
Abstract
Abstract
Background:
The interpretation of do-not-resuscitate orders (DNRs) may vary in nonarrest situations. To reduce ambiguity, many hospitals allow patients to elect partial DNRs.
Objective:
To investigate the effect of partial DNRs on physicians' willingness to perform cardiopulmonary resuscitation (CPR) and nonarrest procedures.
Design:
Cross-sectional study using scenario-based questionnaires between October 2015 and March 2016. A partial DNR was identified as a DNR with Adult Emergency Protocols (AEP) order. Each survey presented 3 patient scenarios followed by 10 interventions.
Setting/Subjects:
Preclerkship and clerkship medical students, and internal medicine residents at a single medical school, and hospitalists at a tertiary-care academic medical center.
Results:
Responses from 275 of 366 (75.1%) eligible subjects were collected. Compared to the case with a full DNR, the presence of a partial DNR was positively associated with subjects' willingness to provide both nonarrest procedures and CPR (p < 0.05). The number of training or practice years was positively associated with a decision not to perform CPR: case 1 (odds ratio [OR], 1.09; confidence interval [CI], 1.04–1.16; p = 0.003); case 2 (OR, 1.07; CI, 1.01–1.14; p = 0.03); and case 3 (OR, 1.09; CI, 1.04–1.16; p < 0.001).
Conclusions:
A partial DNR made our respondents more willing to provide nonarrest procedures, but also CPR. These findings suggest an ongoing need to develop better means of incorporating patients' goals of care into orders that more faithfully guide care for both nonarrest and arrest situations.
Introduction
A
Several reasons may explain why DNRs are misinterpreted. First, simple binary DNRs (resuscitate vs. do not resuscitate) do not accommodate the clinical reality that prearrest and arrest situations often sit along a continuum of physiologic deterioration. 4 For example, endotracheal intubation, which is part of the resuscitation protocol, may be withheld for a patient with a DNR. However, endotracheal intubation may prevent progression from a prearrest to an arrest state (e.g., in the setting of pneumonia, an exacerbation of congestive heart failure, or chronic obstructive pulmonary disease). This withholding of endotracheal intubation during the prearrest situation may be inconsistent with patients' preferences. 5 Second, inadequate communication about prognosis, the likelihood of benefit from nonarrest and arrest emergency treatments, and the overall goals of care among providers, patients, and family members may create unnecessary confusion. Finally, patients with DNRs often have various comorbidities and levels of disability, and physicians may incorrectly presume that patients they view as having a diminished quality of life would wish to forgo what the physician may view as overly aggressive life-prolonging treatments. 3
In an attempt to reduce ambiguity, many hospitals allow patients and their physicians to designate a code status between full support and DNR, such as partial DNR or limited resuscitation orders. At our institution, a partial DNR is identified as DNR with Adult Emergency Protocols (AEP) order. The AEP order governs the use of nonarrest emergency procedures and is composed of yes/no decisions regarding the use of (1) noninvasive ventilation, (2) mechanical ventilation, (3) intravenous vasopressors, (4) intravenous antiarrhythmic medications, (5) elective cardioversion, and (6) cardiac pacemaker. However, little is known about the effectiveness of partial DNRs.4–6 In addition, medical and bioethics organizations have published guidelines and recommendations on the ethical use of DNRs, with little mention of partial DNRs.1,7,8
Here, we describe a cross-sectional study using three case scenarios (an elderly man with advanced cancer and dementia, a middle-aged woman with advanced cancer, and a young man with advanced AIDS-related illness) followed by potential diagnostic tests and interventions to investigate the effect of DNR and partial DNRs on the respondents' willingness to perform both CPR and nonarrest procedures. In addition, we assessed the association between years of training or practice and the respondents' choices.
Methods
Study administration and ethical approval
Data were obtained by self-administered scenario-based questionnaire survey using paper-and-pencil methodology. Surveys were administered between October 2015 and March 2016 to hospitalists attending physicians at a tertiary-care academic medical center (The Queen's Medical Center, Honolulu, HI), University of Hawaii internal medicine residents, and University of Hawaii medical students (MS). The survey and protocol were approved and granted a waiver of informed consent by the Institutional Review Boards at The Queen's Medical Center and University of Hawaii because the study required no intervention and no significant risk of breach of privacy or anonymity.
