
Abstract
Abstract
Background:
Persons with cystic fibrosis (CF) experience high morbidity and mortality, yet little is known about their palliative care needs and how clinicians may address these needs.
Objectives:
(1) To identify palliative care and advance care planning needs of patients with CF and their families; and (2) to identify clinicians' potential roles in meeting these needs.
Methods:
A mixed-methods study of adult patients (age ≥18 years) with moderate-to-severe CF [forced expiratory volume in the first second (FEV1) <65% predicted] were recruited from a CF Center. Semi-structured interviews (30–60 minutes) and questionnaires were administered in person or by phone. Grounded theory was used to analyze the interviews. Questionnaires were analyzed descriptively.
Results:
Forty-nine patients (FEV1 % range = 19%–63%) participated; the participation rate was 80% for eligible patients. Three main domains of palliative care needs were identified: (1) to be listened to, feel heard, and be “seen”; (2) understanding the context around CF and its trajectory, with the goal of preparing for the future; and (3) information about, and potential solutions to, practical and current circumstances that cause stress. In questionnaires, few patients (4.3%) reported talking with their clinician about their wishes for care if they were to become sicker, but mixed-methods data demonstrated that more than half of participants were willing to receive palliative care services provided those services were adapted to CF.
Conclusion:
Patients expressed a need for and openness to palliative care services, as well as some reluctance. They appreciated clinician communication that was open, forthcoming, and attuned to individualized concerns.
Introduction
C
The goals of palliative care are consistent with the Cystic Fibrosis Foundation's mission “to improve the quality of life for those with the disease” (www.cff.org), but a number of additional factors have impeded its implementation and assessment. First, the lack of formal guidelines directing palliative care8,9 has resulted in variability in its provision to patients with CF. Second, although some studies have proposed models for training providers to deliver palliative care to patients with CF,8,10,11 little research has been done that identifies palliative care needs of patients with moderate to severe CF and, therefore, provides little direction for addressing those needs.12,13 Third, although palliative care would benefit CF patients who cope with life-long symptoms and burdensome self-care routines, they tend to associate the concept with EOL rather than quality of life. Despite a growing consensus that patients with chronic respiratory diseases 14 should receive both “primary palliative care” (delivered by the clinicians already caring for patients and their families) and “specialty palliative care” (delivered by palliative care specialists), 15 there are few guidelines available to show how to implement these models of care. Finally, most CF centers lack methods to integrate palliative care into their multidisciplinary CF programs. They do not routinely discuss goals of care and advance care planning (ACP) is often only discussed during a hospital admission.13,16 As with other diseases, the failure to integrate palliative care into a holistic approach to CF care may lead to potentially inappropriate use of aggressive life-sustaining treatments before death17,18 and the use of treatments that may not be desired by fully informed patients. 19
Because of certain unique aspects of CF, including the age of the population and the lifelong nature of their illness, we hypothesized that existing models for delivering palliative care for patients with serious illness might not be appropriate.8,10 Therefore, we undertook a mixed-methods study of patients with moderate to severe CF to understand patients' perspectives on their palliative care needs and explore ways to meet those needs.
Methods
Sample
Eligible patients included adults (≥18 years) receiving routine care at the University of Washington (UW) Adult Cystic Fibrosis Center, with moderate to severe CF lung disease [forced expiratory volume in the first second (FEV1) % predicted <65%]. Participants were recruited consecutively and in person at clinic or by phone following a clinic visit.
Measures
The primary aim of our study was to explore and identify unmet palliative care needs for patients with moderate to severe CF lung disease. We used a mixed-methods design that allowed us to assess both quantitatively and qualitatively the character and scope of unmet needs, assess participant interest in receiving palliative care in specific situations and ask about specialist palliative care interventions.
Interviews
Semi-structured, one-on-one, 30- to 60-minute interviews were conducted with the goal of identifying and exploring patients' unmet palliative care needs. Open-ended questions and follow-up prompts guided conversations about domains of participants' needs, including (1) quality of life and symptoms, (2) communication with clinicians, and (3) palliative care services. Participants were encouraged to share examples of their experiences related to the topics introduced in the interview guide (Appendix 1).
