
Abstract
Abstract
Background:
Communication is key in optimizing medical care when a child is approaching end of life (EOL). Research is yet to establish best practices for how medical teams can guide intrafamily communication (including surviving siblings) when EOL care is underway or anticipated for a pediatric patient. While recommendations regarding how medical teams can facilitate communication between the medical team and the family exist, various barriers may prevent the implementation of these recommendations.
Objective:
This review aims to provide a summary of research-to-date on family and medical provider perceptions of communication during pediatric EOL care.
Design:
Systematic review.
Results:
Findings from a review of 65 studies suggest that when a child enters EOL care, many parents try to protect their child and/or themselves by avoiding discussions about death. Despite current recommendations, medical teams often refrain from discussing EOL care with pediatric patients until death is imminent for a variety of reasons (e.g., family factors and discomfort with EOL conversations). Parents consistently report a need for honest complete information, delivered with sensitivity. Pediatric patients often report a preference to be informed of their prognosis, and siblings express a desire to be involved in EOL discussions.
Conclusions:
Families may benefit from enhanced communication around EOL planning, both within the family and between the family and medical team. Future research should investigate a potential role for medical teams in supporting intrafamily communication about EOL challenges and should examine how communication between medical teams and families can be facilitated as EOL approaches.
Introduction
A
It is widely accepted that communication is a key component of optimizing medical care when a child is approaching end of life (EOL).8,9 Ideally, when a child is faced with a terminal diagnosis and/or enters EOL care, his or her medical team takes a pediatric palliative care (PPC) approach, either integrating a palliative team or providing PPC themselves if a team is not available.10,11 PPC encompasses a child- and family-centered approach to care with a goal of enhancing quality of life by ensuring that EOL medical care is congruent to the family's physical, emotional, and spiritual values. 11
PPC facilitates communication between medical teams and families by addressing the goals and needs of the child and family.8,9 Benefits of effective communication have been demonstrated into the bereavement period. For example, higher parental ratings on communication have been associated with lower levels of long-term parental grief. 12 Many challenges may affect a family's ability to communicate with each other and with the medical team. For example, medical professionals may not know how to breach the subject of death and may avoid the topic to protect child, parents, and surviving siblings from distress. 13
Currently, research on intrafamily communication regarding pediatric EOL is in its infancy. Similarly, very little research is available on pediatric patient perspectives on communication with medical providers. To our knowledge, no review currently brings together the numerous small studies (majority include <100 participants) that have reported on parent perception of medical provider communication at EOL or medical providers' perception on communication with families. Thus, the purpose of this systematic review is to summarize current research on how families communicate with each other and with the medical team when a child requires EOL care with a goal of informing clinical practice and highlighting avenues for future research.
Method
Search strategy
A search of PubMed, Medline, and PsycINFO between January 1, 2000 and September 1, 2017 was performed using the following search terms: “terminal care,” “end-of-life care,” “palliative care,” “pediatric,” “child,” “parent,” “family,” and “communication.” For those studies that met eligibility criteria, reference lists were also reviewed. If a title of an article in a reference list suggested that it could potentially qualify for the current article, the full text of that article was reviewed.
Study selection
Two study authors independently reviewed titles and abstracts of potential studies identified in the initial search to determine which studies were eligible for inclusion in the full text review. Eligibility criteria were defined as the following: the study had to (1) include information on a child currently receiving EOL care/PPC or a child who had received EOL care/PPC before their death, (2) focus on communication within the family or between family and the medical team, (3) be available in the English language, and (4) be published between January 1, 2000 and September 1, 2017. Both qualitative and quantitative research methodologies were included. Intervention studies were excluded.
Results
Characteristics of included studies
The initial search of PubMed, Medline, and PsycINFO yielded 115 results. Overall, findings from 65 studies were included: 9 examined EOL communication within the family, 43 reported on the families' perspective on communication between the family and medical team, and 17 offered perspectives of healthcare providers on communication with families at EOL, with 4 of these studies examining more than one category of communication listed above.13–16 Figure 1 depicts study design with PRISMA diagram, and Tables 1–3 show descriptions of studies selected for inclusion.
