
Abstract
Abstract
Background:
Prognostic uncertainty is common in advanced cancer and frequently addressed during palliative care consultation, yet we know little about its impact on quality of life (QOL).
Objective:
We describe the prevalence and distribution of distress due to prognostic uncertainty among hospitalized patients with advanced cancer before palliative care consultation. We evaluate the association between this type of distress and overall QOL before and after palliative care consultation.
Design:
Observational cohort study.
Setting & Participants:
Hospitalized patients with advanced cancer who receive a palliative care consultation at two geographically distant academic medical centers.
Measurements:
At the time of enrollment, before palliative care consultation, we asked participants: “Over the past two days, how much have you been bothered by uncertainty about what to expect from the course of your illness?” (Not at all/Slightly/Moderately/Quite a Bit/Extremely). We defined responses of “Quite a bit” and “Extremely” to be indicative of substantial distress.
Results:
Two hundred thirty-six participants completed the baseline assessment. Seventy-seven percent reported being at least moderately bothered by prognostic uncertainty and half reported substantial distress. Compared with others, those who were distressed by prognostic uncertainty (118/236) reported poorer overall QOL before palliative care consultation (mean QOL 3.8 out of 10 vs. 5.3 out of 10, p = < 0.001) and greater improvement in QOL following consultation (Adjusted difference in mean QOL change = 1.1; 95% confidence interval = 0.2, 2.0).
Conclusions:
Prognostic uncertainty is a prevalent source of distress among hospitalized patients with advanced cancer at the time of initial palliative care consultation. Distress from prognostic uncertainty is associated with lower levels of preconsultation QOL and with greater pre-post consultation improvement in the QOL.
Introduction
P
This study addresses two key gaps in the science of prognostic uncertainty in palliative care for persons with advanced cancer. First, we assess the quality-of-life (QOL) burden that is associated with prognostic uncertainty among hospitalized patients with advanced cancer before palliative care consultation. Specifically, we describe the degree to which patients report prognostic uncertainty as being bothersome to them and examine the association between distress from prognostic uncertainty and overall QOL. Second, we examine whether changes in QOL before and after palliative care consultation are more pronounced for people who are distressed by prognostic uncertainty versus those who are not. These findings will improve our understanding of prognostic uncertainty in palliative care and, thus, contribute to the empirical basis for identifying, improving, and disseminating the ingredients of palliative care interventions that promote QOL in advanced cancer.
Methods
Overview
As described more fully elsewhere, 23 the Palliative Care Communication Research Initiative (PCCRI) is a multisite observational cohort study. We enrolled 240 hospitalized patients with advanced cancer at the time of referral for inpatient palliative care consultation; 236 responded to the prognostic uncertainty item and are included in this analysis. We include data from patient self-report before consultation and the day after the initial palliative care consultation, clinician self-report immediately following initial consultation; medical record, and six-months of mortality follow-up.
Participants
The parent cohort study took place at two large academic medical centers in geographically distant areas of the United States: the University of Rochester Medical Center (upstate New York) and the University of California San Francisco Medical Center. All English-speaking, hospitalized patients who were referred for inpatient palliative care consultation were eligible for this study if they met the following additional criteria: age >21 years, diagnosed with a metastatic nonhematologic cancer, not having a documented exclusively comfort-oriented plan of care at the time of referral, and able to consent for research either directly or via healthcare proxy (if lacking capacity as determined by the clinical team).
Measures
Prognostic uncertainty
At the baseline assessment, shortly before the study palliative care visit, we asked participants: “Over the past two days, how much have you been bothered by uncertainty about what to expect from the course of your illness?” (Not at all/Slightly/Moderately/Quite a bit/Extremely). As with all PCCRI self-report measures, we designed this item to be easily understood, valid, and low burden in the busy hospital environment to promote representative participation among a seriously ill population. 23 To achieve these performance criteria, we followed the single-item, multiconstruct approach of the successful Dartmouth COOP Chart field measures.24,25 The item question uses the validated language from the Dartmouth COOP “Feelings” Chart (i.e., “Over the past __, how much have you been bothered by…” 24 ) and the prognosis information language of the QUAL-E scale (i.e., “…about what to expect from the course of my illness” 26 ). We used the “past two days…” time period to offer a long enough time for stable estimate of the person's experience yet short enough to minimize the substantial shifts in clinical conditions that can occur during hospitalization among the seriously ill. During pilot testing of all study self-report measures, participants found the question easy to understand, response categories appropriate, and reporting burden low.