Questionnaire
We assessed the following: (1) acceptability of specific palliative care services, (2) occurrence and desire for goals of care discussions before when the respondent would become too sick to speak for him/herself, and (3) barriers and facilitators to participating in discussions about goals of care. The items that assessed the acceptability of palliative care services were investigator-developed and included referral to specialty palliative care, participation in ACP discussions and activities (e.g., having a chance to complete ACP documents such as advance directives), and attending facilitated family conferences at which goals and preferences for future care are discussed18,20–23 (Appendix 2). The items used to assess the occurrence and desire for goals of care discussions, as well as barriers and facilitators to having those kinds of discussions, were evaluated with validated items.24–28 We also collected demographics and self-reported health status.
Data collection
All interviews were conducted by a single researcher trained in qualitative research (M.R.H.). Interviews were digitally audio-recorded and transcribed. All recordings were converted to deidentified documents by a medical transcriptionist. After the interview, participants were asked to complete the questionnaire. The study was approved by the UW Human Subjects Division and participants provided written or telephone consent.
Analyses
A modified grounded theory approach was used to analyze the qualitative data. 29 To develop our code book, four members of the team reviewed 6 transcripts, identifying and defining codes and their properties, and two investigators who are CF pulmonologists reviewed deidentified passages and codes to provide clinical insight. All transcripts were coded by one investigator using Dedoose (www.dedoose.com). To ensure trustworthiness of our coding, an additional 13 transcripts were coreviewed by three members of the team. Any differences were resolved by consensus. Agreement was achieved on 90% of the qualitative excerpts, indicating coding reliability. For participant characteristics and questionnaire data, we report descriptive statistics.
Results
Sample
We interviewed 49 of 61 eligible patients (80% participation; Fig. 1) who provided 46 questionnaires (75% participation). Participants had an average FEV1 41% predicted (standard deviation 12%; range: 19%–63%; Table 1).

CONSORT flow diagram. FEV1, forced expiratory volume in the first second
The mixed race patient was white/black.
FEV1, forced expiratory volume in the first second; SD, standard deviation.
Interview findings
We identified the following three domains of palliative care needs in our qualitative interviews: (1) to be listened to, feel heard, and be “seen”; (2) understanding the context around CF and its trajectory, with the goal of enabling planning and preparation for the future; and (3) information about, and potential solutions to, practical and current circumstances that cause stress (Table 2).
ACP, advance care planning; CF, cystic fibrosis.
The need to be listened to
The need “to be listened to, feel heard, and be ‘seen,’” emerged from participants' descriptions of attentive, empathic, and accepting clinician behaviors that were identified as helpful and supportive. They included being treated respectfully and thoughtfully, being supported when they shared their concerns about symptoms or other personal concerns, and taking into account patients' perspectives on their care. Participants noted that they appreciated their doctor listening respectfully when they confided in them: “As long as I feel they are considering me beyond just the medical—open to listening to me and considering that in how they deal with me.” Participants who said their doctors were good listeners confirmed that they were comfortable being vulnerable in patient–provider interactions: “They've known me for 20 years and because I have these really strong relationships with the CF team—they are really helpful.” Participants with established relationships with their CF provider felt a sense of security that their provider would be present and responsive.
Patients disclosed needing support when they were overcome by feelings of frustration, discouragement, or depression: “I think it would be good to have emotional support for conversations where you're saying, ‘Hey, I need to know…I'm a person with CF and it's overwhelming and sometimes I just want to be able to talk to someone who can empathize and give me some tools in the arsenal.’” At times, this meant acknowledgement of the difficulties associated with having a serious illness: “The doctor actually came along and sat with me for quite a while, as [I] was having a very emotional time about losing my independence. And it meant a lot… It's the little things in life that show, hey, somebody cares.”
Another area of importance to participants was the knowledge that their doctor was familiar enough with them as individuals to tailor care and communication accordingly. Significantly, they were open to seeing a palliative care provider but several patients commented that it would be important that this provider was familiar with CF; they did not want to have to explain CF to other non-CF providers: “It would be nice if taking care of my issues was incorporated. I didn't even realize that I could get other help.”
