
Abstract
Abstract
Background:
While early involvement and integration of palliative care with oncology can positively impact quality of life and survival of patients with advanced cancer, there is a dearth of information regarding this integration in sub-Saharan Africa.
Objective:
We sought to describe the rate and factors predicting specialist palliative referrals among cancer patients in Uganda.
Design:
We examined the rate of referrals of cancer patients to palliative specialists via a chart review, while also surveying and interviewing doctors at the Uganda Cancer Institute (UCI) about their approaches to palliative care.
Setting:
All adult patients at the UCI who died in a 20-month interval from 2014 to 2015. All UCI doctors were approached for the survey and 25 (96%) participated. Seven of these doctors were also individually interviewed.
Measurements:
Number of referrals to palliative specialists and qualitative responses to questions about end-of-life care management.
Results:
Sixty-six (11.1%) of 595 patients were referred to palliative care specialists. Patients with worse ECOG performance statuses were more likely to be referred to palliative specialists (odds ratio 2.23, p = 0.03); no other factors were predictive of a referral. Median number of days lived after referral was 5 days (interquartile range 2–13). Doctors explained the low referral rate and short life expectancy after referral by limited palliative resources and a reticence to have end-of-life management conversations with patients due to cultural taboos.
Conclusion:
Despite recognized benefits of palliative collaboration, doctors at the UCI seldom refer patients to palliative care specialists due to limited staffing, cultural barriers, and difficult interservice communication.
Background
E
Yet, palliative integration remains challenging. 7 Limited palliative care education,8–10 inadequate palliative staffing and resources,11,12 policy shortcomings,13–15 and insufficient outcomes data hinder effective integration. 16 This is most evident in resource-limited settings; palliative services are absent in 28 African countries. 6 Although several palliative care models have been built across sub-Saharan Africa (SSA), 17 Uganda is the only SSA country with an advanced integration of palliative care services. 6 Even in Uganda, however, only <10% of palliative care needs are met. 18
Most cancer care in Uganda is provided at the Uganda Cancer Institute (UCI), the sole comprehensive cancer center for a catchment area of >100 million people (Academic/Administrative Environment and Resources, unpublished reference manual. Uganda Cancer Institute/Hutchinson Cancer Care Alliance.). With roughly 4000 new cancer patients a year, over 75% with stage 3 or 4 disease (HIV prevalence at the Uganda Cancer Institute, unpublished data.), the UCI has great need for effective and integrated palliative services.19,20 When able, UCI physicians provide palliative care for cancer patients, but when palliative expertise is needed (no specific threshold exists, but is a reflection of the physician's professional comfort in providing the required palliative care), they refer patients to Hospice Africa Uganda (HAU) or the Makerere/Mulago Palliative Care Unit (MPCU), a palliative specialist team residing adjacent to the UCI at Mulago Hospital.20,21 These referrals are made in-house, with HAU and MPCU coming to the UCI.
To assess how UCI doctors manage palliative needs in advanced cancer patients, we conducted a mixed-methods study examining the frequency of referrals to palliative specialists, while also surveying and interviewing UCI doctors about their approaches to and attitudes toward palliative care for terminal cancer patients.
Methods
Patient cohort: Chart abstraction
All charts of UCI patients ≥18 years of age with a diagnosis of cancer who died between January 1, 2014 and August 31, 2015 were reviewed for demographic data, clinical diagnosis, date of clinical diagnosis, stage of disease, presenting Eastern Cognitive Oncology Group (ECOG) performance status, date of death, referral to palliative specialists, and date of referral. Vital status was determined by UCI medical records and confirmed on each patient file. Stages 3 and 4 cancers were considered late stage. Cancers with historic response rates of at least 50% to first-line chemotherapy were deemed chemosensitive; all other tumors were considered nonchemosensitive.22,23 “Newly-diagnosed” was defined as receiving a cancer diagnosis within 60 days of death. 24
Patients whose medical files did not contain clinical notes confirming cancer diagnosis or could not be found by the medical records office were excluded. District of residence was considered a binary, either living in Kampala or living outside of Kampala.
