
Abstract
Abstract
Background:
Dyspnea is one of the most frequent symptoms in children with complex chronic conditions (CCC) requiring palliative care. Although it is a subject of high importance, there has been little research on dyspnea in critically ill children.
Objective:
The purpose of this systematic review was to investigate the prevalence and causes of dyspnea in children with CCC and to identify the current state of research on the measurements, treatments, and the evaluation of therapeutic interventions.
Methods:
A systematic literature search for relevant literature from 1990 until the present was performed using the online database PubMed. Information about prevalence, pathophysiological mechanisms, measurement, and treatment of dyspnea was extracted from all 43 eligible publications.
Results:
The prevalence ranged widely from 17% to 80%. Breathlessness was primarily attributed to a disease-specific pathophysiology. A multidimensional approach has not been reported. Assessment of dyspnea included eight tools using either subjective self- or proxy-ratings or objective measures. Evidence for the effectiveness of various treatment approaches was low.
Discussion:
The prevalence rates for dyspnea could be generalized across all conditions and patient subgroups. The biopsychosocial–spiritual approach was not addressed by the studies. There is a lack of an adequate and validated measurement tool that can be applied to children of various ages and diagnoses, communication ability, and practicable across different settings. Most found treatment approaches lacked good evidence in children.
Conclusion:
Although the prevalence rate of dyspnea in pediatric palliative care is high, it has been poorly studied.
Introduction
D
In children with complex chronic conditions (CCC) that are often life threatening (LT) or life limiting (LL), dyspnea is also a frequently reported symptom.5–11 The experience of breathlessness is as frightening for a child as for the parents.3,12 Although the management of dyspnea in adults with LT and LL diseases has been investigated for many years,1,13,14 little research on this topic has been performed in children with CCC.
Recent publications suggest a multidimensional concept of dyspnea.1,15 Many different receptors (chemoreceptors and mechanoreceptors), mechanisms (biological, psychological, and social), and pathways1,16,17 are associated with the various sensations of breathing discomfort that include air hunger, a sense of work of breathing, effort, and tightness.13,15 The causes of dyspnea can be as diverse as the perception. The biological, psychological, social, and environmental factors interact. 1 In adults, the diseases that are frequently accompanied by dyspnea are chronic obstructive pulmonary disease, heart failure, and cancer (especially pulmonary, pleural, or mediastinal).2,18,19 In children and adolescents, breathlessness is commonly associated with severe asthma, compression of the respiratory system, impaired cardiac function, congenital anomalies of various organ systems, pulmonary infections, or breathing muscle weakness.3,4,12,20 In pediatric palliative care, the causes of dyspnea are often difficult to identify since the burden of extensive diagnostic procedures has to be weighed against the anticipated benefit. 21
The assessment of dyspnea in children with CCC is challenging because of the subjectivity and the complexity of this symptom. By definition, the subjective feeling of dyspnea can only be described by the patient. 1 However, self-report is often not possible in children as they lack the appropriate communication skills such as the very young and those with severe psychomotor impairment.3,10 However, proxy-ratings do not necessarily correspond to the child's perception of suffering 22 and signs of dyspnea such as heavy or labored breathing may not fully characterize the patient's experience. 13
Although evidence in adults is valuable to guide pediatric dyspnea management, treatment in adult medicine cannot be congruently transferred into pediatric practice, 3 especially because the underlying pathophysiology causing dyspnea in children may differ from those in adults.2–4,12,20 In addition, the caregiver has to consider that pharmacological treatment may cause age-specific side effects. Although rare, the possibility to cause respiratory depression exists when using fast-acting opioids. Treatment options for the management of breathlessness in children range from psychosocial to pharmacological to mechanical interventions. 20 Pharmacological and nonpharmacological treatment options are also important for children who are already on some kind of ventilation. In those patients sometimes secret management or technical adaptations such as changing ventilator settings are of utmost importance. However, there has been little research on the therapy of dyspnea in children with LT or LL CCC, due to this group of children being relatively small 23 and challenging to study in an experimental setting. 20
This review aimed to summarize the current state of research on dyspnea in children with LT and LL CCC with respect to the prevalence, pathophysiological mechanisms, measurements, and treatments of this symptom. The objective was to define if there was a need for further studies in these areas.
Methods
Literature search
A systematic literature search was performed with the online database PubMed on December 7, 2017. The two topics, children and dyspnea, were covered by using the keywords “Child” OR “Adolescent” OR “Infant” OR “Pediatrics” and the keyword “Dyspnea.” Articles published in 1990 or later were searched. The initial search resulted in 1564 articles.