The need for context around CF and its trajectory
Respondents also discussed the need to place CF into the context of their lives going forward with the assistance of a clinician. By proactively initiating discussions related to disease progression, clinicians could alleviate some of the participants' worries about their illness: “Talking about getting sicker than I am currently never comes up, but more knowledge and discussion about potential next steps of sickness would be very helpful.” Participants also recommended that clinicians introduce these types of conversations about disease progression early and when they were feeling well, rather than waiting until they became sicker: “For them [the care team] to open it up, so you at least get started thinking, so it's not a new thing, like when it comes up for the first time because you're sick.” Participants indicated that “the future” felt easier to address when the CF care team brought the topic up with some reassurance and explained the role: “I think, to be told, upfront, first and foremost, ‘Okay, you are well… This doesn't mean anything to your current level of health. You're not going to die any time soon. But we should think about the future, if anything were to happen, let's get this in place now so that… nobody has to deal with it later. Yes, we know that it could be difficult to talk about, but we're here to support you.’” For the most part, patients hoped to discuss the prospect of getting sicker with a clinician they know and trust.
Need for information
Participants described a need for information about, and potential solutions to, practical and current circumstances that were sources of stress and concern. These included (1) managing their responsibilities at work despite having ongoing symptoms (e.g., low energy and coughing); (2) getting assistance with tasks that arise because of health and healthcare issues such as financial, insurance, and legal issues; and (3) planning for the future. Responsibilities at work felt more daunting when they were sick. Some patients were aware that they were sacrificing their health by prioritizing job performance, but were concerned about reducing hours or talking with their doctor about how to arrange for accommodations: “It wasn't until I brought up the question of, ‘I think I'm to the point where I can't work and do everything’ is when that conversation started with the doctors…there were a couple times where I got sick and they had said, ‘Well, you should back off work and maybe take some time off,’ and I kind of just pushed that aside.” For some participants, work was central to their identity as a functioning individual.