Physician cohort: Survey and interviews
After discussion with UCI and MPCU physicians and adaptations from a literature review,25–27 a survey was designed that assessed physician confidence and competence in administering palliative care and referral practices. This survey included Likert scales assessing physician confidence in palliative care and assessing physician attitudes toward palliative care. REDCap software captured survey data. The survey was offered to all UCI doctors who had provided clinical care at the UCI within six months of survey administration.
From April to May 2016, author D.L. conducted one-on-one, semistructured interviews with UCI doctors who were identified via purposive sampling to capture variability in gender, seniority, and experience in caring for different cancer types. Participant recruitment continued until thematic saturation was reached. An interview guide with open-ended questions explored physicians' understanding of palliative care, how decisions regarding palliative referrals are made, and how palliative care and oncology are integrated. Participants were also asked to assess and give care plans for two cases involving metastatic cancer. These interviews were conducted in English, audio-recorded and transcribed verbatim by D.L.
Data analysis
STATA v14.1 was used for statistical analysis of the chart review and physician survey. Postreferral survival was calculated as median number of days lived after referral. Factors associated with palliative specialist referrals were calculated with logistic regression. All variables with p < 0.20 from the bivariate analysis were used in the multivariate analysis. 28 Proportional statistics describe the frequency with which doctors felt confident in various areas of palliative care.
Authors D.L. and E.C.M. developed and iteratively modified a codebook from the transcribed interviews and conducted qualitative thematic content analysis. All codes were described with specific definitions and reviewed for internal consistency. Data analysis and data collection were done concurrently in an iterative manner to allow emerging themes to inform interviews and ensure saturation. Atlas.ti v1.0.46 was used for coding organization and analysis.
This study was approved by the Fred Hutchinson Cancer Research Center Institutional Review Board, the Uganda Cancer Institute Research Ethics Committee, and the Uganda National Council on Science and Technology.
Results
Chart review
Seven hundred thirty-eight adult cancer patients had a death recorded between January 1, 2014 and August 31, 2015. Of these, 138 medical charts (18.7%) were not found and 5 charts (0.7%) had no confirmed cancer diagnosis, leaving 595 (80.6%) medical charts for analysis. Of these 595 patients, 66 (11.1%) were referred to palliative specialists. The age of those referred was not significantly different to those not referred, and a comparable number of patients in the referred and not-referred groups lived outside of Kampala, were diagnosed with cancer less than 60 days before death, and had chemosensitive tumors (Table 1).
Percentage based on N = 58 and N = 406, as some charts were missing staging information.
Percentage based on N = 60 and N = 403, as some charts were missing performance status.
Bold indicates p value < 0.05.
CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; OR, odds ratio.
Sex (female), late-stage cancer, type of cancer, and comorbidity were significant bivariate predictors for referral to palliative specialists, but proved insignificant after multivariate logistic regression. Presenting ECOG performance status was the only significant predictor of referral, with patients presenting with an ECOG of 3 or 4* more likely to be referred to a palliative care specialist (odds ratio 2.23, p = 0.03) (Table 1).
Of those referred, none was referred at time of cancer diagnosis (Table 2). Nine percent were referred during chemotherapy treatment, 9% were referred at diagnosis of metastatic disease, and 72% were referred after recognition of metastatic disease and/or after having stopped chemotherapy. Once a patient was referred to a palliative care specialist, the median survival was 5 days (interquartile range 2–13) (Table 2).
Survey and interviews
Twenty-five doctors (96%) partook in the physician survey. Of these, 21 (88%) reported previous training in palliative care. Seven of the 25 surveyed doctors were purposively selected for interview; due to a limited number of variables reported as influencing referral patterns, saturation was achieved after seven interviews (Table 3).
When physicians were interviewed about the timing of and life expectancy after specialist palliative referrals, their perception differed substantially from what was documented in the medical records. Nearly half of doctors (48%) reported that specialist palliative referrals generally occurred at time of cancer diagnosis. Ninety-six percent felt that those whom they personally referred had life expectancies exceeding one month, with 36% believing their patients lived at least six months after referral.
The reason for and timing of referrals were varied and complex. Key themes as integrated from the physician surveys and individual interviews are highlighted below.
Confidence in palliative skillset
UCI doctors felt confident in their ability to manage many aspects of palliative care, especially pain control.
