
Abstract
Abstract
Background:
The purpose of medication management in the last days of life is to optimize patient's comfort. Little is known about the medication use in the days before death and how this relates to the care setting.
Objective:
To describe medication use in the last week of life for patients dying in hospital, hospice, and home settings in the Netherlands.
Design:
Retrospective chart review study.
Setting:
A convenience sample of patient records from the three settings in three different regions in the Netherlands that cover more than half the country.
Measurements:
Information about medication use in the last week of life of patients who ultimately died an expected death was registered, including type of medication, start and if applicable stop dates, administration routes, and doses.
Results:
One hundred seventy-nine records were analyzed. Medications most frequently used in the last week of life were analgesics (n = 168, 94.1%) and psycholeptics (n = 150, 84.7%), in particular by hospice patients. The mean number of medications used per patient was nine during day 7 before death and six on the day of dying. On the day of death, 48 (26.8%) patients used a preventive medication. This percentage was highest for patients dying in the hospital or at home.
Conclusions:
Patients who die an expected death receive many medications in the last week of life, part of which are preventive medications. Medication management in patients' final days of life can be improved, especially in the hospital and home setting.
Introduction
M
Research that explores end-of-life medication prescribing patterns has particularly focused on the use of unnecessary futile medications, such as lipid-lowering and antiosteoporosis agents.6–10 They demonstrated that many of these medications are continued until the very end of life. Recently, an observational analysis of medication records from patients with a life expectancy of less than one year revealed that these patients use on average more than 10 medications, with a significant amount of PIMs. 11
LeBlanc et al. have reviewed the literature on studies of medications used at the end of life of patients with cancer and a limited life expectancy. 4 The six included studies showed that as patients approach death, the number of medications they take usually increases, due to an increase of medications aimed at the alleviation of symptoms combined with the continuation of medications for comorbid diseases. All studies focused on medications taken by patients who received care in hospices or from specialized palliative care services. Recently, another multicenter study in hospices underlined the finding of increased symptom-specific medications and continuation of medications for comorbid diseases at the end of life. 12 Hospice care is seen as an example for best practice care at the end of life. 13 The ultimate goal of hospice care is to enable patients to be comfortable. Consequently, medications to treat symptoms will ideally have much more weight than medications with the aim to treat or prevent diseases.
There is scarce information on the use of medications by patients in their last days of life in hospital and in home care settings. The only three studies that assessed medication use in a general hospital setting during the final days showed that many patients receive PIMs, and even medications that are clinically definitely futile in the last days of life.5,14,15 To our knowledge, there have been no studies done in home care settings.
It is unknown whether the number and type of medications in patients with a limited life expectancy depend on the place where end-of-life care is provided. The aim of this study was to describe the medication prescriptions for patients dying in hospice, hospital, and home care settings in the Netherlands.
Methods
Study design
This study consisted of a retrospective chart review within the MEDIcation management in the LAST phase of life (MEDILAST) project. MEDILAST is a multicenter mixed-methods research project with the aim of understanding current medication use in the last phase of life. The project is carried out by VU University Medical Center, Erasmus University Medical Center, and Radboud University Medical Center in the Netherlands.
Chart review
We selected a convenience sample of medical records of patients who had died in hospice, in hospital, or at home by asking physicians to select their two to three most recent cases of patients who had died expectedly from a chronic condition. We aimed at including 3 × 60 medical records in the regions of Amsterdam, Rotterdam, and Nijmegen, respectively, and in each region, 3 × 20 medical records from the hospice, hospital, and home setting, respectively. For the hospital setting, we included records from patients who had died at geriatrics, neurology, oncology, cardiology, or pulmonology departments in a peripheral or academic hospital. In each region, the hospice setting included one high care hospice, where a physician with training in palliative care is at all times available for consultation. Finally, family physician practices were approached by telephone. Following acceptance to participate in the study, three physician researchers (J.J.A., E.C.T.G., and M.K.D.) visited the individual practices and clinical departments to collect the data.
