
Abstract
Abstract
Background:
Hospice in-person visits in the last week of life are critical to ensure quality of care. In 2016, The Centers for Medicare & Medicaid Services (CMS) introduced a Service Intensity Add-on (SIA) payment for in-person routine home care (RHC) visits by a registered nurse or social worker in the last 7 days of life.
Objectives:
The aim of the study was to examine visit patterns in the last week of life and provide SIA payment impact estimates.
Design/Measurements:
Hospice data from 42 volunteer hospice programs for the 6-year period of 2005–2010 were examined. The data included information on the type and duration of visits/other care, the staff discipline, and patient demographics, diagnoses, date of death, and care setting (home, assisted living, nursing home).
Results:
In their last week of life, 251,407 decedents received 2,818,695 visits during 1,352,638 RHC days. Forty-four percent of the decedents had at least one SIA-eligible visit (in-person direct care visit by a registered nurse (RN) or social worker (SW)); 6.6% had only phone contact, and 30.4% had no hospice contact. Rates of RHC days with SIA-eligible days varied considerably across hospices (31% to 60.9%). For the 86.3% decedents with any SIA-eligible visits, average SIA payment would have been $202.5 (Median = $177.2, inter quartile range [IQR] = $108.3-$275.6), which represents a 21.6% increase over the average regular RHC payments received during the last week of life.
Conclusions:
The relative size of the new SIA payment introduced by CMS has the potential to increase RN/SW visits and reduce disparities in visit patterns in the last week of life.
Introduction
I
Most hospice care is delivered in the form of routine home care (RHC) at their place of residence. Medicare pays for RHC using an all-inclusive daily rate, originally based on average visit patterns delivered by hospice providers updated annually. However, there are no visit requirements associated with RHC days, and it is up to the hospice provider to determine if visits are needed during any given RHC day.
Recent research has examined visits received by hospice beneficiaries in their last 2 days of life as an indirect measure of quality of care. Using FY2014 Medicare claims, Teno et al. showed that 12.3% of all Medicare beneficiaries at the RHC level of care received no professional staff visits in their last 2 days of life with large variations across hospice programs, interquartile variation from 3.2% (25th percentile) to 19.5% (75th percentile), race (12.0% for whites vs. 15.2% for blacks), and site of care (10.6% for those dying at home vs. 16.5% for those dying in nursing homes). 4
Starting in CY2016, the Centers for Medicare & Medicaid Services (CMS) implemented a Service Intensity Add-on (SIA) payment for in-person RHC visits by an RN or social worker in the last 7 days of life of the patient. This analysis provides a detailed study of visits received by hospice patients during their last 7 days of life before implementation of the SIA and the potential impact of SIA payments. Our analysis takes advantage of a rich data set with detailed visit data on all patients from 42 different hospice programs during the 2005–2010 period. Unlike currently available CMS visit data, our data differentiate nursing visits between RNs versus LPNs, which allow us to estimate how the SIA payment may contribute to reimbursements received by hospice providers.
Methods
A total of 42 hospice programs, with a combined total of 53 CMS certification numbers (CCNs), volunteered to provide us with all their visit data for 6 years, 2005–2010. Most programs (38) contributed data for all 6 years, one program for 4 years, two for 3 year, and one for 1 year. The providers were located across the country, (AL [2], AR, CA [2], CO, DE, FL [4], GA [4], ID, IL, KS [2], KY [4] MD, MA, MO, NY [8], NC, OH [4]] PA [2], UT, WI, and WY). Most operate in a single state, while a minority (2) had programs in multiple states. Patients were identified using a fabricated unique identifier. No patient personal information was retained except for a few demographic fields needed for the analysis. Institutional Review Board (IRB) approval was obtained from Brown University.
Visit and other care activity data measures
The data contained information for each visit or care activity related to each patient. These included in-person visits, phone calls, interdisciplinary team meetings, and administrative record keeping. Each record included the date, staff discipline, type of visit or care function, duration (in minutes), and level of care.