Study design
Questionnaires were conducted anonymously and elicited only the following self-reported identifiers: subject's current position (first to fourth year MS [MS1–4], postgraduate year [PGY] 1–3 for residents, and hospitalists attending physicians); year of medical school graduation; U.S. medical school graduate versus international medical graduate (IMG) status; and gender. Surveys were collected in a collection box that was retrieved at the end of the study period. The survey instrument presented three clinical vignettes involving patients with serious and life-threatening illness (copies of the vignettes are available from the authors). With permission, all vignettes were adapted with modifications from case descriptions used by Beach and Morrison. 3
The questionnaire included 30 questions (10 questions per case scenario). Each case included a brief case vignette followed by options for CPR and nonarrest procedures that were described in the questionnaire. The 10 treatment decisions were organized so that each scenario contained at least 1 of each of the following 3 categories: (1) minimally invasive procedures (blood cultures, blood transfusions, antibiotics, supplemental oxygen therapy, computerized tomography, and bone scan); (2) invasive procedures (central line placement, lumbar puncture, thoracentesis, and bone marrow biopsy); and (3) complex invasive procedures (esophagogastroduodenoscopy, colonoscopy, bronchoscopy, hemodialysis, inferior vena cava filter, and abdominal surgery). The last three treatment decisions in each scenario involved ICU transfer, emergent intubation, and CPR. The first seven interventions were classified as nonemergency procedures. Emergent intubation and ICU transfer were classified as nonarrest emergency procedures.
Using a four-point Likert scale (strongly agree to strongly disagree), respondents were asked to indicate whether they would initiate each intervention. Case 1 was a 72-year-old man with advanced multiple myeloma and dementia that had a DNR with an AEP order. Case 2 was a 48-year-old woman with advanced breast cancer that had a DNR without an AEP order (defined as full DNR). Case 3 was a 34-year-old man with advanced AIDS-related illness that had a DNR with an AEP order. In cases 1 and 3 (DNR with AEP), we expected respondents would initiate both nonemergency and nonarrest emergency procedures, but not CPR. In case 2 (full DNR), we expected respondents would initiate nonemergency procedures, but neither nonarrest emergency procedures nor CPR.
Statistical methods
The primary aim of this analysis was to compare the decision-making pattern of subjects among scenarios in which the patient had DNRs, either with or without an AEP order. The primary outcome variables were the percentages of agree or strongly agree responses to each of the 10 treatment decisions for each of the 3 scenarios. Chi-square tests were used to compare the percentage of respondents agreeing to initiate each therapy in the presence or absence of an AEP order. We categorized the following groups for the analysis: preclerkship students (MS1 and MS2) as group 1; clerkship students (MS3 and MS4) as group 2; residents (PGY1–3) as group 3; and hospitalists attending physicians as group 4.
The secondary outcome was to assess the association between years of training or practice and the respondents' inclination to initiate specific interventions. The years of training or practice were considered one for MS1, two for MS2, three for MS3, four for MS4, and four plus the number of years after graduation for residents and hospitalists attending physicians. Ordinal logistic regression analysis was used for analysis. Statistical analyses were performed with R 3.2.3 GUI 1.66 (R Foundation for Statistical Computing). A p value <0.05 was considered statistically significant. Continuous variables were expressed as medians with 25th and 75th percentiles, and discrete variables were summarized as percentages.
Results
Respondents
Among the 366 eligible subjects, we collected 283 questionnaires (77.3% response rate). Of the 283 collected questionnaires, 8 questionnaires from clerkship students could not be analyzed because of incomplete data; hence, 75.1% (275/366) of the questionnaires were analyzed. The analyzed sample comprised 134 preclerkship students (49%), 85 clerkship students (31%), 34 residents (12%), and 22 hospitalists attending physicians (8%). Among the respondents, 128 (46.5%) were men and 15 (5.5%) were IMG. The medians of training or practice years (25th and 75th percentiles) were as follows: Group 1, 1.5 (1 and 2); Group 2, 3.5 (3 and 4); Group 3, 6 (5 and 7); and Group 4, 16.5 (12.25 and 24.75).