A structured electronic form (MS Access 2013) was used to retrieve the information from the medical records. Demographics included place of death, age at the time of death, and diagnoses. Information about medication use in the last week of life was registered, which included medication generic names, start and stop dates, administration routes, and doses. The physician's notes were manually screened for information about the decision making on medication use. We reviewed the guidelines for data collection from medical records as developed by Jansen et al. 16
The Medical Ethics Review Committee from the VU University Medical Center approved the study protocol. Thereafter, approval from the board of directors or relevant authority was obtained before data collection in all other participating centers.
Statistical analysis
Medications were coded using the World Health Organization Center for Drug Statistics Methodology's Anatomical Therapeutic Chemical (ATC) classification at the level of therapeutic subgroup (second), pharmacological subgroup (third), and chemical substance (fifth). 17 Descriptive statistics were used to describe the frequency of medication prescription per setting. The Appendix lists the chemical substances classified as preventive medications in this analysis; this classification was agreed by our research group based on patient comorbidities and the dosages reported (i.e., low-dose low-molecular-weight heparin). If it was not clear whether or not a medication was prescribed for preventive reasons, for example, antihypertensives that may be used not only to prevent the complications of high blood pressure but also to relieve symptoms of dyspnea, we did not classify this as a preventive medication. Statistical analyses were conducted using IBM SPSS Statistics 21 (IBM Corporation, 2012). Two-sided p-values <0.05 were considered statistically significant.
Results
A total of 180 medical records were reviewed in this study. One patient died within 24 hours of admission to a hospice and was not included in the analysis. Table 1 shows the characteristics of patients per setting. Hospital patients (n = 59, 32.8%) comprised the wards of geriatrics (n = 8, 13.5%), oncology (n = 16, 27.1%), neurology (n = 12, 20.3%), cardiology (n = 12, 20.3%), and pulmonology (n = 11, 18.6%); participating centers included three academic and seven peripheral hospitals. In addition, 3 high care hospices (n = 61, 33.9%) and 32 primary care practices, which contributed with two to three medical records each (n = 59, 32.8%), were included.
One-way ANOVA.
Chi-squared.
SD, standard deviation.
Patients' age at the time of death ranged from 40 to 103 years. Most patients had a malignancy (n = 109) with larger proportions in the home care and hospice settings compared to the hospital setting. Most cancer diagnoses involved malignancies of the bronchus/lung (n = 29) or gastrointestinal tract (n = 15). Noncancer diagnoses included heart failure (n = 25), cerebrovascular accident (n = 12), chronic obstructive pulmonary disease (n = 9), ischemic heart disease (n = 3), and other conditions (n = 21).
Patients used 304 different chemical substances corresponding to 113 pharmacological subgroups and 61 therapeutic subgroups. During the last week of life, analgesics (e.g., morphine, fentanyl, and paracetamol) were used by 168 (94.1%) patients, psycholeptics (e.g., midazolam, haloperidol, and temazepam) by 150 (84.7%) patients, medications for acid-related disorders (e.g., pantoprazole, omeprazole, and esomeprazole) by 110 (62.1%) patients, medications for constipation (e.g., macrogol, lactulose, and sodium docusate) by 100 (56.4%) patients, and antithrombotic agents (e.g., nadroparin, acetylsalicylic acid, and acenocoumarol) by 87 (49.15%) patients.
The five medications that were most frequently started in the last week of life were opioids (n = 66, 80.5%), hypnotics and sedatives (n = 63, 52.5%), antipsychotics (n = 47, 26.3%), anxiolytics (n = 28, 15.6%), and diuretics (n = 22, 12.3%). The median (interquartile range [IQR]) number of days before death at which these new prescriptions were started was 2 (1–5) days for opioids, 2 (1–4.25) days for hypnotics and sedatives, 3 (2–5) days for antipsychotics, 4.5 (2.5–6) days for anxiolytics, and 4 (2–7) days for diuretics. Figure 1 shows the numbers of patients using medications that were frequently started in the last week of life.
