
Abstract
Abstract
Introduction:
With advanced-stage head and neck cancers, patients may develop large and/or complex wounds despite multiple reconstruction attempts. Wound coverage may require novel approaches to palliate the patient.
Method:
We present the case of a 56-year-old female with advanced squamous cell carcinoma of the scalp and skull who required multiple surgical interventions. Despite our best reconstructive efforts, the patient subsequently developed scalp infection and sepsis, necessitating further debridement for source control. She then required coverage of the exposed dura and skull to prevent further infection.
Results:
The calvarial wound was covered with a dermal regeneration template and held in place by a vacuum-assisted closure (VAC) device. This coverage prevented additional infection and morbidity, was relatively easy and comfortable to manage, and demonstrated healing and development of granulation. Unfortunately, the patient succumbed to her systemic cancer before application of a palliative split-thickness skin graft.
Conclusion:
A VAC device and dermal regeneration template constituted an excellent modality for managing the complex calvarial wound encountered by otolaryngology, neurosurgery, and burn/wound services. The technique provided appropriate palliation for a patient with advanced head and neck cancer.
Introduction
A
Despite rapid evolution of treatment options, prognosis for patients with locally advanced disease remains poor. 2 SCCHN is potentially curable in early stages (five-year survival 81%), but >60% of patients present with advanced disease (five-year survival 43%).2,4 Current multimodal treatment strategies include surgery, radiation, and chemotherapy. Introduction of pedicled myocutaneous flaps and microvascular surgical techniques allows for free tissue flap transfer; many patients treated today would have been previously considered inoperable. 5
But what happens when, despite best efforts, the disease progresses with resultant flap failures? Do we simply give up and tell our patients we have nothing more to offer, or do we involve other specialists who can offer a fresh look, and perhaps novel treatment options? We present a case of a 56-year-old female with advanced SCCHN who had undergone multiple surgical interventions, but had failed attempts at scalp reconstruction. We describe a novel solution to achieve cranial coverage with successful palliation until she succumbed to her systemic cancer.
Case Report
The patient was a 56-year-old woman initially evaluated in March 2014 for widespread fungating and ulcerated vertex and left parietal scalp tumor present for at least six months. She had “many years” of a pale scalp lesion in this region, previously diagnosed as discoid lupus. The patient's history included discoid lupus, smoking half a pack per day for 25 years, and drinking three to four cans of beer per day. Physical examination showed an irregular, raised, and ulcerated lesion, measuring 7 × 7 cm. Bilateral level V lymph nodes measuring <1 cm were palpable. Flexible endoscopy of her upper aerodigestive tract in otolaryngology clinic did not reveal any concerning lesions in her nasal cavity, nasopharynx, lower pharynx, base of the tongue, or larynx. Biopsy revealed SSC. MRI of the head and neck showed bilateral posterior neck lymph node prominence. A PET/CT showed bilateral level II and left posterior cervical enlarged lymph nodes (nontender on physical examination), suspicious for metastatic disease.
In April 2014, otolaryngology and neurosurgery performed a wide local excision of the scalp SSC, measuring 15 × 14 cm, left supraomohyoid neck dissection, left superficial parotidectomy, right level II excisional lymph node biopsy, parietal craniectomy with mesh cranioplasty, left latissimus dorsi myofasciocutaneous free tissue flap reconstruction, and split thickness skin grafting. The tumor invaded the skull, which was drilled away until normal appearing bone was encountered. The tumor had not invaded the dura mater. The patient was discharged home on postoperative day 7 doing well. Final intraoperative pathology confirmed moderately differentiated SSC with peripheral edges free of tumor; tumor extended to the deep margin and involved periosteum. The skin margins at 3–6 o'clock were noted to have superficially invasive moderately differentiated SSC, whereas margins at 6–12 o'clock showed no evidence of malignancy. No malignancy was present in the parotid gland or excised lymph nodes.
Incisions were healing well at first outpatient postoperative visit in May 2014 (Fig. 1). In July 2014, the patient completed radiation therapy with 60 Gy dose of 30 fractions. Unfortunately, in August 2014, head CT with and without contrast identified multiple new calvarial lesions.