Care activity categories
Care activities were classified using the following hierarchical approach based on their degree of direct patient care involvement: (1) in-person visits qualifying for SIA payment (direct patient care provided by a registered nurse (RN) or social worker (SW)); (2) in-person visits not qualifying for SIA payment provided by staff other than an RN/SW); (3) in-person visits with no patient direct care/contact (including visits to confirm death, family/caregiver case conferences, funeral home visits, attendance at death and memorial services, and postdeath bereavement/condolence visits), (4) telephone contact, and (5) no direct contact (can include documentation and charting, deliveries of medications or durable medical devices, care planning meetings, or RHC days with no activity at all). This hierarchical classification of care activity was also used to classify RHC days based on their highest level of direct patient care involvement among visits received during a given day.
Staff disciplines
Staff members were classified into the following disciplines: RN, licensed practical nurse (LPN), SW, home health aide (HHA), Medical Doctor (MD), nurse practitioner (NP), chaplain, bereavement, skilled therapist, other (e.g., aroma, music, and pet therapists), and volunteers.
Hospice provider and patient characteristics
Hospice programs' organizational characteristics, obtained from the December 2010 CMS Provider of Services files, included time in operation (based on year of certification by CMS); facility type (freestanding or facility-based); ownership tax status (for-profit, not-for-profit, government); and provider location, including region and whether urban or rural. CMS hospice claims files were used to calculate the number of Medicare hospice decedents in 2010.
Patient demographic and other patient characteristics included age, gender, race, marital status, whether the person lived alone, residential setting (home, nursing facility, assisted living, other), principal diagnosis, and hospice admission and discharge dates for each hospice episode that we used to calculated length of stay (LOS).
Day-level analyses
To carry out our analyses, we used the date of death and the date of the visit/care activity, as documented, to classify each visit/care activity as associated with a specific day before death (0 indicating the day of death, 1 indicating one day before death, and so on). The unit of observation was each individual visit/care activity on a given day of the last 7 days of life for each patient.
Days were classified by their level of care as routine home care (RHC), continuous care (CC), general inpatient care (GIP), and inpatient respite care (IRC). Our analyses report the number of days of each level of care for context, but the focus of our study was on RHC days.
SIA reimbursement estimates
SIA reimbursements were estimated using the CMS payment rules implemented on 1/1/16 based on in-person RHC visits by an RN or SW in the last 7 days of life of the patient. The SIA payment equaled the CC average hourly rate, $39.37, multiplied by the hours of nursing/social work service (calculated in 15-minute increments with a minimum of 15 minutes and up to a maximum of 4 hours per day) each RHC day during the last seven days of life. We aggregated all SIA-eligible visit minutes during each RHC day, using 0 when total minutes were less than 15, and capping at 240 minutes (4 hours) whenever the total exceeded 240 minutes.
Results
During the 2005–2010 6-year period, 42 hospice programs (53 CCNs) in our study provided care to 313,778 decedents, who received hospice care for a total of 1,839,034 days during their last 7 days of life. Annual sample size ranged from 46,165 in 2005 to 57,291 in 2010. The total number of decedents per hospice program varied from 140 to 8,931, although several of the smaller numbers of decedents resulted from programs not contributing data for all years.
Figure 1 provides a breakdown of the number of decedents and hospice days by their level of care. Most decedents (80.1%, N = 251,407) received RHC at least one day during their last 7 days of life, with a total number of 1,352,638 RHC days comprising 73.5% of all hospice days. About a third of decedents (33.8%, N = 106,162) had some GIP days, comprising 22.3% (N = 409,985) of hospice decedent days of hospice care in their last 7 days of life.
