
Abstract
Abstract
Background:
Haloperidol is widely prescribed as an antiemetic in patients receiving palliative care, but there is limited evidence to support and refine its use.
Objective:
To explore the immediate and short-term net clinical effects of haloperidol when treating nausea and/or vomiting in palliative care patients.
Design:
A prospective, multicenter, consecutive case series.
Setting/Subjects:
Twenty-two sites, five countries: consultative, ambulatory, and inpatient services.
Measurements:
When haloperidol was started in routine care as an antiemetic, data were collected at three time points: baseline; 48 hours (benefits); day seven (harms). Clinical effects were assessed using the National Cancer Institute's Common Terminology Criteria for Adverse Events (NCI CTCAE).
Results:
Data were collected (May 2014–March 2016) from 150 patients: 61% male; 86% with cancer; mean age 72 (standard deviation 11) years and median Australian-modified Karnofsky Performance Scale 50 (range 10–90). At baseline, nausea was moderate (88; 62%) or severe (11; 8%); 145 patients reported vomiting, with a baseline NCI CTCAE vomiting score of 1.0. The median (range) dose of haloperidol was 1.5 mg/24 hours (0.5–5 mg/24 hours) given orally or parenterally. Five patients (3%) died before further data collection. At 48 hours, 114 patients (79%) had complete resolution of their nausea and vomiting, with greater benefit seen in the resolution of nausea than vomiting. At day seven, 37 (26%) patients had a total of 62 mild/moderate harms including constipation 25 (40%); dry mouth 13 (21%); and somnolence 12 (19%).
Conclusions:
Haloperidol as an antiemetic provided rapid net clinical benefit with low-grade, short-term harms.
Introduction
N
Haloperidol is commonly prescribed for nausea, vomiting, and delirium in palliative care. 4 It is a butyrophenone derivative with potent D2 receptor antagonism. A systematic review concluded that there is insufficient evidence from published randomized controlled trials (RCTs) to determine the effectiveness of haloperidol for nausea and vomiting in palliative care. 3
An international collaborative was established in 2011 to address the need to improve the evidence base for clinical prescribing in palliative care by undertaking phase IV (pharmacovigilance) studies in palliative care (RAPID pharmacovigilance program). 5 The program collects data documenting the net clinical effects of medications frequently used to treat common symptoms experienced by patients in the hospice/palliative care setting. Data are collected prospectively in a predetermined format when the medication is commenced in routine clinical care for an agreed indication. The initiative has published several studies on various drugs and indications to date.6–8 This study aims to describe the short-term net clinical effects of haloperidol when used to treat nausea and/or vomiting in patients in hospice/palliative care programs.
Methods
Comprehensive details of the methods used in the RAPID pharmacovigilance program have been described previously.5–8 Twenty-two sites participated across five countries between May 2014 and March 2016. Data were collected for consecutive patients started on haloperidol for nausea and/or vomiting as part of routine clinical care. Nonidentifying (and nonreidentifiable) demographic and clinical data were entered onto a secure website (www.caresearch.com.au) customized for this study.
Nausea was graded by clinicians using verbal descriptors (none; mild; moderate; or severe). The severity of vomiting and short-term harms was assessed using the validated National Cancer Institute's Common Terminology Criteria for Adverse Events (NCI CTCAE).9,10 Overall benefit was defined as a one-point reduction over baseline in the NCI CTCAE scale for vomiting. For nausea, a benefit was described as an improvement from the verbal grading of nausea (for example, severe to moderate, moderate to mild, mild to none). Data for benefits were recorded at 48 hours after starting haloperidol.
A selection of symptoms reflecting harms were assessed at baseline and seven days later. These adverse symptoms had been identified from the literature as haloperidol-related harms. 11 Harms were attributed to haloperidol if the NCI CTCAE criteria score was greater than a baseline measurement at or before day seven for that individual participant. When harms were rated as three or greater on the NCI CTCAE criteria, data were also entered onto the modified Naranjo Adverse Reaction Probability Scale. 12 This is a questionnaire designed to determine whether reported harms are likely to be due the drug itself or other factors. On the occurrence of harms, clinicians were asked to record their responses in the following categories: (1) no change in medication; (2) medication ceased; (3) dose reduced; or (4) dose increased. There was also the ability to note whether another medication was introduced.