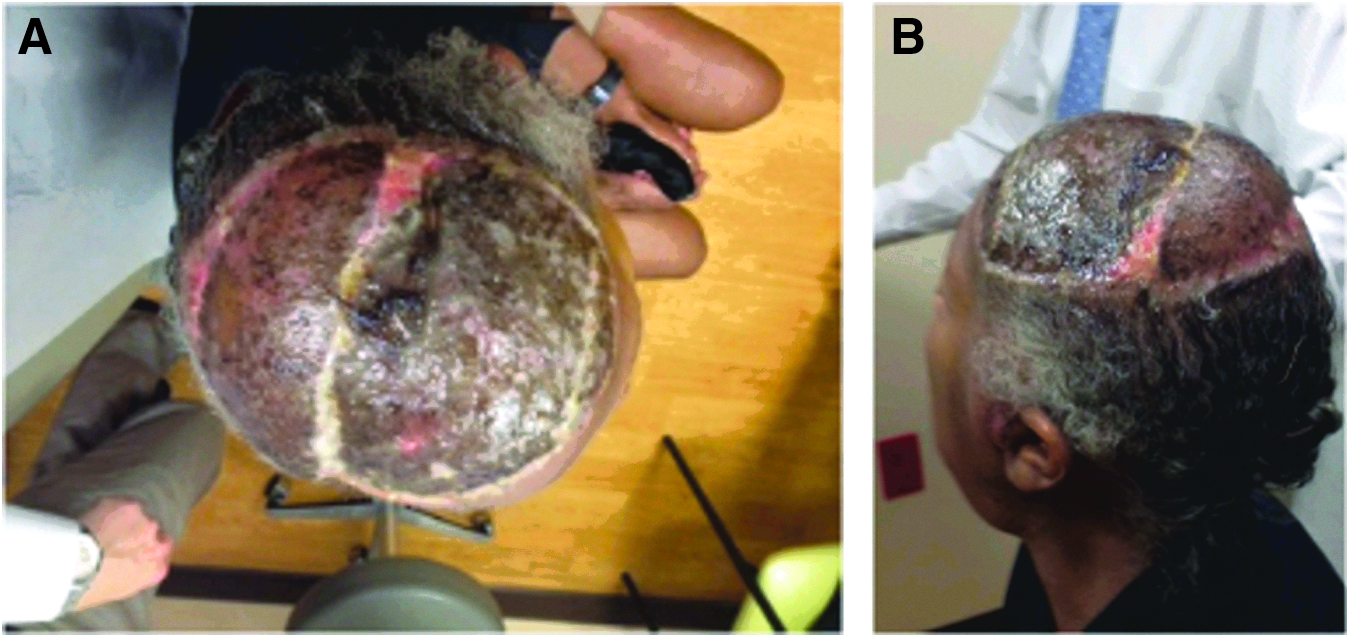
Second postoperative visit.
The patient had craniectomy for removal of new anterior frontal and left parietal skull lesions with drill out to normal appearing bone followed by titanium mesh cranioplasty, and primary scalp closure in September 2014. The scalp incision encompassed ∼60% of the scalp flap circumference, leaving the pedicle intact. The tissue overlying these areas on the scalp flap was trimmed away from the flap. During closure, faint duskiness of the flap in the areas where the underlining tissue was trimmed was noted. Postoperatively, the patient started hyperbaric oxygen therapy, completing 20 treatments.
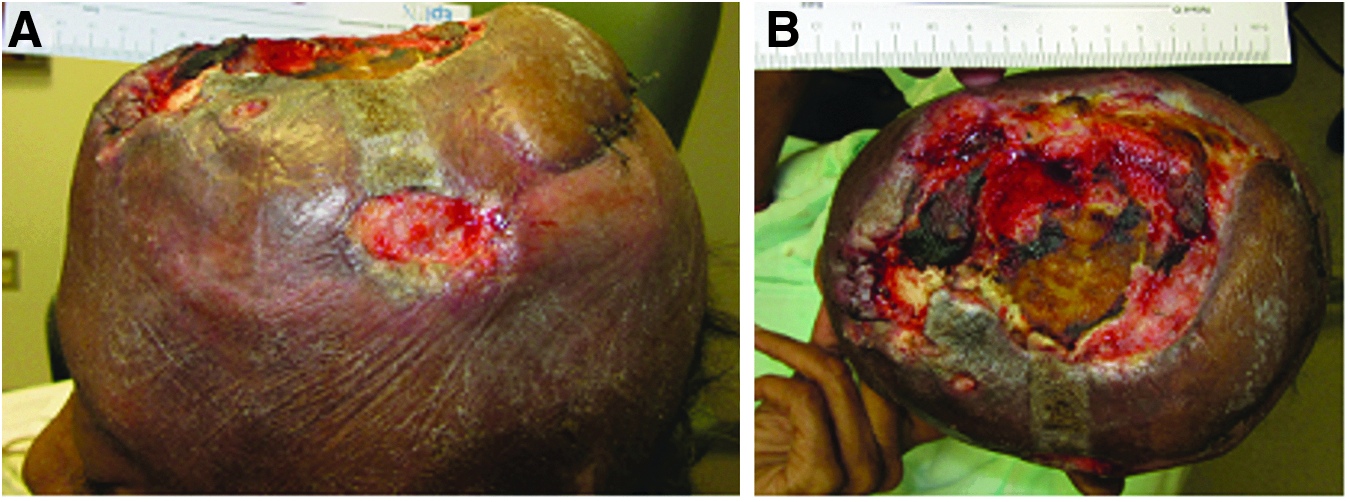
In October 2014, necrotic tissue was noted in the central aspect of the scalp wound and titanium mesh was exposed. The patient was instructed to change dressings twice daily to help debride the necrotic tissue. Palliative chemotherapy with carboplatin was started. In December 2014, the patient was readmitted to the hospital obtunded with infected wound and sepsis (Fig. 2). Admission laboratory studies revealed white blood cell count (WBC) of 9.4 × 10(9)/L, erythrocyte sedimentation rate of 97 mm/h, and C-reactive protein of 10.4 mg/dL. Wound culture grew methicillin-sensitive Staphylococcus aureus, Citrobacter freundii, and Enterobacter cloacae, treated with intravenous vancomycin and meropenem.

Photo taken of the patient's scalp wound defect during the December 2014 admission for altered mental status, wound infection, and presumed meningitis. This demonstrates failure of the cranial repair, and exposed cranioplasty mash with visible dura mater underneath.
Once the patient's level of consciousness improved, she had surgery by neurosurgery and by the burn/wound/acute care surgery team to remove the titanium mesh and release the cranial soft tissue flap. The underlying exposed dura was uninjured as was the surrounding intact cranium. A silver-impregnated dermal regeneration template was placed directly on the exposed dura and adjacent cranium, and was secured peripherally with dissolvable sutures. The wound flap was reapproximated, and a negative-pressure device was applied, set to −75 mm Hg after placing a nonadherent layer and silver-impregnated dressing directly over the implanted template (Figs. 2 and 3).

Intraoperative placement of silver-impregnated dermal regeneration template.