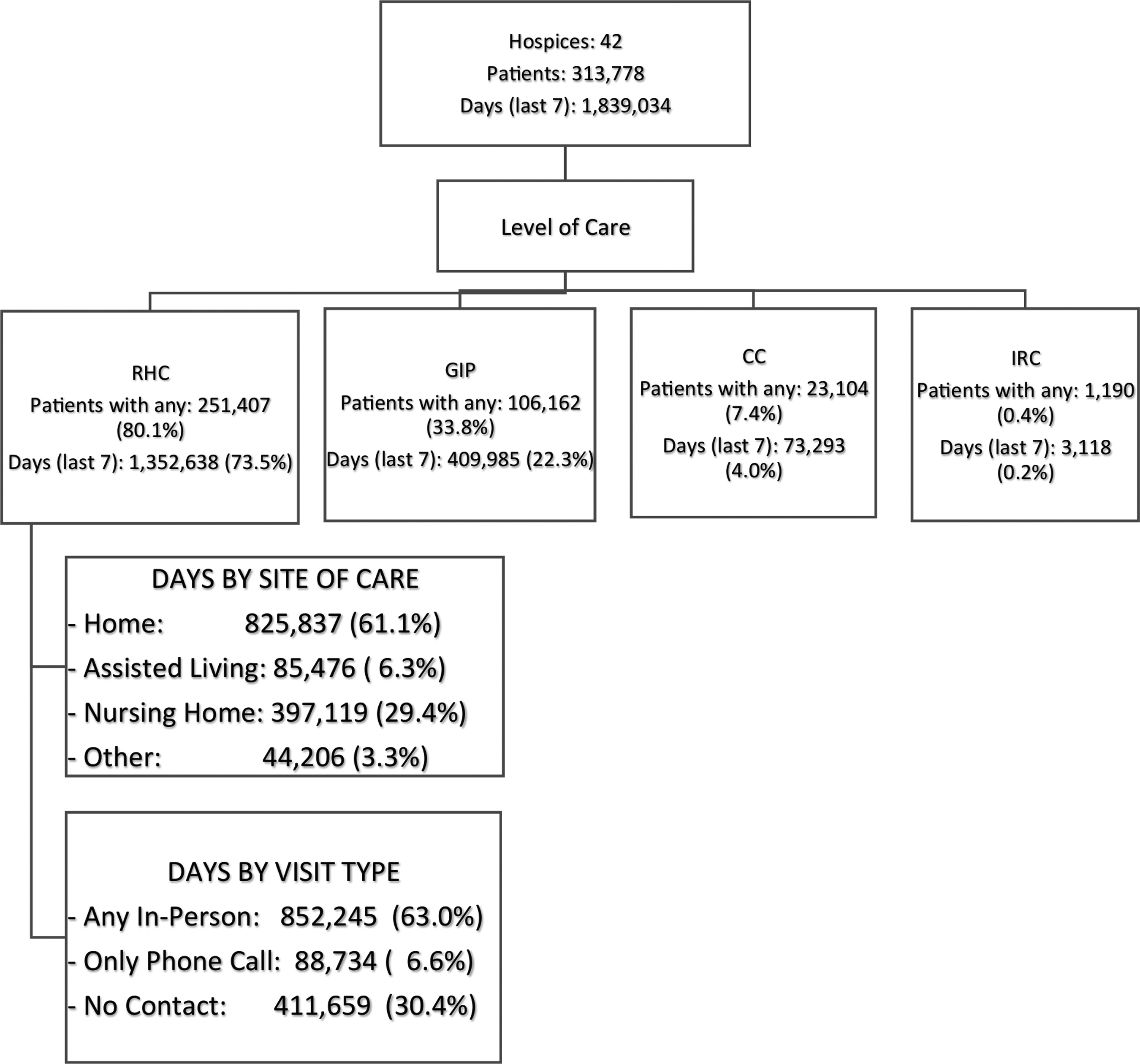
Number of hospice decedents and breakdown of days of care in the last 7 days of life for hospice programs participating in our study.
Just over seven per cent (7.4%, N = 23,104) decedents received some CC-level care with a share of 4.0% (N = 73,293) of the hospice days, and only 0.4% (N = 1,190) of decedents had any IRC days with a share of 0.2% (N = 3,118) of all hospice days. Most decedents received a single level of care during their last 7 days of life, but some received more than one level of care during these days: 59.1% (N = 186,103) had only RHC days and 18.7% (N = 58,716) had only GIP days, while 14.2% (N = 44,690) had RHC and GIP days, and 5.7% (N = 17,979) had RHC and CC days. The remaining 2% of decedents had just CC (0.9%, N = 2,803) or other combinations of levels of care.
Compared with the rest of CMS-certified providers in 2010, those that participated in our study, on average, care for a larger number of patients, have been in operation longer, include more with not-for-profit tax status, and are freestanding hospice programs (see Table 1). Regional and urban/rural distributions for study participants are not very different from nonparticipating hospices.
CCNs, CMS certification numbers; SD, standard deviation.
RHC days care activity
We first examined RHC days by classifying them according to the highest level of direct patient care received by the patient and/or family among all visits/care activities on a given day. Table 2 (last row) shows that of the 1,352,638 RHC days for 251,407 decedents in their last 7 days of life, in almost 44% of them (43.7%), the patient received at least one in-person visit that would qualify for SIA reimbursement. In close to a third of the RHC days (30.4%), the patients had no direct contact or no care activity at all.
CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; RHC, routine home care; SIA, Service Intensity Add-on.
Examination of the RHC days not qualifying for SIA payment revealed that in close to 20%, the patient received a visit that was not eligible for SIA (15.4%) or there was in-person activity that did not include direct patient care or contact (3.9%). In 6.6%, there was only phone contact with the patient or family member, and in 2.8%, care activity was only indirect (e.g., documentation, planning, and delivery of medications). In 27.6% of potential SIA-eligible RHC days, there was no contact or activity at all.
Comparing the highest level of direct patient care during RHC days by patient characteristics (Table 2) shows that across age groups, the main difference appears to be on the type of staff discipline delivering in-person direct care visits, with a slightly higher proportion of SIA visit days for the youngest decedents (45.3%, 0–64 years vs. 41.7%, 95–113 years) and more visits delivered by staff other than an RN or SW among the oldest decedents (17.3%, 95–113 years vs. 12.4%, 0–64 years). The youngest decedents also have a slightly higher rate of phone contact days (7.6%, 0–64 years vs. 6.1% 95–113 years).
There was little variation in RHC visit/care activity types related to gender, but there were larger differences across racial groups. African American decedents experienced a lower rate of RHC days with SIA-eligible visits (39.2% vs. 44.1% for whites and 42.3% or higher for the other racial groups) and a higher rate of days with only indirect or no contact (34.6% vs. 30% for whites and below 31% for the other racial groups). Hispanics also experienced lower rates of SIA-eligible visits (43.5% vs. 49.2% for non-Hispanics), but had a higher rate of visits by staff other than an RN or SW (15.7% vs. 11.8% for non-Hispanics) rather than by a higher rate of days without indirect/no contact as in the case of African Americans.
SIA-eligible RHC days were more prevalent among married decedents than among decedents with other marital status (45.6% vs. around 42% for singles, divorced or widowers). In contrast, a lower proportion of SIA-eligible RHC days compared with days with indirect/no contact was observed for patients who lived alone.
On examination of RHC days related to principal diagnosis, patients with cancer and kidney disease had the highest rates of SIA-eligible RHC days (close to 45%). Patients with dementia had the lowest rates at 41.3% of RHC days and had the highest rates of non-SIA-eligible visits (17.4% vs. 14.7% for cancer patients), but had a higher rate of RHC days with indirect/no contact (32.6% vs 29% for cancer patients).
Finally, patients living at home experienced more SIA-eligible RHC days (45.6%) than those residing in nursing homes (42.1%) or assisted living facilities (43.7%) and a slightly higher rate of days with phone contact (7% vs 6.4% nursing home and 4.3% assisted living). Patients living at home also had a lower rate of RHC days with indirect/no contact (27.9% for home residents vs. 32.6% for nursing home residents and 29.7% for assisted living).
Rates for SIA-eligible RHC days varied substantially across hospice programs (from a minimum of 31% to an almost double maximum rate of 60.9%). Rates also varied by LOS (60.5% for LOS of 1–7 days, 43.2% for LOS 8–14 days, and 39.5% for LOS greater than 14 days) and year (41.9% in 2005 vs. 44.9% in 2010), while indirect/no-contact days decreased considerably in 2010 (34.9% in 2005 to 26.9% in 2010).
RHC visit characteristics and duration
During the 1,352,638 RHC days, patients had a total of 2,818,695 visits or care activities. Table 3 reports the staff discipline for each type of visit, with the number of visits and the proportion delivered by each staff discipline (column percentages) within type of visit. Most of the SIA-eligible visits (80.5%) are delivered by RNs and the remainder by SWs. The non-SIA-eligible in-person direct care visits by staff other than an RN or SW were primarily delivered by home health aides (60.1%), followed by LPNs (15.4%) and by chaplains (13.8%).
The in-person direct patient care visits by RNs or SWs (inside the box) represent the SIA visits that qualify for additional reimbursement. Bereav, bereavement; HHA, home health aide; LPN, licensed practical nurse; MD, medical doctor; N/A, not applicable; NP, nurse practitioner; Other Th, other therapist (Aroma, Music, Pet, other); RN, register nurse; Skilled Th, skilled therapist; SW, social worker.