“We try to offer care on our own … pain is very easy to manage in all of its aspects. It's easy to evaluate a patient and determine if this is somatic pain or neuropathic pain and be able to assess the level of pain, grade it, and prescribe and monitor the available pain medicines” (Male Medical Officer 7).
This confidence was reflected in the survey, where 100% of doctors reported feeling confident in their prescription of morphine, 84% in their basic communication skills surrounding palliative care, and 80% in symptom assessment and management (Fig. 1).
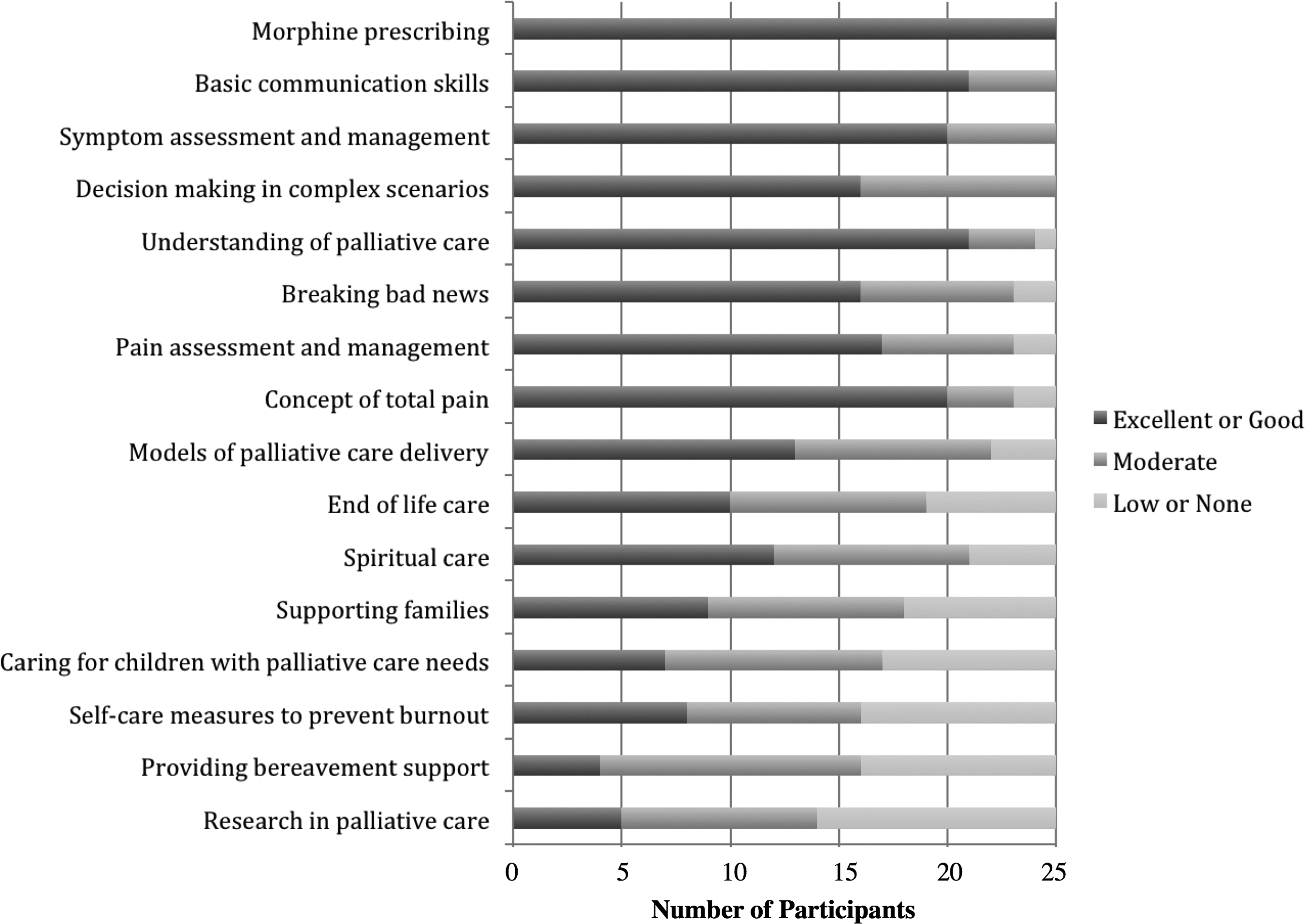
Physician confidence in palliative services.