Descriptive statistics are used in this study, with categorical variables summarized as frequency and percentages, and continuous variables with mean, standard deviation (SD), median, and range.
Given that this study was capturing de-identified data prospectively about routine clinical care where a clinician had already made a decision to commence haloperidol for nausea and/or vomiting, most sites obtained a waiver from their Human Research Ethics Committee, or the study was approved as a low and negligible risk study.
Results
The clinical and demographic data of the 150 study patients are shown in Table 1. Participating sites were drawn from consultative services, ambulatory clinics and specialist inpatient hospice/palliative care units, reflecting the scope of current specialist palliative care practices in the participating countries. In this study, the majority of participants (86%) had cancer. The average age was 71.8 years old (SD 11.1; median 72; range 42–96; n = 144). The majority of participants had advanced metastatic cancer as their primary life-limiting illness, and there were a number of underlying causes of nausea and vomiting identified at baseline (Table 1). Additionally, there were a number of additional symptoms identified at baseline; constipation (n = 53), somnolence (n = 46), and dry mouth (n = 13; Table 2). The median Australian-modified Karnofsky Performance Scale 13 was 50, indicating that patients required “considerable assistance and frequent medical care.” Again there was wide variation (10–90).
CNS, central nervous system.
Patient could have more than one baseline symptom.
The mean baseline NCI CTCAE vomiting score was 0.8 (SD 1.0; median 0). Of the 150 participants, one was commenced on haloperidol for the control of vomiting alone, 66 for nausea alone, and 83 for both nausea and vomiting. At baseline, 142 of the 149 participants who had been experiencing nausea were symptomatic at the time, and graded the severity of their nausea using a verbal nausea descriptors; mild (n = 43), moderate (n = 88), and severe (n = 11). Other baseline symptoms that were prospectively assessed as potential harms are shown in Table 2.
Patients received an average dose of 1.7 mg of haloperidol per 24 hours (SD 0.93; median, 1.5 mg; range, 0.5–5.0 mg) in parenteral or oral preparations.
Vomiting
After starting haloperidol, five patients died before the 48 hour data collection time point. Of 145 evaluable participants, 57 (39%) reported ≥1 point reduction in vomiting score by 48 hours, 49 (86%) of whom had total resolution of vomiting (Table 3).
0, none; 1, 1–2 episodes (separated by five minutes) in 24 hours; 2, 3–5 episodes (separated by five minutes) in 24 hours; 3, ≥6 episodes (separated by five minutes) in 24 hours; tube feeding, total parenteral nutrition (TPN) or hospitalization indicated; 4, life-threatening consequences; urgent intervention indicated; 5, death.
Grey boxes denote no change between baseline and measurement of outcomes.
NCI CTC AE, National Cancer Institute Common Toxicity Criteria Adverse Events—vomiting scale; MD, missing data.
Nausea
Improved nausea was reported in 105 patients (70%) 48 hours after starting haloperidol (Table 4).
Grey boxes denote no change between baseline and measurement of outcomes.
NR, no response.
Harms
Table 5 shows symptoms that are considered as potential harms from the treatment with haloperidol and the clinical responses that were conducted to address those symptoms. Harm in this study was defined as a one-point increase from baseline in NCI CTCAE criteria for the relevant symptom. Thirty-seven participants (25%) reported one or more harms at or before day seven (n = 62). Frequently reported harms were constipation (15/150; 10%) dry mouth (13/150; 9%), and somnolence (12/150;8%). All reported harms were graded two or less, except one report of delirium, which was graded as three, for which the Naranjo Adverse Reaction Probability Scale was not completed.
Grey boxes refer to symptoms being present.
NA, not applicable.
Most harms that were reported resulted in no change in haloperidol medication (46/62, 74%), even where there was a lack of benefit (35/62, 56%) (Table 5). Where present, prescribing responses included medication cessation (10/62, 16%), dose reduction (5/62; 8%), or dose increase (1/62, 1.6%). Clinical benefit for nausea and/or vomiting and no harms (net benefit) was seen in 54 (37%) patients (Table 6).
CI, confidence interval.