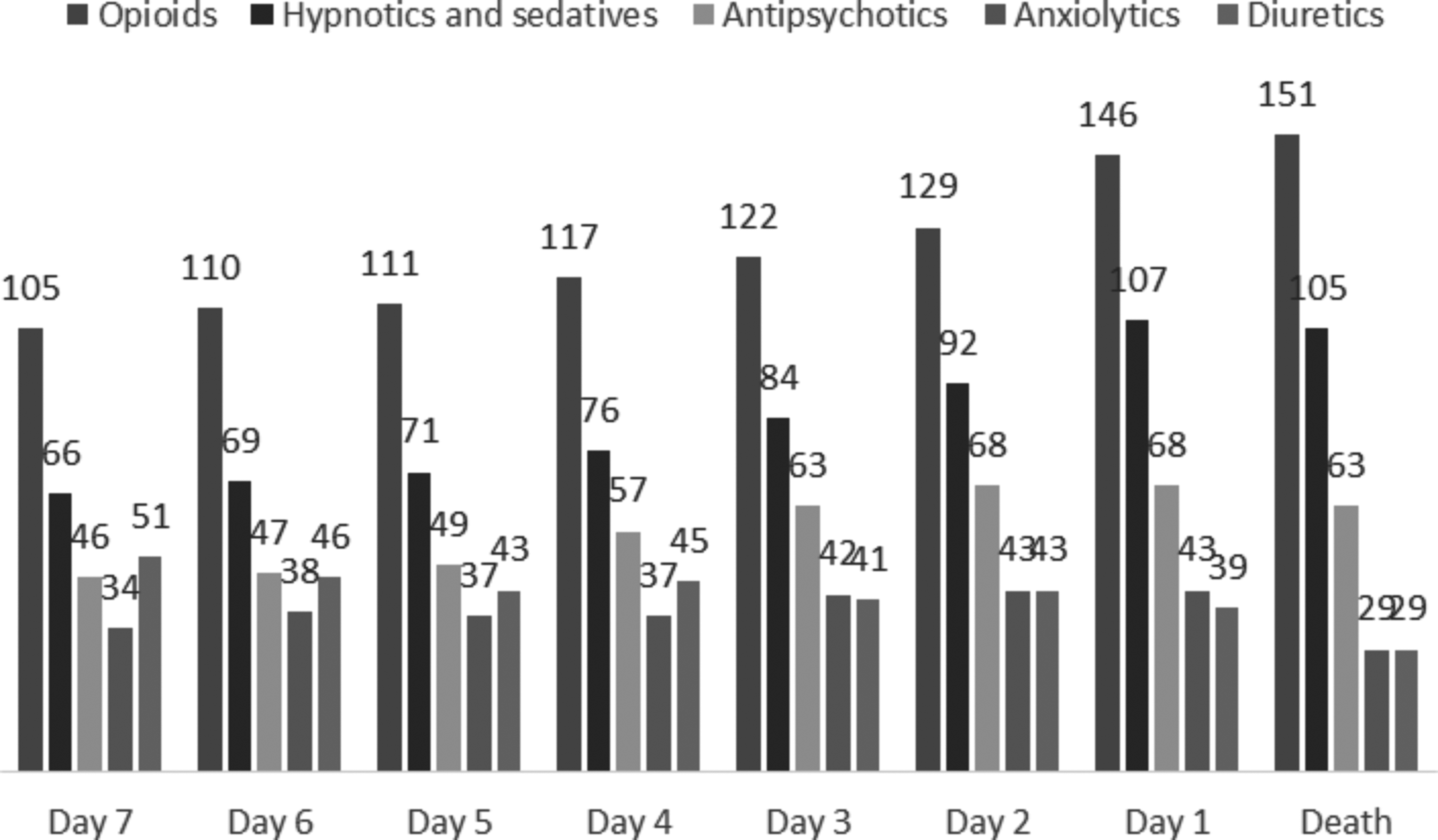
Number of patients using frequently started medications in the last week of life.