Quality of life
We assessed QOL using the McGill Quality-of-life Questionnaire global item: “Considering all parts of your life—physical, emotional, social, spiritual, and financial—over the past two days, how would you rate the quality of your life?” (0–10 scale from “very bad” to “excellent”).27,28 At the post-consultation assessment, we used the same item, but changed the time reference period to “today.”
Mortality
At the time of enrollment, patient-participants identified a key informant for follow-up contact. We obtained date of death from hospital records for those participants who died during the admission in which they enrolled in the study (i.e., index admission). For participants who were discharged from the index admission, we contacted them or their key informants by telephone at one and six months post-enrollment. We confirmed all reported deaths using hospital or obituary records.
Other analytic variables
Participants self-reported their gender, race/ethnicity, educational attainment, and religious affiliations. We evaluated financial strain by asking, “When you think about the amount of income that you have available in a typical month, how often is it enough for things you really need like food, clothing, medicine, repairs to the home, and transportation?” (None of the time/Some of the time/Most of the time/All of the time). We measured patient-participants' expectations for survival using the “likely”23,29 approach: “Would you say that it is likely or unlikely that you will live for a year or longer?” (Very Likely/Likely/Unlikely/Very Unlikely//No Idea). We asked the palliative care clinician to make their best guess about the patients' “most likely survival time, assuming that their illnesses are allowed to take their natural course.” Response options followed intervals that were commonly used in clinical practice at the study sites (<24 hours/24 hours to <2 weeks/2 weeks to <3 months/3 months to <6 months/>6 months). To assess dispositional optimism, we used a single item from the Life Orientation Test 30 : “How well does the following statement describe you? In uncertain times, I tend to expect the best.” (Not at all/Slightly/Moderately/Quite a Bit/Completely). As consistent with similar work using the Life Orientation Test, we identified high versus low dispositional optimism by dichotomizing responses at the median value.31,32 The dispositional optimism item was added during the enrollment period and asked of the final 184 participants only.
Analytic approach
We calculated the frequency and distribution of all study variables. For the five-category ordinal Prognostic Uncertainty measure, we categorized responses in two ways. First, we created approximate quartiles by combining the lowest two response options because the “Not at All” responses were too few for stable estimation (Table 1). Second, we dichotomized responses based on best estimates of a clinically important threshold. The root question and five-item ordinal scale is based on the well-established approach of the Dartmouth COOP Charts clinical screening measures. Receiver–Operator Curves for these measures indicate a threshold of 3 (worse than “Moderately”) for identifying clinically important levels of distress, 33 thus the COOP Project endorses interpretation that “high scores (i.e., patient rating of 4 or 5) represent unfavorable levels of health.” 34 Therefore, we categorized responses of “Quite a Bit” and “Completely” (i.e., 4 and 5) as distress. In our sample population, the clinical threshold definition was also the median split point. This distribution is beneficial for our descriptive epidemiology purposes because it minimizes the potential problem of unstable estimates (e.g., sparse data) in stratified analyses. We described the point estimate and 95% confidence intervals (CIs) for the prevalence of distress from prognostic uncertainty among the full sample and stratified by patients' socioeconomic and clinical characteristics. For statistical significance testing purposes, we used t tests for normally distributed continuous data, chi-square tests for nominal and binary categorical data, and Kruskal–Wallis tests for ordinal comparisons.
Defined as distress.
HS, high school; AA, African American.
For the change in QOL, we calculated the difference between the pre- and post-consultation ratings of QOL, each using the identical 0–10 scale. We calculated the mean pre–post difference and 95% CI for the full sample and for each quartile of prognostic uncertainty. We considered a difference of 0.5 SD to be a clinically important difference in mean. 35 We used a generalized linear regression model to evaluate whether the degree of change differed for those who were distressed versus those who were less bothered by prognostic uncertainty.