There were areas within palliative care where doctors reported less confidence. Less than half of doctors were confident in spiritual care (46%), end-of-life care (40%), and supporting families (36%) (Fig. 1).
Who and when to refer
Eighty-four percent of surveyed doctors believed that not enough patients were referred to palliative specialists (Fig. 2). Despite the importance of performance status in the chart abstraction, interviewed doctors did not report using any specific protocol to determine whom to refer to palliative specialists. Nonetheless, doctors referenced four common reasons for referring patients to palliative specialists: (1) patients not responding to chemotherapy; (2) patients at the end of life; (3) not enough time to address end-of-life issues; and (4) patients needing more holistic care.
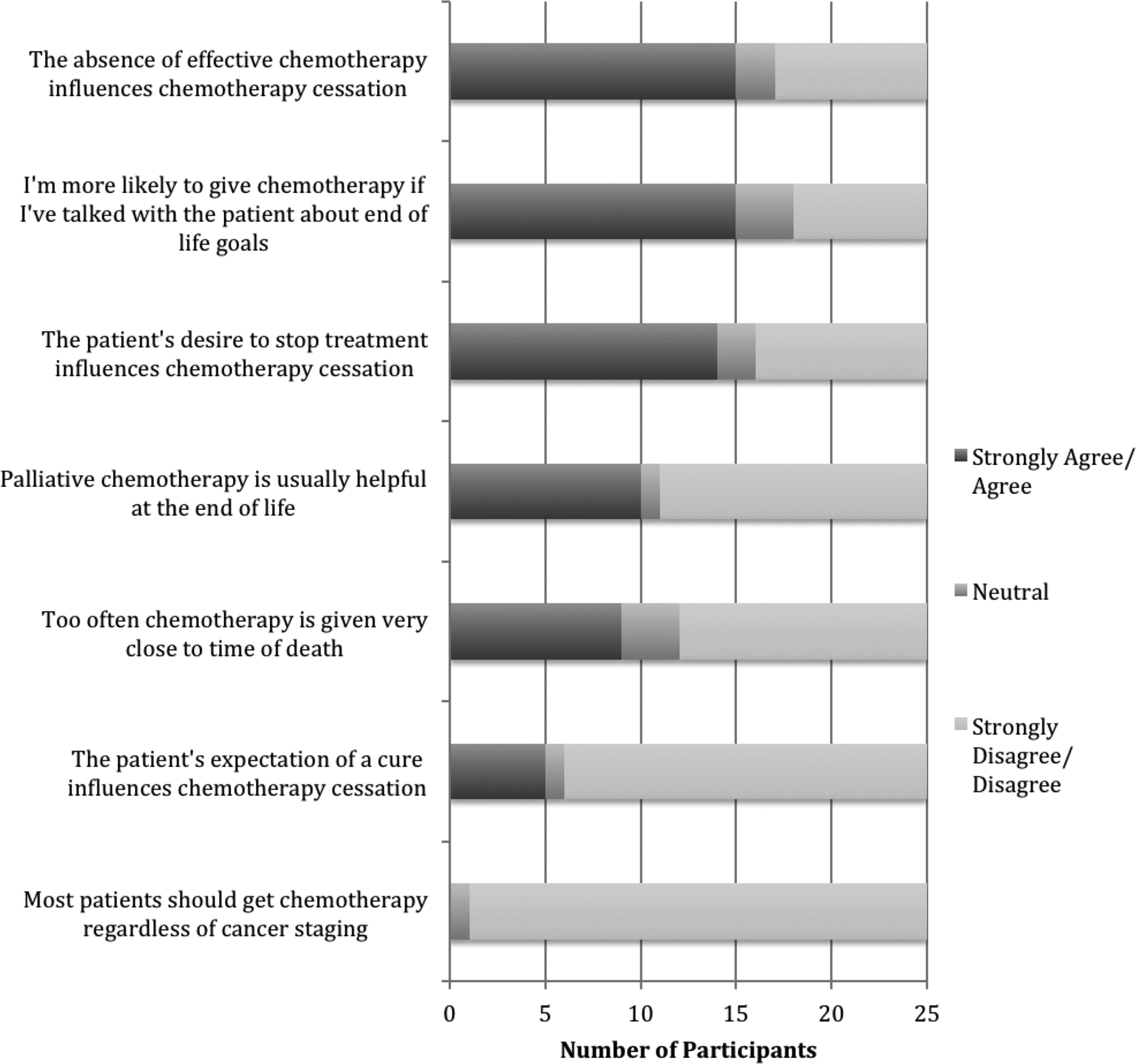
Physician attitudes toward palliative care.