The research group determined the following inclusion criteria:
Definition of LT and LL CCC
In this systematic review, solely studies dealing with children suffering from LT or LL CCC were included. CCC were defined according to Feudtner et al. as “Any medical condition that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or 1 organ system severely enough to require specialty pediatric care and probably some period of hospitalization in a tertiary care center.” 24
The CCC classification system categorizes various pediatric health states that may lead to palliative care at some point in their progression. The system was initially used to study the patterns of pediatric mortality and end-of-life care. 24 The actual version assigns the ICD-10 codes (International Classification of Disease, version 10) for a wide range of conditions to one of ten categories (cardiovascular, respiratory, neuromuscular, renal, gastrointestinal, hematologic or immunologic, metabolic, other congenital or genetic, and malignancy, premature and neonatal). The CCC categories and related codes are accessible in the reference list of Feudtner et al. 25
To extract studies that focused on CCC, we compared the underlying diseases of the children in every study to this reference list of all CCC in the ICD-10. 25 When the criterion of CCC was not met by the majority of patients in a study or when the diagnosis was not certain, the publication was excluded. This also applied for CCC-compatible diagnoses that were not considered to be potentially LT or LL. An LT illness was defined according to Craig et al. as one “where there is a high probability of premature death due to severe illness, but there is also a chance of long-term survival to adulthood.” An LL illness was “defined as a condition where premature death is usual.” 26
Study allocation
The titles and abstracts of all identified publications were screened for the inclusion criteria. Based on the information provided, the articles were classified as eligible for the review or not. If the information in the title and abstract did not suffice for classification, the full text was scanned. Any classification uncertainties were discussed by two authors (L.P. and M.P.) to reach a consensus. In addition, the reference list of the included publications was browsed to identify additional relevant studies, and the previously known literature was screened for suitable references. All hand-searched publications had to comply with the inclusion criteria.
Results
Overview of included studies
A total of 45 publications were included in this review (Fig. 1). Of these, 23 studies had a retrospective character, and 14 were prospective. Two studies were randomized controlled trials. Seven case-series studies (n ≥ 3) were included.

Flow diagram: articles screened.
Prevalence of dyspnea
Data concerning the prevalence of dyspnea in children with LT or LL CCC were found in 15 studies (Table 1). Six studies collected data from medical charts,5,7,9,10,27,28 seven via parental interviews,6,8,11,22,29–31 one during clinical presentation, 32 and one by self-report. 33
na, not available; oap. overall prevalence; AHD, advanced heart disease; CVA, congenital vascular anomalies; L, leukemia; ST, solid tumor; LY, lymphoma; CNST, central nervous system tumor.
The most commonly used sources for the assessment of the child's dyspnea were reports by the medical staff5,7,9,10,27,28 or by the parents via questionnaires.6,8,11,22,29–31 Four studies used a comparable comprehensive semistructured questionnaire for the assessment of symptoms as perceived by the patient's parents.6,29–31 In two, an instrument constructed for patient rating of various symptoms was used to evaluate dyspnea9,33 and in one the parents had to list up four main symptoms in their child's last month of life. 11