The five medications that were most frequently stopped in the last week of life were medications for peptic ulcer and gastro-esophageal reflux disease (n = 64, 35.8%), antithrombotic agents (n = 50, 27.9%), nonopioid analgesics (n = 48, 26.8%), medications for constipation (n = 46, 25.7%), and diuretics (n = 38, 21.2%). The median (IQR) number of days before death at which these prescriptions were stopped was 2 (1–4) for medications for peptic ulcer and gastroesophageal reflux disease, 2 (1–4) for antithrombotic agents, 1 (1–3.75) for nonopioid analgesics, 3 (1–4) for medications for constipation, and 2 (1–6) for diuretics. Figure 2 shows the use of the five most frequently stopped medications in the last week of life.
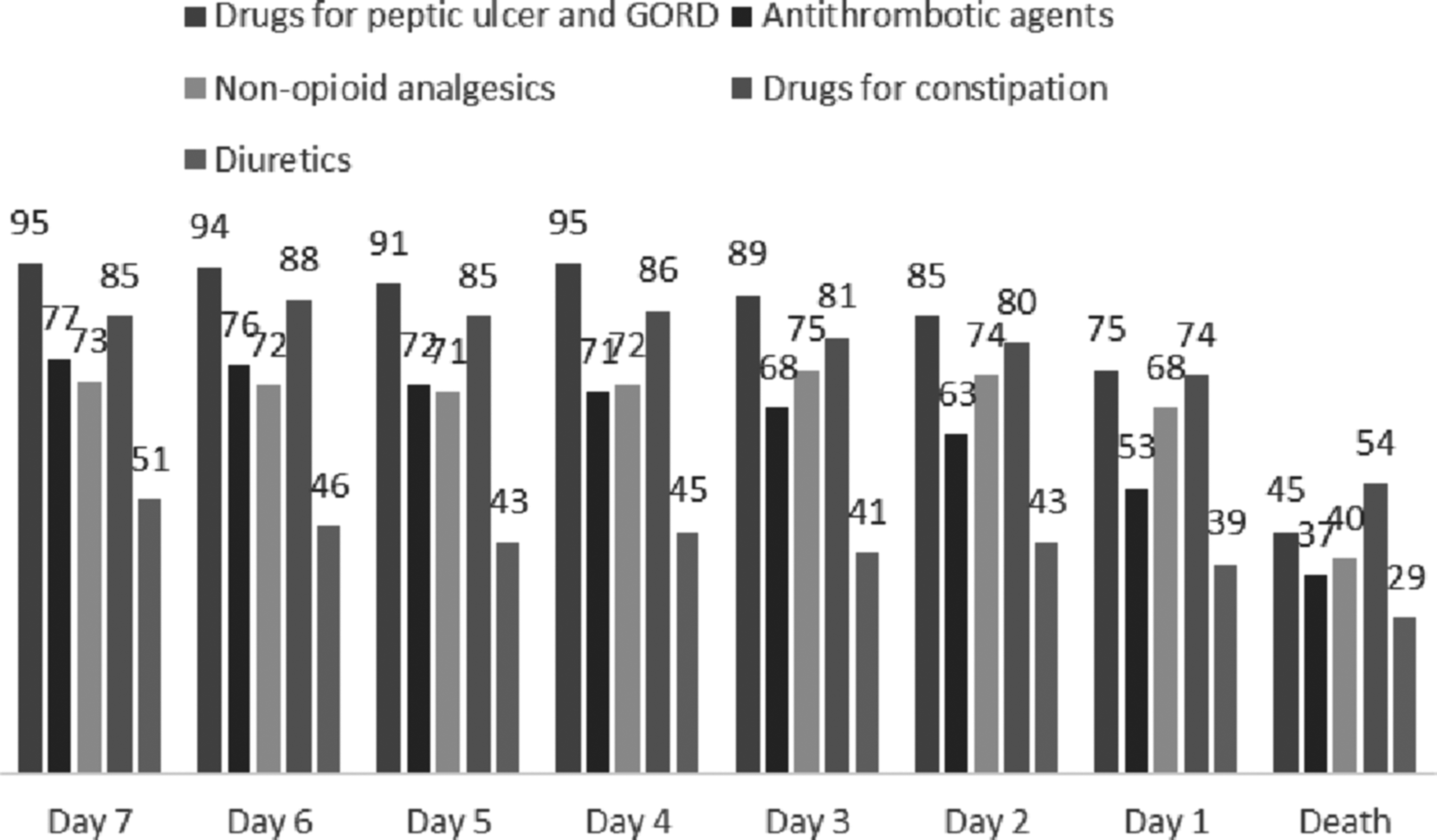
Number of patients using frequently stopped medications in the last week of life.