We evaluated potential effect measure modification using stratified analyses. We evaluated and adjusted for potential confounding using backward multiple regression modeling by evaluating the impact of potential confounder sets on the point estimate of association (i.e., odds ratios [ORs] for logistic models; difference in mean QOL differences for linear model). For each association, we identified potential confounders as those variables demonstrating association with the independent and dependent variable. For the association between prognostic uncertainty and the low/moderate/high categories of QOL, we used ordinal logistic regression.
This study was approved by the protection of human subjects review committees at the University of Rochester Medical Center, the University of California, San Francisco and the University of Vermont Medical Center.
Results
As shown in Table 1, participants' median age was 63 years (IQR from 54 to 71 years), half were women, two-thirds were financially insecure, 15% did not graduate from high school, and 24% self-identified as non-white. Approximately 1 in 10 participated by proxy.
Prognostic uncertainty was a substantial burden in the study population. More than 3 out of 4 reported at least moderately burdensome levels; half reported levels consistent with distress (Table 1). Distress from prognostic uncertainty was strongly associated with QOL (Table 2) and this association persisted when considering quartiles of the prognostic uncertainty item (Kruskal–Wallis p = < 0.001). People who were distressed from prognostic uncertainty had nearly three times the odds of their QOL ratings falling into a lower category (i.e., high vs. moderate vs. low) compared with others (OR = 0.36; 95% CI = 0.22, 0.56). These findings persisted after adjusting for age, gender, race, ethnicity, education, dispositional optimism, patient's perceived life expectancy, and proxy reporting status (ORadj = 0.31; 95% CI = 0.17, 0.57).
Strata-specific sample sizes might be less than 236 due to missing item responses.
Added to baseline questionnaire for the final 184 participants only.
CI, confidence interval; QOL, quality of life; EOL, end of life.
The prevalence of distress from prognostic uncertainty did not substantively differ by gender, race, education, financial insecurity, functional status, or clinician-rated survival prognosis. People who were distressed by prognostic uncertainty lived a similar amount of time as those who were less bothered by prognostic uncertainty (hazard ratio: 0.97; 95% CI: 0.73, 1.29).
Both dispositional optimism and patient expectations of longer survival (>1 year) demonstrated strong inverse associations with the prevalence of distress (Table 2) and these associations persisted when considering quartiles of the prognostic uncertainty item (Kruskal–Wallis p values 0.01 and 0.05, respectively).
We observed substantial interaction between Dispositional Optimism and Self-Rated Prognosis on the frequency of distress from prognostic uncertainty. Among patients who expected to live for at least one year, optimists were far less likely to report distress from prognostic uncertainty than nonoptimists (unadjusted OR = 0.13; 95% CI = 0.05, 0.39). We observed a statistically significant pattern of association between optimism and distress from prognostic uncertainty among those who expected to live one year (OR = 0.13), those who had “no idea” how long they might live (OR = 0.83), and those who expected to die within one year (OR = 2.05, model interaction term p = 0.001). As shown in Figure 1, these associations persisted after adjustment for potential confounding or exclusion of proxy reporting.