The prevalence of dyspnea in children with CCC ranged from 17% to 80% and varied with the diagnosis (Table 1). Importantly, these data were based on different assessment methods and refer to various time periods and were therefore not directly comparable. The highest dyspnea prevalence at the end of life was reported to be 80%, which was observed in children with cancer, 6 and the lowest prevalence was 21% in a mixed sample. 9
Seven publications investigated symptoms exclusively in children with cancer. In summary, the prevalence of dyspnea in children with cancer ranged from 41% to 80% at the end of life. According to the judgment of the authors, 29–58% of the children with dyspnea suffered severely from this symptom.5,6,22,29–31 The only study of children with cancer who were not receiving end-of-life care reported an overall prevalence of 17% and noted that different kinds of cancer lead to varying dyspnea prevalence (leukemia: 22%; solid tumor: 19%; lymphoma: 12%; central nervous system tumor: 6%). 33
Five studies investigated dyspnea in pediatric palliative care patients with different CCC. The prevalence of dyspnea in these mixed samples ranged from 21% 9 to 61% 11 during various time periods of palliative care. Specially, the prevalence was 61% in the last month of life, 11 ranged from 32% to 47% in the last week9,10 and was reported to be 21% in one study during the last day of life (Fig. 2). 9 According to the investigators, 100% of the children felt distress when dyspnea occurred at the time of admission to the pediatric palliative ward 7 and 17% felt distress from dyspnea when the symptom occurred on the last day of life. 9 In one publication, the relationship between dyspnea prevalence in the last week of life and the location of death was investigated. 9 The data from the medical records suggested that dyspnea occurred less frequently in the pediatric intensive care unit (35%) than in the ward (70%). 9
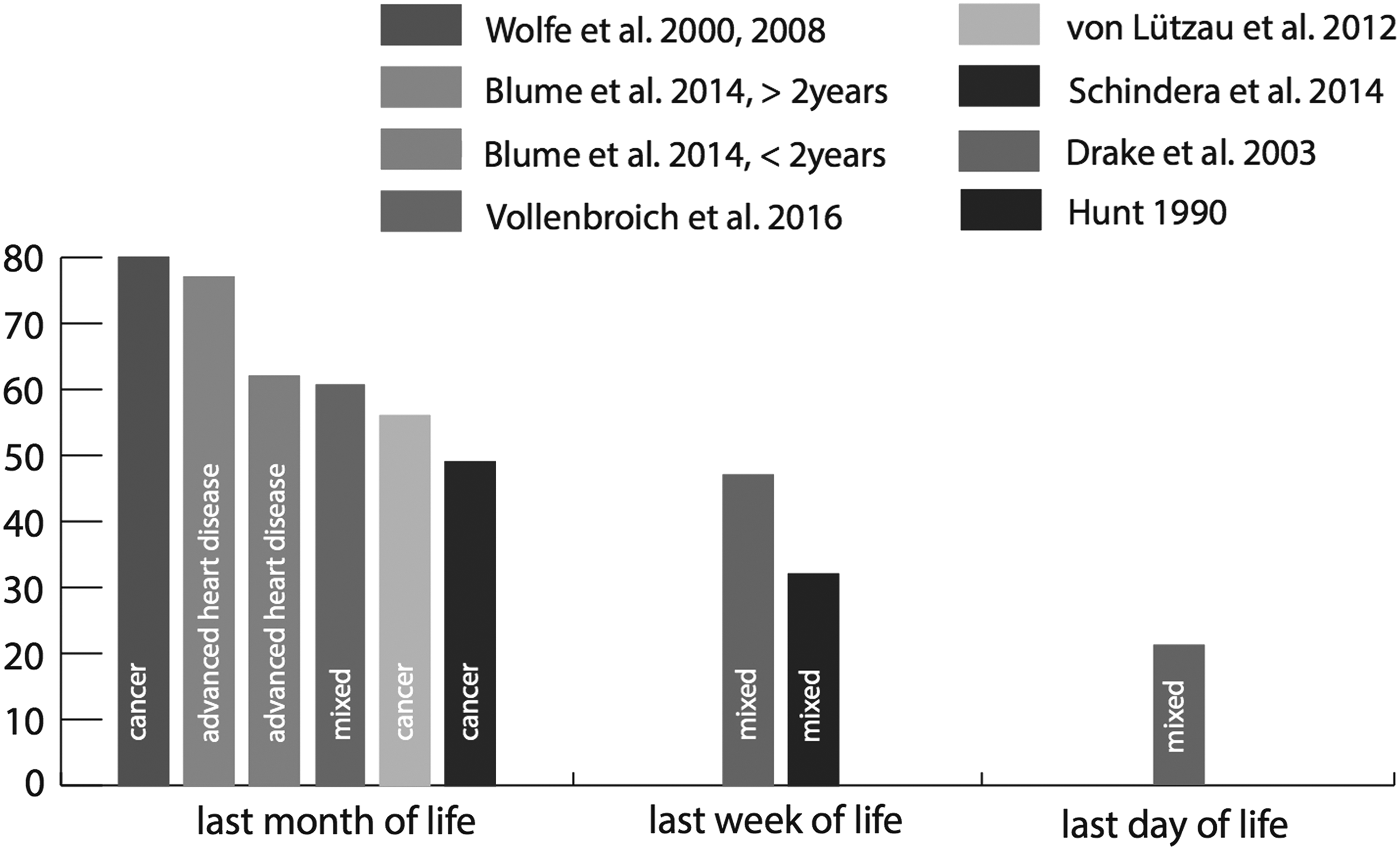
Prevalence of dyspnea toward the end of life in children with CCC. CCC, complex chronic conditions.
Pathophysiological mechanisms of dyspnea
Conditions that had the potential to influence the experience of dyspnea were reported in 33 studies. Dyspnea was described in pulmonary as well as in extrapulmonary diseases, but none of the studies exclusively reported the pathophysiological mechanisms or the variety of causes that might contribute to dyspnea in children with LT or LL CCC.
The “Oxford Textbook of Palliative Medicine,” 17 as an external source, provides five categories of mechanisms that have the potential to cause dyspnea. Conditions may lead to breathlessness via an “increased respiratory drive,” “mechanical impedance,” “respiratory muscle failure,” “wasted ventilation,” and “psychological” mechanisms or a combination of these given causes. Most dyspnea-related conditions and diseases found in the studies reviewed here could be assigned to one or more of these categories of pathophysiological mechanisms.
1. An increased respiratory drive can be triggered by various pathophysiological features such as hypoxemia, metabolic disorders, or intrapulmonary receptor stimulation. 17 Reported conditions that may result in hypoxemia include cystic fibrosis (CF)34–41 or other respiratory diseases,42–46 cardiac pathologies8–10,27,28,42,47–50 or lung infections.21,27,51,52 CNS pathologies such as severe motor and cognitive disabilities due to various conditions or brain tumors10,27,30,42,53 can also change the respiratory drive. Renal pathologies 42 can be accompanied by metabolic disorders, and intrapulmonary receptor stimulation may be caused by pulmonary edema. 54
2. Mechanical impedance can accompany airflow obstruction, mechanical chest wall restriction, or reduced compliance. 17 Reported pathologies consistent with this mechanism include malignancies or metastases,27,52,54–56 which may cause impairment of pulmonary ventilation or compression of the airways. In addition, various chest wall diseases have the potential to contribute to dyspnea. 55 Subglottic stenosis32,57 was another reported diagnosis with the potential to cause dyspnea due to airflow obstruction.