The effect of AEP on inclination to provide nonemergency and nonarrest emergency procedures
Compared to case 2 (full DNR), case 3 (DNR with AEP) was positively associated with subjects' intent to provide nonemergency procedures (p < 0.001 for groups 1–3 and p < 0.05 for group 4) (Fig. 1). We also found that cases 1 and 3 (DNR with AEP) were positively associated with subjects' intent to provide nonarrest emergency procedures in all groups compared to case 2 (full DNR) (p < 0.001) (Fig. 2).

The effect of AEP on inclination to provide nonemergency procedures. Case 1—an elderly man with advanced cancer and dementia that had a DNR with an AEP order; Case 2—a middle-aged woman with advanced cancer that had a DNR without an AEP order; Case 3—a young man with advanced AIDS-related illness that had a DNR with an AEP order. †p < 0.05; *p < 0.001. AEP, Adult Emergency Protocols; DNR, do-not-resuscitate order.
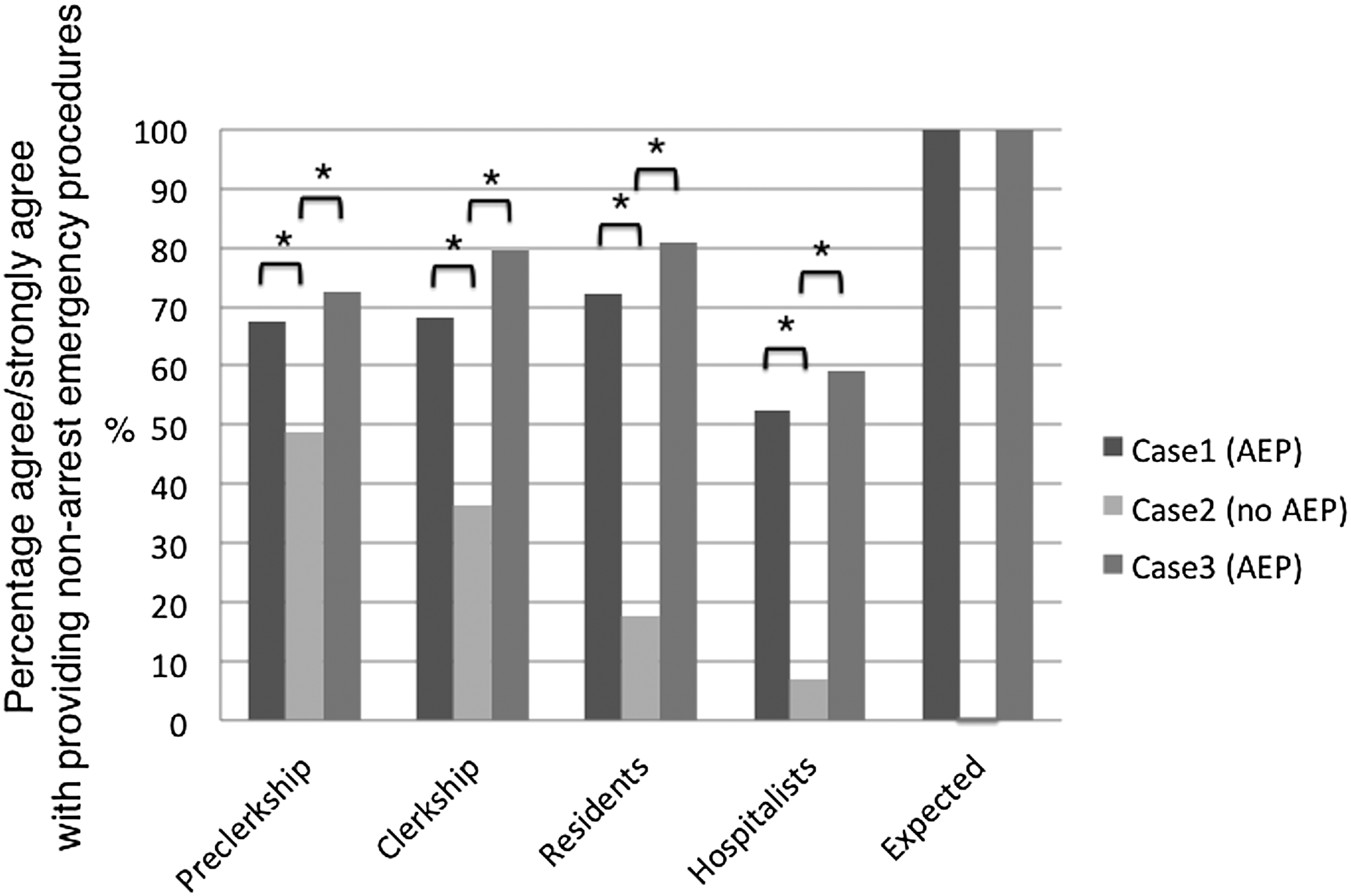
The effect of AEP on inclination to provide nonarrest emergency procedures. Nonarrest emergency procedures—Emergent intubation and intensive care unit transfer. Case 1—an elderly man with advanced cancer and dementia that had a DNR with an AEP order; Case 2—a middle-aged woman with advanced cancer that had a DNR without an AEP order; Case 3—a young man with advanced AIDS-related illness that had a DNR with an AEP order. *p < 0.001.