Discussion
This study found that haloperidol was effective in treating nausea and vomiting, with three in four patients experiencing some benefit within 48 hours and one-third of patients experiencing benefits with no harms. The effectiveness and tolerability of haloperidol when used as an antiemetic as described in the literature are consistent with these findings. A meta-analysis in 2004 found strong evidence for haloperidol as an effective antiemetic for nausea and vomiting in the post-operative setting and for various gastrointestinal disorders, with minimal toxicity. 15 Similarly, a single arm, observational study in palliative care patients found two-thirds of patients commenced on haloperidol experienced some symptomatic benefit. 16 Recently published guidelines support haloperidol's use in the palliative care setting. 17
In this study, one in four patients reported short-term harms, almost all of which were mild in severity (Tables 5 and 6). The most commonly reported harms were constipation, dry mouth, and somnolence (Table 5). Of the reported harms, only one in four resulted in a clinical intervention such as dose reduction or cessation, while the remainder continued on the same dose. This might indicate that the improvement in nausea and vomiting resulted in a net clinical benefit by outweighing these low-grade harms. However, this might also represent potential missed opportunities to treatment modifications once started even in the face of harms, especially as some patients experienced harm without benefit.
Strengths
Using a multicenter, multinational, multisetting prospective design, this study helps to understand the real world clinical performance of haloperidol when prescribed for nausea and/or vomiting in patients receiving palliative care. At present, there is no published high quality evidence to support the use of haloperidol in this setting.
This study treated nausea and vomiting as distinct symptoms, and collected data for each from all participants using designated scales. This is in contrast to previous studies in palliative care where nausea and vomiting were treated as one problem. 18 Although commonly occurring together, some patients experience these symptoms independently at varying degrees (Fig. 1).
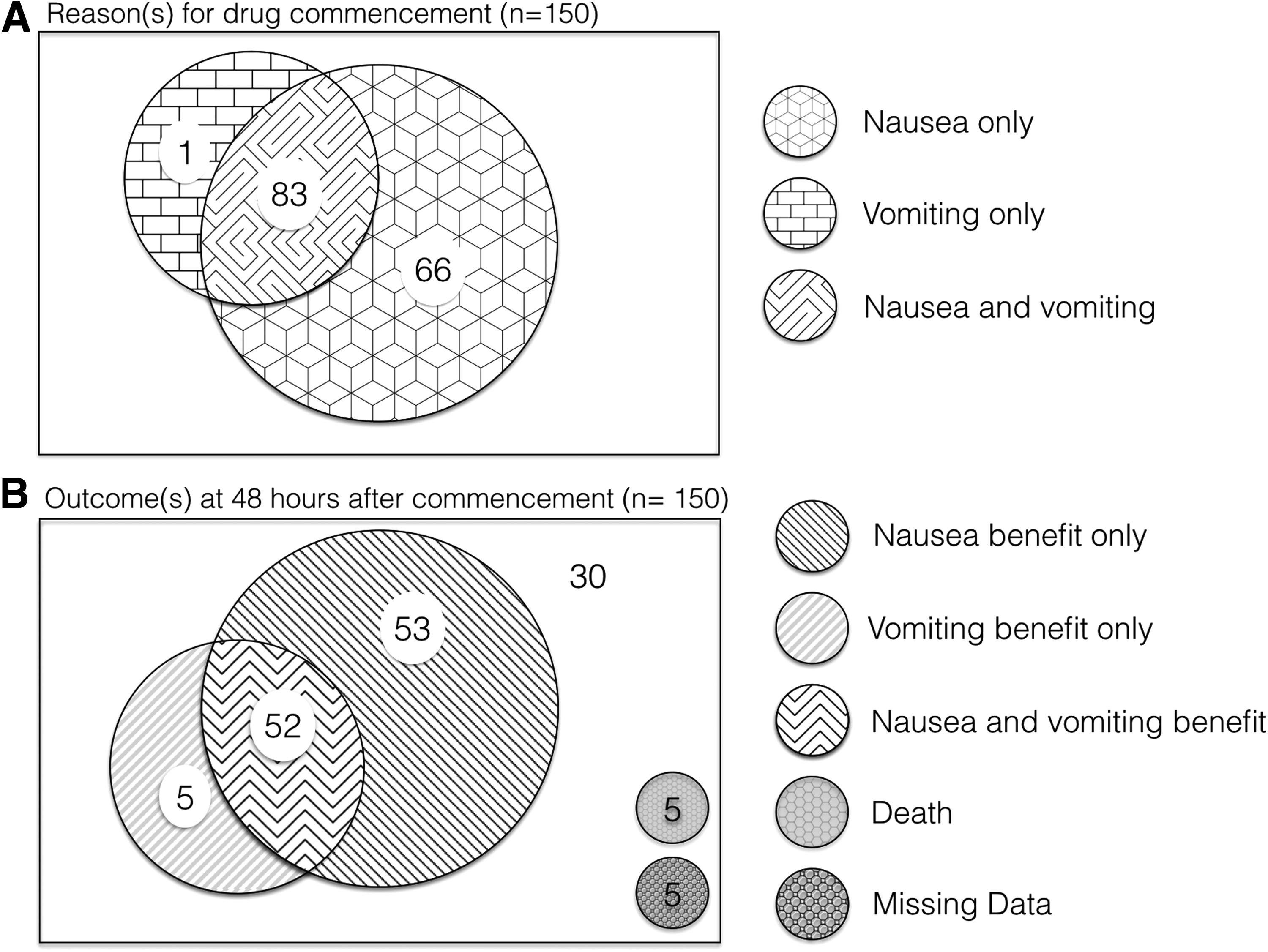
Representation of reasons and outcomes of the use of haloperidol for nausea and vomiting in hospice/palliative care.