SIA-eligible visits had an average duration of approximately one and a half hours (93 minutes) and in-person non-SIA-eligible visits had a slightly shorter average duration at 85 minutes. In-person visits with no direct patient care were the longest at 107 minutes on average, most of which occurred on the day of death. Examination of visit duration over each of the last 7 days of life for those with LOS >7 days (to eliminate confounding by admission visits, which are inherently long) showed that the duration of direct care visits (both SIA-eligible and non-SIA-eligible) remained relatively steady at 6 to 2 days from the day of death at around 82 minutes, increased slightly the day before death to 86 minutes, but had a large increase on the day of death to 100 minutes for SIA-eligible visits, and 92 minutes for in-person direct care non-SIA-eligible visits.
Economic impact of the SIA reimbursement
A total of 251, 407 hospice decedents had 591,293 RHC days with 786,954 SIA-eligible visits (58.7% of the 1,340,532 in-person direct patient care visits). After combining all SIA-eligible minutes for each RHC day, 4,002 RHC days (0.7% of the 591,293 SIA days) had an aggregated SIA minutes below the 15-minute minimum requirement to qualify for SIA payment, so their SIA payment was set to $0.00. An additional 51,093 SIA days (8.6%) exceeded the maximum allowed 240 minutes that qualify for the SIA payment and were set to the maximum $157.5.
The average add-on payment per SIA-eligible day (including the 0.7% with $0) was $74.3 (SD = $41.9, Median = $62.3, IQR = $39.4-$98.4). Adding up all the SIA payments for each patient over their RHC days in their last week of life, there were 217,012 decedents for whom there was a potential SIA payment. The average payment for these SIA decedents was $202.5 (SD = $128, Median = $177, IQR = $108-$276); $201 (SD = $127) for nonprofit programs versus $234 (SD = $146) for for-profit programs. The hospice program with the smallest average potential SIA reimbursement per SIA person would have received $145.8 per SIA reimbursed patient, while the program with the most would have received $343.7 per SIA patient. Using the total number of patients with RHC days as the denominator, the programs with the smallest and largest SIA payments would have received $100 and $337.6, respectively, per patient with any RHC days in their last week of life.
Conclusions
Our results show that the majority (86.3%) of hospice decedents who had RHC days in their last week of life received one or more visits that would qualify for SIA reimbursements, with an average total add-on payment of $202.50 per decedent. To put this add-on payment in perspective, the average decedent with RHC days would have received $939 in regular RHC reimbursements during their last week of life (using CY2016 RHC rates of $186.83 for days 1–60 of the hospice stay and $146.83 for days 61+, and the LOS patterns in our sample). Therefore, the $202.5 average SIA add-on represents a considerable 21.6% increase over the usual RHC payments per patient with RHC days.
The size of the SIA payment incentive, together with the large disparity in SIA-eligible hours observed across hospice programs, has the important implication that while the SIA will incentivize all providers to increase the number of RN/SW visits during the last week of life, the incentive will be particularly strong for programs currently delivering at the low end of SIA-eligible minutes. These programs have more room to increase their SIA-eligible minutes, and the added SIA minutes will represent a larger marginal increase in payments than for programs already delivering at the high end. The expected result is a reduction in disparities in SIA-eligible hours across hospices and across decedents (as in the observed racial and ethnic disparities in SIA-eligible visits for African American and Hispanic decedents).
An important limitation of our study is that our sample of hospice programs is not fully representative of the current programs. Visit patterns and duration of visits that qualify for SIA payment could be very different for those not included in our study. The second largest limitation is that our study reflects usual care patterns in 2005–2010, and visit patterns will likely be different in 2016 after the payment rules changes introduced by CMS. However, the trends we observed in our study years toward more visits qualifying for SIA payments will likely continue.
Despite these limitations, this study is the first to examine the potential impact of SIA payments overall and to illustrate the large variability across hospice programs. It provides an important benchmark to put in perspective the importance of the SIA incentive. Our results point toward a potentially sizable increase in additional in-person direct patient care visits by RNs and SWs and a reduction in existing disparities of such visits that can significantly improve the quality of care received by hospice beneficiaries at their end of life.
Footnotes
Author Disclosure Statement
No competing financial interests exist.