The vacuum-assisted closure (VAC) system was changed on postoperative days 8 and 12. On postoperative day 21, a portion of the dermal template had dried out and was clearly not viable (Fig. 4), so the patient returned to the operating room for further debridement of the head wound, including skull debridement and burr-hole placement, replacement of the dermal regeneration template, and reapplication of the VAC system with the same dressings and settings. The VAC system was subsequently replaced weekly for the next two weeks. On her last postoperative follow-up visit one week later, the patient's wound VAC was taken down revealing mostly well-adherent and granulating dermal regeneration template. The area over the exposed dura mater still had questionable viability. Granulation tissue was developing well >80% of the wound, though (Fig. 5). Unfortunately, before final skin grafting, she succumbed to her systemic cancer.

Intraoperative replacement of Primatrix bovine fetal collagen regeneration template before wound vacuum-assisted closure placement at second operation.
Photos from the last clinic visit, granulation forming over a majority of exposed calvaria with some negative pressure wound therapy discoloration of silver-foam wound nearly ready for skin grafting at this visit after some judicious intraoperative debridement.
Discussion
As this case illustrates, treatment of SCCHN can be challenging. Current treatment strategies for SCCHN include combination of surgery, radiation, and chemotherapy. Treatment of locally advanced SCCHN is complicated by disease site and volume, prognosis, functional deficits associated with therapeutic choices, therapy-associated toxicities, and needs and condition of individual patients. 2 Ablative surgery can result in significant cosmetic and functional morbidity, making reconstruction an essential part of initial surgical evaluation and management. 5 Pedicled myocutaneous flaps and free tissue flaps can be essential components of surgical treatment. 5
Usually scalp and forehead defects <3 cm diameter can be closed primarily. Larger defects may be more difficult because galea is relatively inelastic. 6 Excessive tension can result in ischemia, resulting in wound dehiscence, scarring, disfigurement, and alopecia. Guerrissi 7 reported a series of 21 patients with defects from 10% to 60% of scalp surface area, reconstructed with local flap advancement based on blood supply centered around superficial temporal, posterior auricular, and/or occipital arteries. The donor area was covered with skin graft. Various free flaps, such as lattissimus dorsi and rectus muscle flaps and scapular system, anterolateral thigh, and radial forearm fasciocutanous flaps, can then be applied. 5 Options are limited if these flaps fail.