End-of-life conversations
Several interviewed doctors explained the delay and lack of specialist palliative referrals by a reticence to discuss end-of-life care with patients.
“I don't know what percentage of doctors actually have that kind of conversation, but I would say it's very small, maybe less than 1% … It's a difficult conversation to have. People break down and cry. Some people go into denial or depression. You do not want to be the bearer of such news. So sometimes we just steer clear” (Female Medical Officer 1).
Of the physicians surveyed, 80% felt that end-of-life conversations did not happen frequently enough and only 40% were confident in end-of-life care (Fig. 2). Concerns about end-of-life conversations relinquishing hope and causing depression were reported by nearly 2/3rds of surveyed doctors (Fig. 2).
Cultural norms
Interviewed doctors also emphasized that discretion surrounding end-of-life conversations was linked to cultural constraints.
“In Uganda it's kind of taboo to talk about death. You find that many patients are scared about death. So most clinicians will avoid talking about death even when they know the patient is going in the next few days” (Male Medical Officer Special Grade 6).
Several stories were recounted about the cultural insensitivity of discussing death in Uganda. When asked to imagine themselves as patients with terminal cancer however, all interviewed doctors claimed they would want to know their prognosis and have an end-of-life conversation with their doctor.
When doctors cited instances of disclosing prognoses to patients and having end-of-life conversations, the overwhelming majority of disclosures were well received.
“At the end of it all, the family was actually very grateful. The mom came back and told us, ‘I am very relieved you told me this.’” (Female Medical Officer 1)
“This man gave me a cow just because I told him” (Male Medical Officer Special Grade 2)
Coordinating palliative care
All interviewed doctors felt that most of their patients would benefit from involvement of palliative specialists and better integration with the palliative specialist team, but recognized that most patients were not being seen by palliative specialists.
Access to specialists
While 96% of surveyed doctors believed palliative specialists helped their patients (Fig. 2), most also had concerns regarding the lack of staffing.
“Many times, whereas generally we would like to refer a patient at cancer diagnosis, we understand the weight we would be exerting on these specialists” (Male Medical Officer 7).
Communication and system-based barriers
All interviewed doctors discussed the challenges of truly integrating with palliative specialists.
“The palliative care team is not on-ground. They are at a different physical location and the team is also not in a very specific place. And so, it's always seen as an inconvenience and a lot of work to refer people to the palliative care team…The palliative care team will come but there is no known schedule that they will come everyday at like 10 or at 8…so it's very hard to plan around” (Female Medical Officer 5).
“It's unfortunate that most times the teams don't communicate with each other…what used to happen is that all these discussions would be within a tumor board or a clinical meeting…But this is not something common happening here. Because now the radiotherapy has its own discussion down there. We have our own discussion here. The palliative care team has its own discussion. So you find there is this haphazard” (Male Medical Officer Special Grade 6).
When interviewed doctors were asked to propose a management plan for two hypothetical patients with metastatic cancers, only 1/12 responses included a referral to a palliative specialist. Many doctors ultimately felt that coordinating care with palliative specialists was more of a challenge than a benefit. Nonetheless, all interviewed doctors emphasized there would be great benefit to enhanced collaboration with palliative specialists.
Discussion
Despite well-established benefits of early and integrated palliative care, there is ongoing difficulty in providing comprehensive palliative care in under-resourced oncology settings. Our study showed that UCI doctors not only have confidence in administering components of palliative care but also recognize the benefit of specialist involvement. Insufficient resources and logistical challenges contribute to a lack of collaboration between UCI doctors and palliative specialists, while cultural factors further complicate end-of-life care by limiting end-of-life conversations. This results in few advanced cancer patients being referred to palliative care specialists.