Figure 3 shows the numbers of patients receiving preventive medications in the last week of life. The preventive medications most frequently used were antithrombotic agents that were used by 87 (48.6%) patients, vitamins by 36 (20.1%) patients, cholesterol-lowering medications by 16 (8.9%) patients, calcium by 10 (5.5%) patients, and iron supplements by 5 (2.7%) patients. Although there was a tendency to stop preventive medications in the last week of life, 48 (26.8%) patients still used preventive medication on the last day of life.

Number of patients using preventive medication in the last week of life by setting.
Table 2 shows the differences in medication use between settings in the last week of life for the 15 most frequently used pharmacological subgroups. There were statistically significant differences between settings for hypnotics, sedatives and anxiolytics, nonopioid analgesics and antipyretics, medications for constipation, antithrombotic agents, diuretics, antihypertensive agents, antibiotics, and belladonna derivatives. These differences were mostly related to the fact that the hospice setting differed from both other settings. Medications used for symptom control (for instance hypnotics and sedatives; nonopioid pain medication) tended to be used in more patients in the hospice setting, whereas predominantly preventive medications (for instance, antithrombotics and statins) tended to be used more in both the hospital and home care setting.
Statistically significant at α 0.05.
Gastroesophageal reflux disease.
High-ceiling diuretics + potassium-sparing agents.
Betablockers, angiotensin-converting enzyme inhibitors, vasodilators.
Inhaled adrenergics, other drugs for obstructive airway disease.
Beta-lactam antibacterials, quinolones.
The median number of medications used per patient in the last week of life was nine from day 7 to 2 before death, eight on day 1 before death, and six on the date of death. In the home setting, the median number of medications per patient was seven during the entire week. Overall, a larger variation in the median number of medications used per patient per day was observed in the hospital setting (seven on day 7 and six before death, five on day 5 before death, seven on day 4 before death, five on day 3 before death, six on day 2 before death, and three 1 day before death and on the day of death), while no variation was seen in the home setting. The tendency in both hospice and hospital settings is a reduction in the median number of medications per patient.
When comparing settings with regard to medications that were frequently started in the last week of life, it was found that diuretics were started more often in the hospital (18 patients, 38.3%) than in the home (3 patients, 7.5%) and hospice (1 patients, 2.1%) setting (p < 0.001). Although not reaching statistical significance, opioids were started more often in the hospice (12 patients, 92.3%) and hospital (37 patients, 86%) than in the home (17 patients, 65.4%) setting (p = 0.056).
When comparing settings with regard to medications frequently stopped in the last week of life, it was found that antithrombotic agents were stopped more frequently in the hospital (29 patients, 49.2%) than in the home (13 patients, 21.3%) and hospice setting (8 patients, 13.6%) (p < 0.001); this was also the case for diuretics, which were stopped more often in the hospital setting (20 patients, 33.9%) when compared to the home (9 patients, 14.8%) and hospice setting (9 patients, 15.3%).
The medications most frequently continued until death in the home and hospice setting were opioids (48 and 54), hypnotics and sedatives (35 and 46), and antipsychotics (25 and 24). In the hospital setting, these were opioids (49), hypnotics and sedatives (25), and antithrombotic agents (14), respectively.
The comparison between settings of medications classified as preventive is shown in Table 3. The use of thromboprophylaxis, vitamins, and cholesterol-lowering medications was consistently lower in the hospice setting, but no differences were found in the use of calcium or iron supplements.