Integra (Life Sciences, Plainsboro, NJ) is a bilayered dermal regeneration template of artificial skin for treatment of life-threatening third-degree burn wounds throughout the body. It consists of a layer of bovine type I collagen, chemically modified with the addition of glycosaminoglycans, and is coated with an adherent layer of silicone to form a bilaminar matrix. The collagen matrix serves as a dermal regeneration template, whereas the silicone functions as an artificial epidermal barrier to fluid. Once it has been grafted onto a wound for three to six weeks, a neodermis is generated by capillary ingrowth; the silicone layer loosens and is easily removed. An ultrathin (0.004–0.006 inch) autograft can then be applied. Yeong et al. 8 described two patients with severe head burns involving the calvarium treated with this technique. They concluded that compared with split-thickness skin graft, this technique provided a thicker coverage for wound closure. Importantly, these procedures were ultimately performed in a relatively sterile wound bed, an important consideration. In another small series, six cranial wounds were closed with the dermal regeneration template, resulting in five of the six wounds completely healing with cosmetically acceptable results. 9
A dermal regeneration template has been used off-label to aid in closure of full-thickness excision for BCC, SCCs, and melanoma. 9 The template simplified wound care, subjectively appeared to decrease pain and postoperative bleeding, and yielded cosmetically acceptable wound repair. Autografting was not necessary; wounds healed in two to four months by primary epithelialization over neodermis after removal of the silicone layer.
Negative pressure dressing is an adjunct in repairing many wounds, including those involving the head. However, its use in repair of cranial defects is limited.10–15 In noncranial sites, negative pressure dressings provide advantages of control and removal of wound secretions, reduction of edema and bacterial load, growth of granulation tissue and angiogenesis, increasing localized blood flow, and epithelial migration. 16 Early skin reapproximation and promotion of granulation tissue may avoid the necessity for complex reconstructive surgery. 16 Gumus 11 noted that vacuum-assisted dressing accelerated separation of necrotic bones and stimulated granulation tissue formation in burned calvarium. Powers et al. 12 described using VAC for 16–91 days (in five patients with complex cranial wounds from etiologies including trauma, SCC, and malignant meningioma). Cutaneous wound defects measured as large as 15 cm in diameter. Four of five patients had open skull defects with concomitant dural defects, and one patient had dural dehiscence. After surgical debridement, all five patients were treated with direct VAC device application to reapproximated dura, pericranial flap, or regenerative tissue matrix overlying central nervous system tissue. In all cases, the VAC device promoted granulation tissue formation over the dural substitute, prevented cerebrospinal fluid leakage, and kept the wounds free from local infection.
We developed an individualized treatment plan for our patient based on the mentioned studies and experience with noncranial wounds. Wound care decisions in this patient were complicated by the continued presence of malignancy as well as infection causing sepsis. Although the Integra bilaminar skin substitute is an excellent product for many cases, in this case it would have been inappropriate initially because of the infected state of the wound bed, and would likely have failed, even after aggressive debridement. The Primatrix 17 (TEI Biosciences, Boston, MA) bovine fetal collagen dermal regeneration template used in this patient is much more resistant to infection, yet still aids in the formation of granulation and a “neodermis” over which a skin graft may be placed. Furthermore, a silver-impregnated variety, inherently resistant to infection given the presence of ionic silver, was utilized to reduce the risk of infection reoccurring. 18 Finally, negative-pressure wound therapy, with or without the use of silver-based dressings, which has been shown to have pleiotropic effects on wound healing through microdeformation of recipient tissues, immune alteration of wound beds, and possibly by altering the bioburden of wound beds, 19 was used. In our case, a multimodal approach to attempt wound closure worked best with this patient's end-stage disease process, infected wound bed, and end-of-life wishes.
Conclusion
A VAC device with a dermal regeneration template can provide an excellent framework for managing complex calvarial wounds. This technique helped promote development of a healthy wound base, accomplishing goals of accelerating wound healing and maintaining patient comfort. In patients too frail or with diseases too advanced to undergo conventional flap reconstructive procedures, usage of dermal regeneration technology and negative pressure dressings can still accelerate wound healing and allow for eventual wound closure.
Footnotes
Acknowledgment
This work was supported by research funds from Division of Neurological Surgery, University of Missouri-Columbia School of Medicine.
Author Disclosure Statement
No competing financial interests exist.