Patients consistently mentioned that they needed assistance with navigating tasks such as going on disability or Medicaid and securing medication. One married participant said, “It gets really expensive, really quick. And as I get older, I'm like…how is that all going to work in the future? We have to make enough money to pay for it… it's hard.” Patients admitted they could barely stay on top of the costs of medications, let alone tackle signing up for social security, even with the help of a social worker. Participants also noted that health insurance and legal issues were areas with which they would like guidance: “I do have insurance through work … but I could wake up tomorrow and not be able to go to work.” Some patients recognized that they needed resources but were unsure where to find them.
Finally, although only a small number of patients reported having completed ACP activities when asked on the survey (n = 2, 4%), in interviews they acknowledged this apprehension and reluctance but also the importance of completing advance directives such as living wills and a durable power of attorney for healthcare. They described being unclear about the steps they would actually take to complete these documents. One single man in his mid-thirties said, “Getting a living will and power of attorney is something that has kind of been on my agenda. I know I need to get done…” Several patients noted that their care team had not yet communicated with them about when and how to document their wishes, and that they felt they could defer planning, assuming their loved ones would honor their preferences. However, some participants were aware that leaving decisions up to others could create distress for their loved ones in the future.
Questionnaire findings
On items assessing respondents' willingness to use palliative care services, ∼60% of patients endorsed being “very willing” to be referred to a palliative care consultant, to participate in ACP, and to discuss goals of care with their family and doctor. Less than 15% of respondents indicated little or no interest in participating in these palliative care activities (Fig. 2).
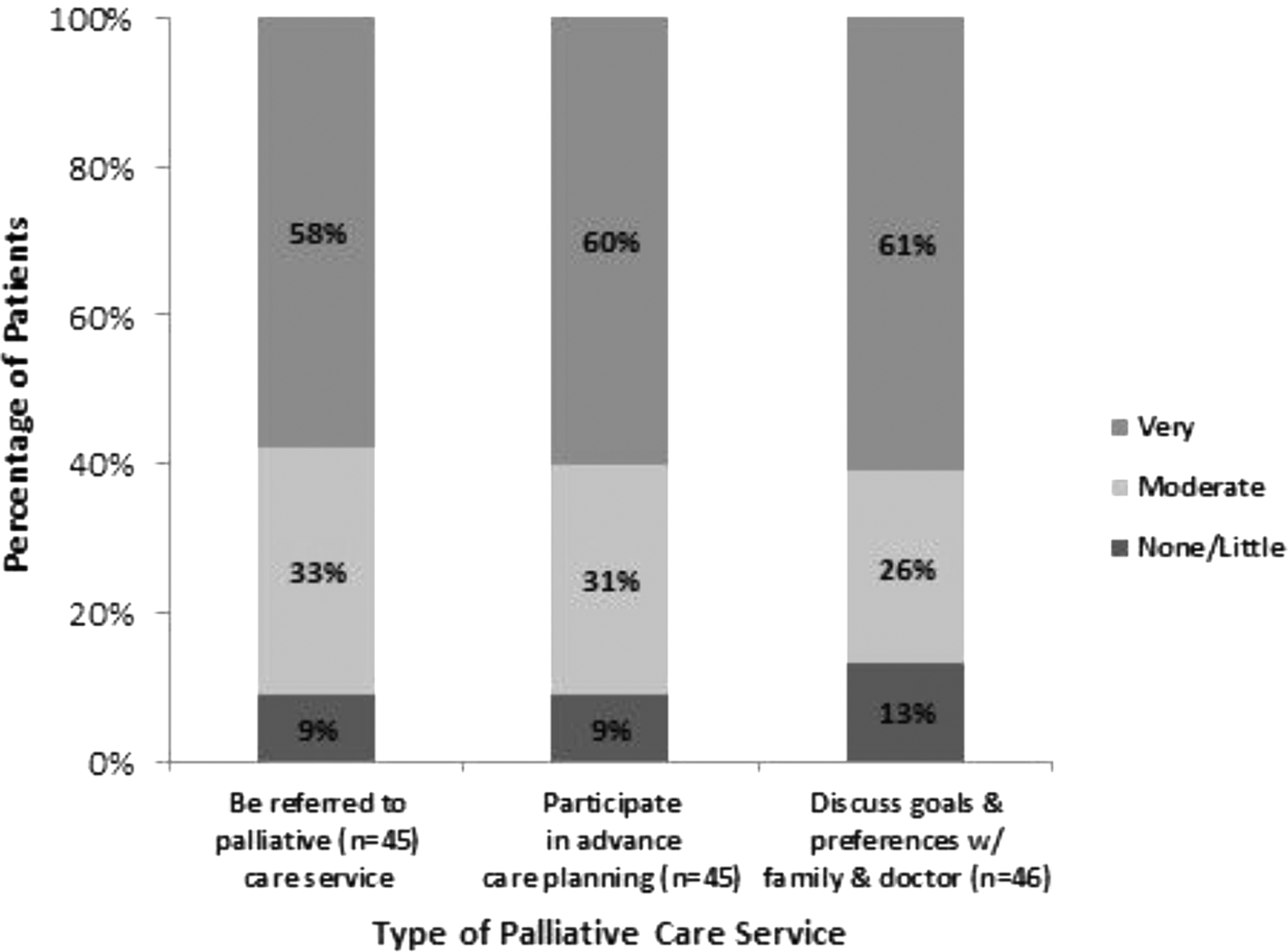
Patients' willingness to use palliative care services.
When asked about occurrence of and desire for goals of care discussions before when the respondent would become too sick to speak for him/herself, patients indicated they could imagine having these types of serious conversations, but nearly all had not had them to date. In response to the question, “Have you ever discussed with your CF doctors, in a face-to-face discussion, the kind of medical care you would want if you were too sick to speak for yourself,” over 90% of respondents indicated that they had not. When asked whether they would like to have such a discussion, about 50% were unsure, and 40% did not. Only 10% endorsed wanting to have this discussion with their CF doctors (Fig. 3). By contrast, when patients answered similar questions about serious discussions with family—∼60% recalled having discussed issues related to ACP with their family and almost 70% of patients with prior family discussions were supportive of having additional discussions (Fig. 4). Even among patients who had not previously had a discussion with family, 44% indicated that they would be in favor of beginning this discussion (Fig. 4).