Statistically significant at α 0.05.
Discussion
This study showed that the number of medications patients used decreased in the final week of life, regardless of whether patients die at home, in a hospice, or a hospital. As could be expected, the number of medications aimed at the alleviation of symptoms, such as opioids and sedatives, increased in the final week. The percentage of patients using such symptom alleviators was the largest in hospices, followed by the home and hospital settings. In all three settings, some patients used preventive medications until the very last days of life, but this most often occurred in patients dying at home and in hospital: more than a third of these patients used one or more preventive medications on the day before their death.
The importance of adapting the use of medications to a patient's life expectancy is increasingly acknowledged. 4 In a Delphi study, palliative care clinicians from nine countries came to the consensus that, ideally, medications aimed at the alleviation of symptoms (opioids, benzodiazepines, antipsychotics, and antimuscarinics) should always and everywhere be available for dying patients. 18 In our study, we found that virtually all the patients in the hospice setting used morphine and sedatives, and in more than half of them, antipsychotics were used. In the home situation and in particular in the hospital, less patients received these medications. Antimuscarinics were not prescribed except for a few patients in the hospice. The added value of these medications to prevent death rattle is doubtful as suggested by the results of two placebo-controlled randomized trails, where no favorable effect of antimuscarinics was found.19,20
Another important reason for adapting medications for patients with a limited life expectancy is their futility: some medications have a lag time that exceeds the patient's expected life span and therefore might only do harm. 21 This applies primarily to preventive medications. For example, it has been proven that stopping statins in patients with an estimated life expectancy of less than one year is safe and may improve quality of life. 22 Our findings reveal that preventive medications are least often used by patients in the hospice, except for thromboprophylaxis. In the home setting and in hospital, on the other hand, more than 50% of the patients used one or more preventive medications in the week before death, including preventive medication other than thromboprophylaxis. For example, nearly a quarter of hospital patients used a statin one week before death. This finding also underlines that in the hospice medication management seems more appropriate and in line with intended care for patients in the last phase of life. 13
In total, almost 50% of the patients was administered thromboprophylaxis in the week before their death, which was often continued until death. In the most recent NICE guideline, it is advised to review decisions about thromboprophylaxis for patients at the end of life on a daily basis, taking into account the views of patients and their relatives, and the multidisciplinary team. 23 It seems that many physicians struggle with the question as to whether thromboprophylaxis should be prescribed to patients who only have a limited life expectancy, mainly due to the lack of studies demonstrating positive and negative effects. 24
Our study showed that some types of medication were started or continued in the last week of life for some patients, whereas they were stopped in others. Some of these medications have in the literature been classified as PIMs.4,5 Our findings underline the difficulty to categorize medications in the end of life as inappropriate. For example, diuretics can be considered to be PIMs when they are solely used as antihypertensives. However, they may relieve a patient's symptoms in case of dyspnea and not at all be inappropriate. It may therefore be better to follow a patient-centered approach rather than an explicit list of PIMs. 25 An exception should be long-term preventive medications, such as statins, which are medically futile anyway. 9
Our study had some limitations. First, the reasons for medication prescription were seldom described in the records. Therefore, we cannot draw conclusions about the intention of their administration. Second, we cannot rule out the possibility that medications have been discontinued in practice, without it being registered in the records. However, especially in hospice and hospital settings, it is common practice to administer all and only medications that are listed in the medical record to prevent any misunderstandings. Third, differences between settings could be accounted for the illness and stage of disease of patients, as well as for the background of the treating physician; however, the distinction between the two could not be established with our data.
Despite these limitations, our study demonstrates that the medication management in patients' final phase of life can be improved, especially in home care and hospital settings.
Footnotes
Acknowledgments
This research study was funded by a grant from the Dutch government (ZonMw 1151.0036). The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The authors would like to acknowledge the work of Dr. W.J.M. Dekkers whose thoughts and input contributed gratefully to this article. In addition, the authors wish to acknowledge all physicians who provided access to the patient records.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.