Limitations
Seventeen participants included in the study were prescribed other antiemetics at the time of commencing haloperidol. It is not possible to assess whether reported benefits were the result of haloperidol alone, or due to the combination with other antiemetics. This may be significant as one study observing haloperidol used in post-operative nausea and vomiting found a synergistic benefit when haloperidol was used in combination with ondansetron. 19
Data on reported harms were collected at baseline and up to seven days. While this short time frame allows for a rapid collection of data and provides information regarding short-term harms, it was unable to quantify harms that develop over a longer period of time such as tardive dyskinesia. 20
There is no gold standard for measuring nausea or vomiting in the palliative care setting. 21 The National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) is a tool widely used in outcome measures and is considered a standard in cancer clinical trials despite lack of validation. 22 Further recent work has been done as these tools were being prepared for electronic patient reported outcomes.10,23
Clinical implications
Haloperidol appears to provide symptomatic benefit in both nausea and vomiting resulting from a variety of underlying causes in patients receiving palliative care. Most patients who reported benefit within two days had complete resolution of their symptoms. Haloperidol was well tolerated with approximately one quarter of patients experiencing side effects from the medication within one week, the vast majority of which were reported as mild in severity. Our data also suggest again a reluctance to stop prescription of medications that are causing harm without benefit. Clinicians need to be vigilant and systematic about reducing exposure to medication that is causing net harm, especially with no perceived benefit.
To date, there have been no fully powered RCTs that evaluate the use of haloperidol for nausea and vomiting in patients receiving palliative care. By providing data from a larger number of patients in the palliative care setting, this study contributes stronger evidence of the net effectiveness of this medication when used in routine clinical palliative care, which can guide practice and future research.
Future direction
There is a recently completed, randomized, open label phase III study of haloperidol compared to a pharmacological approach based on the dominant mechanism of nausea (ACTRN12610000481077), which is ready for publication. There is currently a randomized, controlled, double-blinded phase III study (ACTRN12615000177550) drawing toward completion that compares haloperidol with methotrimeprazine for the treatment of nausea related to cancer and nausea not related to anticancer therapy. It is hoped that this will help to further inform practice for symptom control in this setting.
There is no agreed outcome measure for nausea and vomiting in the palliative care setting. 21 This is an ongoing challenge for research into these symptoms. This study shows that the NCI CTCAE criteria provided a useful measure of change in symptoms. The tool is able to be used in clinical and research settings and allows nausea and vomiting to be assessed separately.
Conclusion
This study observed a positive overall clinical benefit when haloperidol was used for nausea and vomiting as part of routine symptom management in palliative care. Although short-term harms occur, they are mostly mild in severity. Clinicians should be alert to net harm and de-prescribe when there is little or no clinical benefit or when the harm outweighs the therapeutic gain. These findings contribute to the body of evidence supporting the current use of haloperidol as an antinausea and antiemetic agent in the palliative care setting.
Acknowledgment
This study was funded as part of the Palliative Care Clinical Studies Collaborative (PaCCSC) by the Commonwealth Department of Health as part of the National Palliative Care Program. The funder had no control over design, analysis, or reporting of the study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.