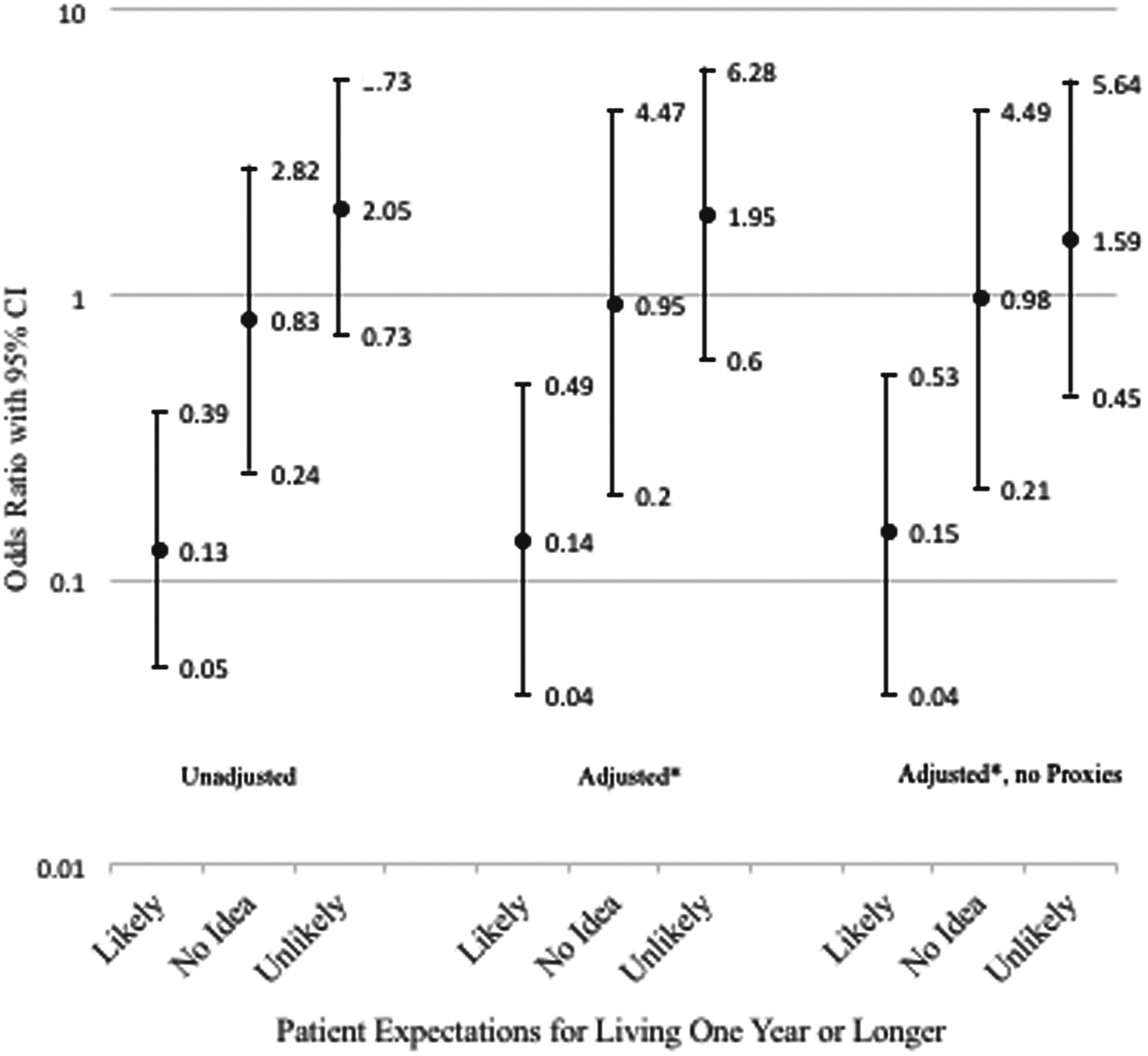
Association between dispositional optimism and distress from prognostic uncertainty, stratified by self-rated, one-year survival expectations. (adjusted for age, gender, race, ethnicity, education, quality of life, and proxy reporting status).
As shown in Table 3, those who were distressed by prognostic uncertainty before the palliative care consultation reported a greater magnitude of improvement in QOL on the day following the consultation. The degree of change among participants reporting distress preconsultation was greater than 0.5 SD, thus suggesting a clinically important improvement. 35
Magnitude of difference >0.5 SD.
Final model includes the following covariates: dispositional optimism, self-rated prognosis, and proxy reporting status.
Discussion
In this multisite study, we evaluated the prevalence, distribution, and outcomes of distress from prognostic uncertainty among hospitalized patients with advanced cancer who consulted with palliative care. Four of our observations are particularly important and merit further discussion. First, we observed that 9 out of 10 patients reported being at least slightly bothered by prognostic uncertainty near the time of palliative care referral and half were experiencing clinically important levels of distress. The prevalence of distress from prognostic uncertainty did not differ based on clinicians' expectations for survival time or actual survival time. Clinicians, patients, and families often avoid discussing prognosis in serious illness8,13,36–39 and not only miss important opportunities to discuss treatment preferences that might be prognosis sensitive, but also to recognize, understand, and address suffering caused by patients' awareness of prognostic uncertainty.
