changed the estimated coefficient for year of death by 10% or more.
The high p-value for year of death in the unadjusted model preluded the need to test for confounders, so the unadjusted model is the final model.
The final model included adjustment for age, race/ethnicity, insurance status, diagnosis, number of diagnoses (three-level ordinal variable), and the number of hospital admissions, ED visits, and outpatient visits occurring 1–13 months before death.
The final model included adjustment for age, diagnosis, and the number of hospital admissions, ED visits, and outpatient visits occurring 1–13 months before death.
The final model included adjustment for age, insurance status, diagnosis, number of diagnoses (three-level ordinal variable), and the number of hospital admissions, ED visits, outpatient visits, and outpatient providers in the 1–13 months before death.
Bold signifies p < 0.05.
Discussion
We examined the proportion of deaths that occurred in the hospital among decedents cared for by a large multisite academic healthcare system from 2010 to 2015. In addition, among patients dying in the hospital, we examined whether these patients died in hospitals that were not affiliated with this healthcare system. Our goal was to update the factors that might differentiate patients at risk for dying in any hospital as well as identify the predictors for death in a hospital not affiliated with the healthcare system that had provided recent care, which has not previously been evaluated. This information may be useful to healthcare systems that are developing advance care planning programs and seek to ensure that information generated by advance care planning is available to clinicians providing care at the end of life, wherever that care may occur. Effective advance care planning that crosses healthcare systems will be particularly important in the context of accountable or population-based capitated care programs. 21
Among decedents with at least one of nine chronic illnesses, we found that ∼40% of these deaths occurred in hospitals throughout the six-year study period; these rates are similar to national rates reported by the CDC. 6 Within our population of decedents with at least one chronic illness, receiving care within a large academic healthcare system, older patients and those with a diagnosis of cancer or dementia were less likely to die in a hospital, and this finding is consistent with prior studies.12,14,19,22–25 It is likely that a more predictable disease course with more prognostic certainty, such as with malignancy or dementia, allows patients and their clinicians opportunities to communicate and implement goals of care; these goals of care may, in turn, reduce the likelihood of a terminal hospitalization and allow patients, families, and providers to prepare for a death guided by patient's goals and preferences. These patient groups are also more likely to be enrolled in hospice services at the end of life, which may contribute to our findings. 2 Conversely, we found that patients with more comorbid diagnoses were more likely to die in a hospital. Because the course of illness for these patients may be more complicated and less predictable, and because these individuals may have multiple care providers and more fragmented care, the risk of death in a hospital may be increased. In our review of literature, this predictor has not been evaluated previously.
We found that decedents who died in a hospital were more likely to be married at the time of death. In contrast, older studies have shown that being married is associated with a greater likelihood of death at home: a fact that has been attributed to the increased social support available to married persons.12,14,22–25 Further studies are needed to determine whether this association is changing over time. We also found that non-white race was associated with greater likelihood of death in a hospital similar to prior findings.11–14 We found no association between level of education and place of death, unlike prior work that suggests higher income and education are associated with greater likelihood of home death.13,14,23,26 We also did not find an association between payer type and site of death, whereas prior work has shown an association between increased health maintenance organization penetrance and decreased hospital deaths, 13 and an association of Medicare coverage with greater likelihood of death at home. 27 In addition, some prior studies suggest that death at home is more common among individuals living at some distance from a hospital, a variable we were not able to assess. 14
Utilization patterns in the year leading up to the last month of life indicated that patients who had a greater number of visits in the system's outpatient setting were less likely to die in a hospital. These patients may have had more opportunities to establish a relationship with a provider with whom they were able to discuss end-of-life goals and establish a plan of care that facilitated death outside the hospital. In contrast, we found that patients who saw a larger number of unique outpatient providers were more likely to die in the hospital; this finding is in line with the Institute of Medicine's assertion that fragmented care leads to higher intensity care. 1
In our analyses of factors associated with death in a hospital external to the target healthcare system, we found that decedents at greatest risk for death at a hospital outside the healthcare system included patients with lower education, patients with cancer or diabetes, fewer comorbid conditions, and fewer recent admissions at hospitals within the system. Race and marital status were also significantly associated with death in nonsystem hospitals. These factors may be useful in identifying patients who would benefit more from a focus on advance care planning that can be accessed outside the healthcare system.
Our study has several important limitations. First, we focused on a single healthcare system in a single state, and our findings may not generalize to other healthcare systems or states. However, the academic healthcare system we examined is a large diverse system that may be similar to other academic healthcare systems. Second, we used data from the EHR that were collected for clinical purposes rather than research, and our findings may be limited by diagnostic misclassification associated with inaccurate or incomplete documentation. However, the EHR also offers advantages in containing information not present in claims databases and providing information on more patients than many research databases. Third, distance to the nearest hospital may have been a factor associated with hospital death outside the healthcare system, but we did not have reliable information that would enable us to estimate this. Fourth, we examined the chronic conditions that patients had before death, but did not ascertain the cause of death. Fifth, we do not have reliable data on the market share for this healthcare system, which might influence temporal trends. Finally, we were unable to determine the proportion of patients for whom death in the hospital was the preferred location.
In summary, we found that among patients with chronic life-limiting illness, those with an illness portending a less-predictable disease course—such as younger age, more comorbid illnesses, or a diagnosis of CHF—were more likely to die in a hospital setting. Those dying in a hospital outside the healthcare system, and therefore possibly at risk for fragmented care and inaccessibility of advance care planning documentation at the end of life, were likely to be less well educated, currently or previously married, with diagnoses of cancer or diabetes, and fewer comorbid conditions. This group of patients dying in hospitals outside the healthcare system appears to be increasing over time, although further studies should confirm this finding in other healthcare systems.
Footnotes
Acknowledgment
This study was funded by the Cambia Health Foundation and UW Medicine.
Author Disclosure Statement
No competing financial interests exist.