3. Respiratory muscle failure may contribute to dyspnea in affected children. 17 Muscle diseases41,42,52 or mechanical disadvantages such as pleural effusion21,54,55 have the potential to cause respiratory muscle weakness or failure and dyspnea.
4. Wasted ventilation can occur in conjunction with large vessel obstruction or capillary damage. 17 Studies conducted with children suffering from these conditions were rare. Reported causes with the potential to lead to this condition were congenital vascular anomalies 28 or advanced heart disease. 8
5. Psychological mechanisms may lead to dyspnea or increase the sense of dyspnea that has another primary cause. Anxiety and depression are two examples of psychological conditions that possibly induce or enhance dyspnea. 17 No study reported psychological reasons for the development of dyspnea.
Besides disease-related causes, the side effects of different treatments were temporally associated with the development of dyspnea.5,58–60 Children with cancer who received chemotherapy during the last four weeks before death were reported to experience dyspnea more often than those who did not receive chemotherapy at this stage of disease. 5 Another study reported that dyspnea occasionally occurred after lung irradiation for cancer in children. 59 In some cases, pediatric patients who were treated with stem cell transplantation for malignant infantile osteopetrosis developed severe pulmonary hypertension with dyspnea during the first three months after the transplant process. 60
Measurement and assessment of dyspnea
Tools for the measurement or assessment of dyspnea used either self-assessment (subjective self-rating), observations of the patient's behavior and condition (subjective proxy-rating), or physiological parameters to rate the experience of breathlessness (objective measures). Fourteen studies reported on the measurement of dyspnea; a total of eight different tools were applied.9,33–40,42,47,50,61,62 Four studies focused on the evaluation or development of tools for the measurement of dyspnea in children with LT or LL CCC37–40 (Table 2).
ic, internal consistency; na, not available; CF, cystic fibrosis; rt-t, retest reliability; ri-i intraindividual reliability; α, Cronbach's alpha. 59
Subjective self-rating tools
The “Dalhousie dyspnea scales” were developed for self-rating by visualization of the severity of the three dyspnea sensations, “effort,” “chest tightness,” and “throat closing,” using pictorial scales. For each sensation, a set of seven cards with increasing severity was created for the rating of dyspnea. The scales were validated for mentally healthy children (≥8 years) with CF or asthma. 38 Four studies mentioned the “modified Borg Scale” (BS), a tool to measure the effort to breathe and the discomfort evoked by breathing during exercise using a 0–10 rating.35–37,39 The BS was validated for mentally healthy children (≥9 years) with CF. 37 Another tool, the “Visual Analog Scale” (VAS) was used to measure dyspnea in three publications.39,47,61 The VAS measures the severity of breathlessness using a 0–10 rating. No study had the sole objective to validate the VAS.
The “Medical Research Council dyspnea scale” (MRC), which measures the impairment due to dyspnea, 36 and a “numeric rating scale” 34 were each used in one study. The psychometric quality of these two scales was not tested. Two studies used the items regarding dyspnea from the “Memorial Symptom Assessment Scale” (MSAS) to rate shortness of breath.9,33 A version adapted for children aged 10–18 years was used. This scale is a patient-centered rating instrument for the evaluation of a wide range of symptoms in children with cancer. To measure frequency, severity, and distress for each symptom, 4- or 5-point Likert scales were used. In one study, the tool was completed by proxy from a nurse, 9 in the second by self-rating. 33 The validity of the tool has been confirmed for communication-competent children, aged from 10 to 18 years. The rating of dyspnea was not validated separately. 33
Subjective proxy-rating tools
One cross-sectional study used and validated the “Liverpool Respiratory Symptom Questionnaire” (LRSQ) for cognitively normal and neurologically healthy children. The tool measures chronic respiratory symptoms across different domains, including the shortness of breath. Over a period of three months, the parents documented their observations of the child. The LRSQ was validated for pediatric patients with CF, aged from 6 to 12 years. 40
Objective parameters
The “Fifteen-Count Breathless Score” (15-count score) incorporates objective measures. It distinguished between different degrees of breathlessness by measuring the number of breaths taken to count up to 15. It was applied and validated in children with CF aged from 6 to 18 years in one study. 39
One study dealt with children unable to communicate their symptoms. In the absence of a tool to measure dyspnea in newborns, the researchers evaluated the child's general condition and focused on the observation of the behavior. Indicators for the sensation of breathlessness or respiratory distress were increased work of breathing and evidence of distress. Labored breathing was considered if tachypnea, nasal flaring, grunting, use of accessory muscles, or chest wall retractions occurred. Distress was interpreted if restlessness, irritability, or crying was observed. 42 In a case series (n = 4) of severely neurologically impaired children, observations such as “struggling to breathe” and “very agitated” described respiratory distress. 62 Cyanosis and changes in depth of breathing, chest expansion, or breathing sounds, as well as anxiety, were used to assess the respiratory status in other studies.37,50
Measured physiological parameters were oxygen saturation and heart beat, as well as spirometry results, in children with CF.37,39,50
Treatment and evaluation of dyspnea therapy
A total of 16 studies reported on dyspnea treatment in children with LT or LL CCC. The approaches to therapy ranged from preventive methods to the symptomatic use of medicinal and nonmedicinal interventions.