Second, we observed that people who were distressed from prognostic uncertainty had poorer QOL at the time of referral to palliative care. Our data cannot identify the causal direction of this association. It is possible that other drivers of QOL (e.g., pain or dyspnea) raise patient fears about what to expect as their illness progresses, thus increasing the burden of any perceived prognostic uncertainty. It is also possible that the emotional, spiritual, and existential distress of prognostic uncertainty lowers QOL. Most likely, these phenomena exist in dynamic equilibrium around the time of referral to palliative care. Communicating about prognosis is common in palliative care8–12 and our findings suggest that addressing prognostic uncertainty might be an important mechanism by which palliative care improves QOL in advanced cancer.1,40–42
Third, we observed greater—and clinically important—improvement in QOL following initial palliative care consultation among participants who were distressed by prognostic uncertainty compared with others. As described above, this is a descriptive epidemiologic study and these findings offer limited opportunity for causal inference. Given the baseline association between distress from prognostic uncertainty and poorer QOL, it is possible that our data may simply represent “regression to the mean.” However, emotionally attentive 43 prognosis communication is common in palliative care consultations9–11 and managing uncertainty is a key component of high-quality prognosis communication.3,13–16,21 Our findings point to prognostic uncertainty, specifically, to be an important target for QOL interventions in palliative care populations.
Fourth, we observed a clinically relevant interaction between dispositional optimism (i.e., tending to expect the best in uncertain times) and patient expectations for how long they were likely to live on distress from prognostic uncertainty. When participants expected that they would live for a longer period of time (i.e., more than one year), then optimists were less likely to experience distress than nonoptimists. However, this association differs for those who did not expect to live for at least one year. Indeed, optimists might be more vulnerable to distress from prognostic uncertainty as their awareness of end of life grows. These findings are descriptive and require confirmation, but raise important hypotheses that warrant further research. Optimism is a dominant and celebrated approach to uncertainty in Western cultures, particularly the United States. 44 For many, this approach fosters resilience sufficiently well to obviate the need for cultivating other “backup” methods for handling uncertainty. However, optimism as a personality trait may become dysfunctional in contexts with limited options for action, or when one is forced to confront the inevitability of death. In such circumstances, dispositional optimism may set people up for greater disappointment and emotional distress. More research is needed to explore these and other potential mechanisms. Our data suggest that optimists might be particularly vulnerable to distress from their appraisal of prognostic uncertainty as death nears, and may require additional support to promote emotional coping.
This study has important limitations. We included only English-speaking participants. Therefore, we do not know the experience of uncertainty among those who experience barriers to communication in English-speaking settings. Additionally, this sample includes academic medical center sites in California and New York; inferences about other geographic or institutional sites with substantially different cultural norms might not be valid. However, given the high prevalence of distress from prognostic uncertainty in our multisite sample, we expect that our findings remain relevant in most acute care palliative medicine settings. Third, this study uses single-item, multiconstruct “field” measures for the clinical setting that are brief, valid, and easy to complete. This approach makes it feasible for seriously ill and dying people to participate, but at the expense of construct specificity, estimate precision, and sensitivity to change.
In conclusion, awareness of prognostic uncertainty is associated with worse QOL for patients with advanced cancer who are referred for palliative care consultation. Palliative care consultation may benefit those who are suffering with this type of uncertainty. Dispositional optimism may be a risk factor for dysfunctional emotional coping with uncertainty as awareness about end of life grows. More research is needed to understand, support, and disseminate best practices for addressing suffering due to prognostic uncertainty in palliative care.
Footnotes
Acknowledgments
This work was funded by a Research Scholar Grant from the American Cancer Society (RSG PCSM124655; PI: R.G.). The authors thank the American Cancer Society and the palliative care clinicians, patients, and families who participated in this work for their dedication to enhancing care for people with serious illness.
Author Disclosure Statement
No competing financial interests exist.