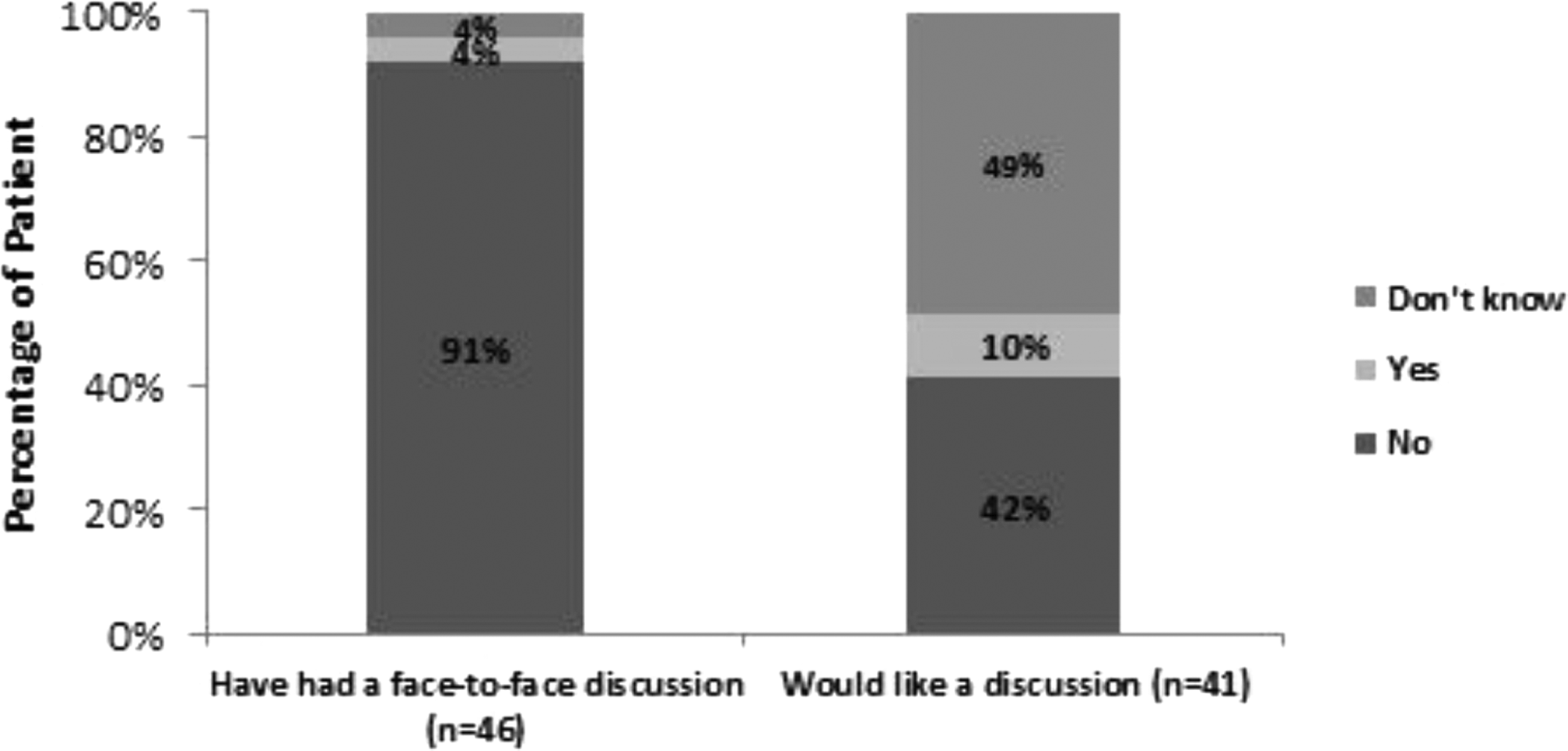
Patients' experience with and attitudes toward serious discussions with doctor.

Patients' experience with and attitudes toward serious discussions with family.
In responses to questions about barriers or facilitators to serious illness communication, a third or more of patients indicated that they didn't like to talk about getting very sick (36%) and would rather concentrate on staying alive (33%). Patients mentioned some practical barriers, noting that their doctor didn't seem to have the time to have a serious illness discussion (35%), and that they were not sure which doctor might be taking care of them when they became very sick (32%) (Table 3). More than half of patients endorsed each of the four facilitators, with the highest endorsements for the two items about thinking and planning for the future: “I worry about the quality of my life in the future” (60%), and “I worry that I could be a burden on friends/family if I were to become very sick” (57%) (Table 4).
EOL, end of life.