The effect of AEP on inclination to provide CPR
Even though the patients in all three scenarios had a DNR in place, compared to case 2 (full DNR), the presence of an AEP order in cases 1 and 3 was positively associated with subjects' intent to provide CPR in groups 1–3 (p < 0.001 [case 1 and 3], p < 0.001 [case 3], and p < 0.05 [case 1 and 3], respectively) (Fig. 3). None of the hospitalists attending physicians indicated an intent to provide CPR for either full or partial DNR scenarios.

The effect of AEP on inclination to provide cardiopulmonary resuscitation. Case 1—an elderly man with advanced cancer and dementia that had a DNR with an AEP order; Case 2—a middle-aged woman with advanced cancer that had a DNR without an AEP order; Case 3—a young man with advanced AIDS-related illness that had a DNR with an AEP order. †p < 0.05; *p < 0.001.
Association between years of training or practice and respondents' inclination to initiate interventions
The number of training or practice years was positively associated with a decision not to perform CPR in all cases as follows: case 1 (coefficient, 0.09 [confidence interval, CI 0.03–0.15]; odds ratio [OR], 1.09 [CI 1.04–1.16]; p = 0.003); case 2 (coefficient, 0.06 [CI 0.01–0.13]; OR, 1.07 [CI 1.01–1.14]; p = 0.03); and case 3 (coefficient, 0.09 [CI 0.04–0.15]; OR, 1.09 [CI 1.04–1.16]; p = 0.001). In addition, there was also a statistically significant association between number of training or practice years and a decision not to provide nonarrest emergency procedures in case 2 (coefficient, 0.06 [CI 0.03–0.09]; OR, 1.06 [CI 1.03–1.09]; p < 0.001) (Table 1).
Case 1, an elderly man with advanced cancer and dementia that had a DNR with an AEP order; Case 2, a middle-aged woman with advanced cancer that had a DNR without an AEP order; Case 3, a young man with advanced AIDS-related illness that had a DNR with an AEP order.
AEP, Adult Emergency Protocols; CI, confidence interval; CPR, cardiopulmonary resuscitation; DNR, do-not-resuscitate order; OR, odds ratio.
Discussion
For our respondents, the presence of a partial DNR, that is, DNR with an AEP order, created an apparent paradox of medical decision making. The presence of the DNR with an AEP order increased the likelihood that our respondents would provide nonarrest emergency procedures. It also, for case 3, increased the likelihood that patients would be provided nonemergency procedures. On the other hand, the presence of the DNR with an AEP order increased the risk that our respondents would not honor the DNR in arrest situations. Clinical experience modified this risk, as we found a significant association between years of training or practice and the willingness to honor the DNR part of a DNR with an AEP order.
The goal of DNRs is to clarify patient wishes for treatment at the end of life. Partial DNRs have been developed in an effort to further refine these treatment preferences. While concerns have been raised about the impact of DNRs on nonarrest situations, to our knowledge, this is the first study to examine the potential impact of partial DNRs. Our findings add support the concerns of patients, family members, and providers that a DNR, whether full or partial, may be misinterpreted as a “do-not-treat” order.2,3,9,10
Improperly managed prearrest conditions may lead to further clinical decompensation and cardiac or respiratory arrest, but a DNR, by itself, is not designed to guide management in those prearrest situations. 11 Partial DNRs are intended to allow individual treatment wishes for patients in prearrest situations. However, it is impossible to anticipate all possible prearrest and arrest situations, and providers may offer too many or medically inappropriate choices in efforts to honor patient autonomy. In addition, patients and family members may poorly understand DNRs. 12 People without sufficient knowledge or experience in healthcare may not fully comprehend the risk and benefits of various treatments and procedures.