Disease-modifying therapies: secondary/tertiary prevention in dyspnea
The preventive effects of a six-week inspiratory muscle training with an inspiratory-threshold loading device were investigated in children with CF. A controlled trial compared the effect on the strength and endurance of inspiratory muscles between eight trained children (trained at up to 40% of maximal static inspiratory pressure [PImax]) and eight patients who performed only a low-intensity training (trained at a load of 10% of PImax). The effect on dyspnea was measured. Neither a statistically significant change in the dyspnea scores from baseline in any group nor a statistically significant difference in the dyspnea scores between the groups was observed after six weeks of training. No adverse effects were reported. 36
The preventive use of noninvasive ventilation (NIV) was tested in a randomized controlled trial in 13 clinically stable children with CF. All participants performed a six-minute treadmill walking test with and without NIV. Compared to the nonuse during the test, NIV significantly improved the walking distance, forced expiratory volume in one second (FEV1), and rib cage volume. However, no significant difference in the BS scores between the tests was found. 35
Pharmacological treatment
1. One retrospective chart review with a small sample size (n = 11) reported on the use of opioids for dyspnea in palliatively attended newborns and infants with different CCC. In more than 81% (n = 9), labored breathing and restlessness were ameliorated after the intranasal application of fentanyl. In two cases, only one dose was needed, whereas in others, the children were treated with 2–15 doses within minutes or hours. The initial dose ranged from 0.2 to 3.8 mcg/KG BW, depending on the patients' conditions. No adverse effects occurred. 42 One case series (n = 4) described the use of buccal morphine sulfate in nonverbal children with severe neurological impairment. Morphine was used when respiratory distress was persistent and recurrent despite the use of disease-modifying interventions. The initial dose ranged from 0.025 to 0.1 mg/KG BW with later dose increases in three children (maximal dose: 0.09–0.25 mg/KG BW). The opioid was administered every four hours when needed. Clinical significant benefits from morphine application such as relaxation, a decrease of distress, or a comfortable look were reported in all patients. Respiratory depression, significant sedation, or other adverse effects were not identified. 62
2. The use of methotrimeprazine as an antipsychotic drug for the management of end-of-life symptoms was described in another retrospective chart review. Dyspnea (n = 8) or respiratory distress (n = 2) was treated in children with various CCC. No isolated effect of methotrimeprazine could be measured because it was used in combination with morphine (n = 8) or fentanyl (n = 1) in 9 of 10 cases. In six patients, the symptoms clinically “improved,” “settled,” or “decreased” after application. In two patients, sedation was observed. None of the children presented with abnormal neuromuscular or other adverse effects. 41
3. Benzodiazepines, mostly midazolam (65%), were reported to be used for sedation and to address dyspnea and anxiety in 30 terminally ill children with CCC in one study. The effect of benzodiazepines on dyspnea or possible adverse reactions of this therapy were not presented. 9
4. The application of oxygen in cases of dyspnea or hypoxemia was documented in several studies,9,27,34,51,53,54,59,60 but none investigated the effects systematically.
5. The daily use of inhaled treatments (steroids, albuterol, and ipratropium) was used additionally to other medications to treat recurrent respiratory distress. 62
Mechanical treatment
The symptomatic use of NIV was investigated in a sample of 44 children with CNS disorders and acute respiratory distress due to severe pneumonia. Twenty-two children were treated with additional NIV when the conventional therapy was not effective. In this group, the arterial carbon dioxide tension (PaCO2), arterial oxygen partial pressure (PaO2), the ratio of partial PaO2 and fraction of inspired oxygen (PaO2/FiO2 ratio), heart rate, and blood pressure (RR) significantly improved after one hour of treatment, and no child needed progressive treatment. In the control group, none of these parameters improved and three patients went into progressive desaturation that required invasive ventilation. It was not the objective of the study to investigate changes in the dyspnea intensity or the clinically observed respiratory distress. In two cases, the therapy had to be discontinued due to poor compliance of the patient. In addition, two children developed facial erythema and one a nasal ecchymosis. 51
Four studies mentioned the use of mechanical ventilation.6,9,53,62 In one study, which investigated symptoms in 103 children dying from cancer, 45% of the patients were dependent on a ventilator in the last 24 hours of life. Ventilatory support was withdrawn in 80% after onset. 6 The second study described a mixed sample of dying children (n = 30) in whom artificial ventilation was used in 66.7%. The investigators did not specify the type of ventilation applied. 9 Statements concerning any effect of this approach were not presented in either study.6,9 In another publication, 13 severely disabled and dyspneic children who suffered from acute respiratory distress syndrome (ARDS) were treated with mechanical ventilation, oxygen, and antibiotics. In some of these patients, steroids, surfactant therapy, or methylprednisolone pulse therapy was also used. Nine patients recovered completely. It was not the focus of the study to report any effect of the treatment on dyspnea. Three of the children died despite therapy. 53 In one patient with severe neurological impairment, mechanical ventilation was used overnight. The treatment's efficacy was not outlined. 62
Independent of any therapeutic approach, there were three studies on the end-of-life symptom control in children with cancer. One publication (sample size n = 48) reported successful treatment of dyspnea using a retrospective parent proxy-report in 51.9% or 46.7% if children suffered severely from dyspnea. 30 In the second study (sample size n = 103), dyspnea was treated in 65% and the therapy was considered successful by the parents in 16%. 6 In the follow-up, national and local efforts for the improvement of palliative care systems led to significantly less suffering when dyspnea occurred (37% compared with 58%). Efforts consisted of the foundation of a multiprofessional “Pediatric Advanced Care Team” (PACT), which provided frequent teaching for pediatric oncology practitioners, clinical consultations to patients and families, as well as a close cooperation with the oncology ward. 29
The surgical treatment of the underlying diseases that caused dyspnea was reported in five additional publications,28,32,49,56,57 but it was beyond the scope of this review to describe all surgical details.