Discussion
Our findings from this mixed-methods study of palliative care needs of patients with moderate to severe CF lung disease indicate a number of unmet needs as well as openness to addressing these needs through engagement with CF providers and palliative care specialists.11,30,31 This openness was supported strongly in the interview data and somewhat less so in the survey data, where only 10% of respondents endorsed wanting a discussion with their CF doctor about care if they became too sick to speak for themselves. However, even in the survey, when asked about services and activities to which they would be open, greater than half of respondents reported a willingness to be referred to palliative care, to participate with their CF clinician and family to discuss future goals and preferences, and to participate in ACP that would specify their wishes and values regarding future care. Some of the apparent contradictions in our findings may be attributed to differences associated with different data collection methods, but these results suggest considerable ambivalence toward goals of care discussions. These different approaches, both qualitative and quantitative, and the findings they elicit, are the strength of mixed methods; they may yield, taken together, a more complete understanding than could be obtained with a single approach. 32
In our qualitative research, we found that adults with CF experience concerns about loss of functioning, independence, increased symptoms, and complex CF treatments. Participants were open to having these palliative care needs addressed by their CF clinicians during clinic visits if (1) they could talk with a provider with good communication skills, (2) topics were broached thoughtfully, and (3) they could decline to talk or talk only as much as they felt comfortable. In both our qualitative and quantitative data, we found that respondents identified easier or harder times during which to have these discussions. In interviews, our participants felt that that bringing up palliative care should not be done by their doctor at visits when a patient is feeling poorly or “is receiving bad news.”15,33,34 These circumstances included (1) being diagnosed with an exacerbation, (2) being told that their lung function is dropping, or (3) being asked to consider lung transplant. On the questionnaire, we found that the major barriers to goals of care conversations were as follows: not wanting to talk about becoming sicker; not feeling sick enough; and not knowing which doctor might be taking care of the respondent were he/she to become very ill. It seems likely that these issues and barriers will need to be addressed to effectively facilitate goals of care discussions. For the most part, participants conveyed receptivity to the idea of talking about quality of life concerns with their CF doctor.
We also found that many patients were open to talking to their CF clinician about their fears and worries associated with living with a serious illness and about ACP. This finding aligns with previous research that has proposed that patients are willing to talk with their clinicians about their needs, but the context and framing of these discussions are critical.8,11 In our study, patients with CF reported that they cope with stresses associated with their illness daily, and they felt that primary palliative care from CF clinicians could reduce pressures related to finances, relationships, housing, or medication. Consistently, they agreed that CF clinicians could do more to encourage them to express their needs on a regular basis. Participants varied in the quantity and quality of their needs; however, they agreed that they wanted their CF clinician to be attentive, caring, receptive, and supportive.
In the qualitative interviews, patients acknowledged the importance of goals of care discussions and their role in guiding care during illness progression, but also recognized the difficulty of these conversations. Despite some reluctance, most of our participants were open to goals of care discussions with their CF clinicians under certain conditions: (1) giving patients some control over the circumstances and content of the discussion, (2) having these discussions when they are not experiencing an exacerbation, and (3) ensuring sufficient time so that conversations do not feel rushed or distracted. This concern—that doctors may not have sufficient time to have these conversations—was also identified in the survey data as a barrier to goals of care discussions with their clinicians. Our respondents observed that clinicians should initiate ACP discussions if they did so with sensitivity and reassurance that ACP is a process by which patients can ensure that their goals and values that will guide future care are known and understood. Drawing from both data sources, most participants were willing to see palliative care specialists, but several commented that it should be someone who understands CF so they don't have to explain their disease to non-CF clinicians. Participants also reported that involving the family was important, and many had already discussed their wishes with their family/friends. Our findings resemble those from other studies that show that discussions about ACP are not part of regular CF clinical care11,17,18,22,35 and that ACP often happens too late for patients to direct their preferences for EOL care.13,35 This guidance from our participants may be helpful in overcoming resistance to ACP discussions.11–13,20,22
Our study is limited by being conducted in a single CF Center and may not be generalizable to other settings. In addition, response bias may exist, since participants may have been more open to talking about palliative care than those who did not participate. We also were only able to recruit people who were seen in clinic during the study period; thus, we may have missed individuals with more infrequent or irregular visits. Finally, our qualitative methodology emphasizes patterns found in the experiences of participants; future studies will be needed to examine the prevalence or frequency of these experiences.
In summary, we found that patients with CF have identified a broad range of palliative care needs. Addressing these needs during times of wellness in a forward-thinking and nonurgent setting was highlighted consistently. Palliative care needs may be best addressed by providers who can listen empathetically, be responsive to both near-term and long-term concerns, and be skillful in supporting ACP discussions. We also found that, although patients with CF endorsed the importance of primary palliative care from CF clinicians, most were open to seeing palliative care specialists and participating in ACP and family conferences, provided the palliative care providers understand CF. Further studies are needed to identify ways to use these findings to integrate primary and specialty palliative care for patients living with CF.
Footnotes
Acknowledgment
Funded by the Cystic Fibrosis Foundation (Grant No. AITKEN14Q10).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.