To be medically effective, resuscitation may need to be provided in a bundle, not in an a la carte format. Dumot et al. compared patients who received limited advanced cardiac life support (ACLS) to those who received full ACLS. 13 They found that 23% of patients who received full ACLS (104 out of 445) survived to hospital discharge, while none of the patients with limited ACLS survived (0 out of 37). Berger 4 and Sanders et al. 6 have suggested that discouraging partial DNRs may promote more accurate and comprehensive advance care planning. Berger also proposed shifting from intervention-oriented care to goal-oriented care with a model order that addresses treatment of prearrest situations. This model contains the following five elements: incorporating a patient's goals of care; providing for patient refusal of specific treatments; allowing for physician discretion; reconciling requests for specific treatments with care goals; and being readily interpretable. 4
Yet clearly, some patients may desire and derive a survival benefit from emergency treatments before an arrest, for example, vasopressors for hypotension or noninvasive positive pressure ventilation for respiratory failure. Ensuring that patients who desire and might benefit from these life-saving therapies receive them is a legitimate medical goal. Our study supports partial DNRs as a means to improve the likelihood that patients receive this wanted care, as well as possibly decreasing the likelihood that they will be denied prearrest treatments compared to patients with full DNRs.
However, we still found our respondents would not perform nonarrest emergency procedures even in the presence of a DNR with an AEP order 52.3 to 72.1% and 59.1 to 80.9% of the time in cases 1 and 3, respectively. Our findings are consistent with other studies that demonstrate DNRs may influence decision making in nonarrest situations, but expand this influence to partial DNRs as well as full DNRs.3,14
To our knowledge, this is also the first attempt to study the impact, if any, that training and clinical experience play in making medical decisions regarding both prearrest and arrest treatments for patients with DNRs. We found a significant association between training level or clinical experience and a tendency to honor the DNR status. The association was strongest in the setting of full DNRs. For all nonarrest interventions, both nonarrest emergency and nonemergency, the effect of training was not statistically significant except for case 2, in which training level or clinical experience was positively associated with a tendency to honor the AEP order. Why were our less-experienced clinicians and students less likely to honor partial DNRs? Possibly, with training and experience, respondents gain prognostication and communication skills. Sullivan et al. demonstrated that students and residents did not have adequate education on end-of-life communication and felt unprepared to provide many key components of good care for the dying. 15 Historically, medical education about goals of care or end-of-life discussions may take place, if at all, within the preclerkship years in lecture halls, although recently other educational models have demonstrated effectiveness.16,17 However, even among experienced clinicians, self-reported confidence in the ability to discuss code status with patients is low. 14
There are several limitations of this study. First, this is a single-center survey. Therefore, our findings may have limited generalizability. Second, the hypothetical cases may differ from real world-experiences. Third, subjects had limited information about the patient's goals of care or treatment preferences other than their resuscitation code status, DNR or partial DNR. However, in the real world, a resuscitation team may often have no readily available information about a patient's goals of care or treatment preferences other than their resuscitation code status. Even if the family is available, it may be difficult to clarify the patient's preference due to the urgent nature of the situation. Finally, our subjects may have had different assumptions about patient prognosis due to the difference of age and disease among the cases, and that may have affected subjects' intent to provide medical interventions. 9 However, to prevent cognitive bias, or anchoring, each case was described either in the presence or absence of AEP, but not both.
In conclusion, our study showed that partial DNRs, similar to standard DNRs, might affect medical decision making in both prearrest and arrest situations. Partial DNRs increased the likelihood that our respondents would provide treatments in nonarrest situations, but also increased the risk that they would provide resuscitation in arrest situations. Neither partial nor full DNRs can communicate complex end-of-life care plans and the shared medical decision making that ideally lead to the development of these plans. Further research to confirm these findings and the potential risks and benefits of partial DNRs is needed. These findings suggest an ongoing need to develop and validate better means of incorporating patients' medically achievable goals of care into orders that more faithfully guide care for both prearrest and arrest situations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.