Discussion
It was the aim of this review to summarize the current state of research on dyspnea in children with LT and LL CCC with respect to prevalence, pathophysiological mechanisms, measurements, and treatments. The systematic summary of this information is essential for the initiation and implementation of further studies, the development of valid measurement tools, and the further investigation and evaluation of treatment methods.
Prevalence of dyspnea
The published studies showed a wide range in the prevalence of dyspnea in children with LT or LL CCC. Similar to findings in adult patients,2,63 different sample characteristics such as the underlying diseases and methodological differences in the assessment of dyspnea lead to varying prevalence rates.
The results discussed in this review showed that dyspnea prevalence was reported lower the nearer the children were to death, irrespective of the diagnosis (Fig. 2). However, this did not necessarily show the extent of changes in the occurrence of dyspnea toward end of life in children with CCC because this observation could be the product of various differences between the studies such as varying treatment approaches or different methods with respect to data sources and study design.
Only one study investigated dyspnea prevalence on the last day of life. 9 It may be that the high number of children with altered consciousness in this phase contributes to a lower prevalence of dyspnea. The study was conducted with the lowest number of participants (n = 30), and results may therefore not be reliable nor generalizable. Regarding prevalence estimates based on parental proxy reports, it is uncertain whether the parent's perception accurately corresponds with the experience of the child.6,22 Although a significant parent/child correlation concerning the child's quality-of-life rating was previously reported in communication-competent children with cancer, 64 the subjective experience of dyspnea can only be perceived and described by the patient. 1 Moreover, parental interviews were performed one to five years after the child's death. Most likely, the parent's perception of symptoms will change over time 6 and may have been influenced by other factors associated with the child's death. The retrospective chart reviews could have been influenced by incomplete documentation during the care, which could have resulted in an underestimation of symptom prevalence.
In summary, the generally high dyspnea prevalence of 49–80% in the last month of life5,6,8,11,29,31 indicates the importance for reliable measurement, detailed documentation, and good evidence for treatment approaches of dyspnea in children with CCC who are receiving palliative care. The differences observed in the occurrence of dyspnea led to the conclusion that special attention must be given to precise measurements of the symptom in future studies, although this might be challenging due to the complex character of this symptom. Nonetheless, the availability of validated measurement tools that are applicable across all settings of end-of-life care and for children with a wide range of underlying diseases is essential to collect precise and comparable data concerning dyspnea prevalence.
Pathophysiological mechanisms of dyspnea
The mechanisms leading to dyspnea in children with LT or LL CCC varied widely. None of the studies focused solely on the causes of breathing discomfort in these children. All information was extracted from case series or articles that had other main research topics. Overall, the reported causes were physiological in nature and can therefore be summarized in the previously mentioned categories of the pathophysiological mechanisms related to dyspnea. 17
Importantly, dyspnea is not always the consequence of a single biological pathology. In fact, dyspnea is a multifactorial symptom that is influenced by various conditions. Modifying factors can include those of physiological, psychological, and social nature. 17 Depending on the main cause, different sensations of dyspnea, including “air hunger,” “sense of excessive work of breathing,” and “tightness,” 15 can be generated by stimuli of various receptors and pathways. 16
It is surprising that no psychological or social causes were reported in the literature given the biopsychosocial model of care used in pediatric palliative care. This is remarkable as anxiety is closely connected to dyspnea,12,20,23,50,63,65 and these two conditions have the potential to exacerbate each other. 3 Moreover, feelings such as sadness, loneliness, and tension may aggravate the perception of dyspnea, 63 but no studies noted their influence. Pain also has the potential to cause dyspnea. 3 None of the extracted studies described this interrelationship.
In contrast to clinical experience, none of the studies reported on common musculoskeletal diseases such as muscular dystrophy and scoliosis related to degenerative and nondegenerative conditions or the frequently observed problem of hypersecretion. Clinical experience would suggest hypersecretion can be closely associated with the sensation of dyspnea, especially at the end of life in children with CCC.