In our cohort, patients with worse ECOG performance statuses (3 or 4) were more likely to be referred to palliative specialists, aligning with the qualitative assessment by doctors—only the sickest are generally referred. This exclusive focus on performance status differs from the literature, where age and cancer type have been found to significantly influence which patients are referred to palliative specialists.29,30 The lack of importance of age at the UCI may be due to the relative youth of patients in our cohort; although other studies have shown higher referral rates for patients <65 years old, age may be less important when most patients are relatively young. Meanwhile, the fluidity in physician scope of practice at the UCI may explain the unimportance of cancer type, since most UCI physicians care for various cancer types, unlike the subspecialists cited in prior research.
Our study has several limitations. While the UCI is a cancer referral center for a population of >100 million people, the findings here only represent one treatment facility, raising concern about broad generalizability. Chart abstraction is limited methodologically 31 and only looks at decedents known by the UCI, meaning those who died at home without having the family notified the UCI were not included. Further, nearly 20% of medical files were not found. Finally, median survival after referral did not control for observed time.
Regardless, it remains important that limited available palliative resources are maximized. This is a real concern in regards to the 5-day median survival after palliative consult, as prior studies have observed, one- to two-month life expectancies after palliative consults.32–34
This phenomenon may be partially explained by the realities of working in SSA, where patients tend to present with late-stage disease and limited life expectancies. In addition, our cohort was comprised mostly of patients who had been hospitalized for cancer care and thus may represent a sicker population with more advanced cancer. Furthermore, since conversations about end-of-life care often do not happen or occur late in the disease process, the short life expectancy after referral may be a reflection of delayed end-of-life management plans. Finally, doctors might simply be misconstruing the life expectancies of their patients; nearly all doctors in our study overestimated life expectancy after referral.
However, while overestimation is not uncommon,39 the limited 5-day average survival highlights the need for earlier collaboration with palliative specialists. Such collaboration requires efforts to resolve inconsistent communication between care teams, as illustrated by uncoordinated clinical rounds and separate tumor boards. To further aid early management of terminal disease, care must also address cultural taboos specific to Uganda. While some Ugandans may not want to discuss issues surrounding death, the heterogeneity of the UCI patient population and the anecdotal stories above suggest that many patients do want to know their prognosis. A population survey in Kenya showed 57% of people would prefer to know their prognosis with terminal disease 36 ; a significant proportion of Ugandan patients likely want to know their prognoses too, although few patients are currently being engaged in such conversations.
More focused training is needed for doctors to comfortably address end-of-life issues in culturally sensitive manners. In addition, more research is needed in Uganda to elucidate patient preferences in end-of-life care and to provide outcomes data so that physicians can make timely, evidence-based referrals.
Ultimately, our research underscores the need for greater integration between oncology and palliative care. While such integration should be informed by recent international consensus regarding palliative integration, 37 it must also account for potential obstacles unique to resource-limited settings.16,38 Specific and locally relevant parameters are needed to guide early collaboration with palliative specialists and to help oncologists decide whom to refer.
Given the shortage of palliative care resources, an enhancement of palliative care proficiencies among physicians who treat cancer patients in resource-limited settings is also critical. Education emphasizing cross-cultural end-of-life care, recognition of imminent death, and how to approach conversations about death should be emphasized in medical training to improve doctors' management of nonsymptom-based palliative care in terminal cancer patients. As oncology and palliative care infrastructures expand in SSA, the region is uniquely poised to develop models for integrated care from the ground up.
Conclusion
Doctors at the UCI have confidence in administering many components of palliative care to patients with advanced cancer. When palliative needs surpass their skillsets, UCI physicians collaborate with palliative specialists as they are able. However, a lack of staffing and difficulty in interservice communication limits the degree of palliative integration at the UCI, and this is exacerbated by cultural discomfort in discussing issues surrounding death. This study highlights the importance of greater integration and enhanced palliative collaboration in regions of SSA where patients present with late-stage disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.