It is apparent that the detection of the potential etiology for dyspnea in children with CCC is challenging due to the variety of pathologies and the appropriateness of pursuing the cause of dyspnea during the terminal phase.5,21 Nevertheless, it is important to identify as many of the potential causes as possible to better direct therapeutic interventions so as to improve treatment efficacy15,21 and minimize the child's suffering. These difficulties further illustrate the complexity of researching on dyspnea in children with CCC.
Measurement and assessment of dyspnea
The main problem concerning the measurement of dyspnea in children with LT and LL CCC is the lack of an adequate assessment tool. As many children in this cohort are unable to self-report, symptoms must frequently be interpreted by their caregiver.10,42,62 The subjective nature of such interpretations, for many reasons, runs the risk of the symptom's intensity and, as a direct result, the child's suffering, being underevaluated. This can be particularly challenging for parents and inexperienced medical and nursing staff.
In children with limited communication, due to young age or disease, no established dyspnea-assessment tools34–40,42,47,50,61 are able to assess acute-onset dyspnea or able to detect sudden changes in the symptom intensity. Six tools34,36–39,47 require a reasonable level of communication and cognitive capacity to understand the instructions and complete the assessment. The LRSQ may be the only instrument that could be appropriate for the use in children unable to provide self-assessment. However, the purpose of this score is to assess chronic respiratory symptoms over a period of three months and not to measure acute dyspnea. 40
Only four of the analyzed studies37–39,47 provide validation of self-assessment tools in children able to communicate with CCC. BS, VAS, and the 15-count score37,39 can be completed rapidly39,66; advantageous in the assessment of an acute dyspnea attack. A combination of the subjective BS or the VAS with an objective tool such as the 15-count score can improve the reliability and accuracy of the measurement. 4 The “Dalhousie dyspnea scales” provide an accurate means to assess the sensation of dyspnea. 4 However, it has not yet been determined how the scales can be used in a clinical setting and to assess a dyspnea attack. 38 It is noteworthy that the “effort” scale in this instrument does not have the robust validity of the other two scales,4,38 probably because this sensation is harder to understand. 38
None of the self-assessment tools has been validated for preschool children.37–39 All four studies with the objective of evaluating the dyspnea tools were conducted with CF patients.37–40 Therefore, the instruments may be not suitable for use in other underlying diseases. Concerning the physiological parameters, it is noteworthy that the measurements of respiratory rate, oxygen saturation, or blood gases have no correlation to the sensation of dyspnea. 67
As in adults, 66 there is no gold standard for the assessment of dyspnea in children with advanced disease. Therefore, the need to adapt and validate existing tools or to develop new instruments to improve the measurement of dyspnea is urgent, especially for pre-school children or those without sufficient communication skills. A detailed and comprehensive assessment tool needs to be applicable across all settings and in children with varying underlying diseases. This requires the consideration that dyspnea can be the result of a wide range of pathological mechanisms and can cause a variety of breathlessness sensations. At the same time, it must be mentioned that difficult quantifiable aspects such as experienced distress and suffering complicate the construction of an adequate assessment tool.
Therapy and evaluation of the treatment
Various approaches to the treatment of dyspnea in children with LT and LL CCC have been reported in the literature. Management strategies vary from psychosocial to pharmacological to mechanical interventions. 20 However, for most of these approaches, strong evidence is lacking. Importantly, a reduction of dyspnea can be supported by the understanding and treatment of the causes.21,67 Pain, anxiety, poor fluid balance, and underlying diseases need to be identified and approached with appropriate treatments.3,67 Nevertheless, professionals must frequently intervene without solid evidence and initiate the therapy without having clarification of the pathophysiologic process at play. 21
Disease-modifying therapies: secondary/tertiary prevention of dyspnea
To date, there is no proof for the effectiveness of preventive approaches for treating dyspnea in children with CCC. Two studies testing inspiratory muscle training and NIV failed to show statistically significant positive effect on dyspnea in the participants, suggesting these interventions may not be useful in the prevention of dyspnea in children with CF.35,36
Symptomatic treatment
Symptomatic management options such as self-hypnosis, relaxation techniques, airway-clearing techniques, or fans blowing directly on the face for the treatment of mild dyspnea in children with CCC have not been investigated although these methods may be appropriate in other children. 20 Apart from that, no research on further nonpharmacological strategies such as guided imagery, therapy with social workers or others was found.
All included studies reporting on the use of any pharmacological therapy were limited due to small sample sizes,9,41,42,62 the retrospective character,9,41,42 and the rudimentary outcome reports.9,41 This means that to date, there is no evidence for pharmacological dyspnea treatment in children with CCC.
In adults, however, the use of opioids in dyspnea treatment in advanced disease is well studied and there is a solid evidence base. 68 Recently, published reviews show that opioids are frequently used as a therapy for the relief of dyspnea in pediatrics as well.3,20 In opioid-naive children, a starting dose of 25% for pain therapy seems appropriate and can be increased as needed.3,12,20 We found two studies dealing with opioids. One retrospective chart review suggested that the use of an intranasal fentanyl for labored breathing in newborns was minimally invasive, safe, and effective. 42 A case series described the successful treatment of respiratory distress with buccal morphine. 62 However, small sample sizes and the retrospective nature of the studies limited determination of safety. No sufficient evidence from a randomized controlled trial regarding the efficacy of opioid therapy was available.
A single study tested an antipsychotic (methotrimeprazine) for the treatment of dyspnea. 41 The isolated effect of methotrimeprazine in dyspnea management could not be evaluated because it was administered with opioids in 90% of the subjects, rather it was suggested to be a potential adjuvant for palliating dyspnea in combination with opioids. 41 However, there have been conflicting reports regarding possible potentiation of the respiratory depressive effects of opioids,69–71 and no evidence for safe and effective use was provided. To our knowledge, also in adults, antipsychotics are not a considered treatment option against dyspnea.
Benzodiazepines can control anxiety, which often accompanies breathlessness, but they are not recommended as stand-alone agents in the absence of opioids.12,20 They appear to be used frequently in conjunction with opioids to resolve dyspnea 12 but their use in children with CCC was only reported in one study. 9 No outcome was reported by this study preventing further evaluation.
The use of oxygen in patients with obvious hypoxemia is recommended, 20 and the application seems to enhance the patient's and parental sense of control. 12 In children with chronic carbon dioxide retention, careful use is required to avoid suppression of the hypoxic drive. 3 However, evidence for the improvement of dyspnea by oxygen application is missing in children with CCC.
The initiation of NIV is one option to treat respiratory failure in children with CNS disorders. The use of this intervention leads to significant improvements in blood gas parameters, and there is a trend to prevention of endotracheal mechanical ventilation in some cases. 51 Lessening of dyspnea can be a secondary benefit of this approach. Although NIV is considered to be minimally invasive, mild side effects and the need to discontinue in two cases imply the experience can be distressing. 51 Positive treatment effects should be considered carefully against the risk of additional suffering caused by the NIV in every individual child. No study has investigated the effect on the subjective experience of dyspnea.
Mechanical ventilation has been reported to be used at the end of life in children with cancer or in disabled children suffering from ARDS,6,53 but no outcomes concerning the individual experience of dyspnea were presented. It is therefore not currently possible to provide any statement about the effect on dyspnea.
Finally, the use of NIV and invasive ventilation with the intent to treat dyspnea is challenging. A distinction must be made between children with diverse CCC. For example, in children with CNS disorders, ventilation is mainly used to support the secondary effect of reducing dyspnea. In a child with cancer at the end of life, the primary purpose of ventilation can be to lessen suffering from respiratory distress. In any case, it has to be considered individually, if ventilation is sufficient to achieve the goals of treatment and if local resources are in place. Other management options need to be reviewed, as well as the length of ventilation.
In summary, knowledge regarding the psychosocial and medical treatments of dyspnea in children with LT and LL CCC needs to be extended. Studies with representative sample numbers, patient characteristics, including a mix of diagnoses, and various levels of communication and detailed outcome reports are required to determine the most appropriate management approach for this symptom. The aim of future research should work toward a stratified and stepwise strategy for management of dyspnea in children with LT and LL CCC.
Limitations
As the literature search concentrated on the PubMed database, the review's focus is primarily medical. This search may not capture all nonmedical interventions, studies of nursing science, and psychological research available.
Conclusions
The result of this systemic review demonstrates that little research has been conducted on the prevalent and distressing symptom of dyspnea in children with LT and LL CCC. It frequently causes suffering to the child and affects the parents requiring future research to focus on the social, psychological, as well as the physiological aspects.
A reliable measure of dyspnea is necessary for future research on the prevalence, pathophysiology, and treatment of this symptom in children with CCC and has the potential to help the caregiver manage the sensation of breathlessness more efficiently. There are few tools for the assessment of dyspnea in children with CCC, which have only been validated in a limited number of diagnoses. The lack of a widely applicable and standardized tool leads to diverse findings regarding dyspnea prevalence and complicates the determination of the possible causes that contribute to dyspnea. None of the available instruments can be applied in an acute episode of dyspnea or is able to detect sudden respiratory changes in nonverbal children. There is an urgent need to adapt and validate existing tools or to develop new instruments for the appropriate assessment of dyspnea in children with CCC. A suitable tool should be applicable in a wide range of settings, across various underlying diseases, and independent of the child's age and communication skills.
Research on dyspnea treatment in children with LT and LL CCC must be continued. Studies dealing with various therapeutic approaches are needed, from preventative measures to psychological and pharmacological treatments as well as finding the place of artificial ventilation techniques. Evidence for the appropriate intensity of treatment with detailed outcomes and safety for each approach must be increased. There is a high need for studies with a prospective design and representative study populations. Randomized controlled designs would be preferable, if possible. In addition, qualitative or mixed methods approaches may help to learn more about the complexity of dyspnea and associated suffering. Such research has the potential to allow development of a standardized and focused approach, which has the potential to enable caregivers to apply a stratified and stepwise treatment to affected children.
Footnotes
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.