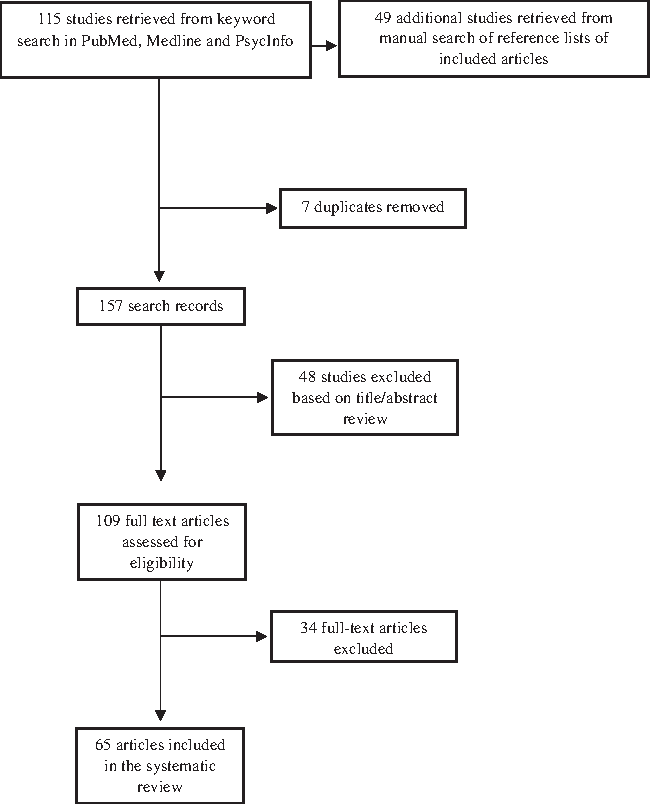
PRISMA diagram for studies of patient, family, and medical team communication during pediatric palliative care (2000–2017).
EOL, end of life.
PICU, pediatric intensive care unit; NICU, neonatal intensive care unit; PPC, pediatric palliative care; ACP, advanced care planning; DNR, do-not-resuscitate.
LSMT, Life-sustaining medical treatment.
Of the 65 included studies, 1 took place in South America, 35 took place in North America, 22 in Europe, and 1 in both Europe and North America. A total of six studies took place in Australia and New Zealand and one in East Asia. A total of 30 studies focused on children receiving EOL care for cancer, 8 on patients with heart conditions, 4 on children with neurological issues, 1 on conditions involving seizures, 1 on conditions causing respiratory failure, 3 on brain tumors or abnormalities, 9 on complications from multiple, perinatal, and premature births, 3 on genetic or chromosomal abnormalities, 1 on gastroenterological issues, and 36 on a combination of life-limiting conditions.
Study participants
Sample sizes for the studies ranged from 7 to 13 pediatric patients,17,18 7–18 siblings,19,20 4–429 parents,16,21 and 9–446 healthcare providers.22,23 One study focused solely on the perspectives of pediatric patients with life-limiting conditions, 38 studies included only parents with deceased or dying children, and 3 studies examined parents and children together. Three studies examined the needs of surviving siblings, and three studies explored the perspectives of family members in general.
Parental and healthcare provider perspectives were included in two studies, and one study explored the perspectives of the pediatric patient, their parents, and their healthcare providers. Eleven studies documented only the perspectives of healthcare providers, and three studies were exclusively chart reviews. Although some studies included quantitative data, the majority used qualitative methods. Studies collected data through the examination of medical records, surveys, and individual and/or focus group interviews.
Communication Within the Family
Communication between caregivers and child
All three of the studies that examined communication between parents and children with a terminal diagnosis focused on if and how parents discussed death with their child; none of the studies included communication with the child about EOL care. Only one study included patients with diseases other than cancer. Most studies implemented a qualitative approach (see Table 1).
While research regarding how parents make decisions about discussing death is still in early stages, several studies identified the following potentially influential factors: families were more likely to discuss death if they were more religious, the child was older, and they perceived that the child was more aware of their medical condition and possible death. 21 Those who elected to discuss death with their child wanted to prepare their child for death, support their child's needs and wishes, help their child cope, and foster closeness in their relationship with their child.13,24 Those who refrained from discussing death aimed to protect their child and themselves.13,24 In reviewing parents' choice about discussing death with their child, no parents reported regrets about discussing death, whereas 27% who did not discuss death with child expressed regret. 21
Communication between caregivers and surviving siblings
To date, three studies have examined communication about EOL with a surviving sibling. Preliminary research has suggested that parents approach talking with surviving sibling about death similarly to how they approach the dying child: avoiding discussions to try to protect children or engaging in discussions to help children prepare for the death of their brother or sister. 13 One study suggested that the majority (87.5%) of parents' spoke with siblings about the child's death (from the parents' perspective). 25 The two studies which included data from surviving siblings' perspectives suggested that siblings held concerns about their brother or sister's impending death and wanted to be consistently informed and involved in their sibling's life and EOL care.19,20
Communication between the Family and the Medical Team
General EOL care communication
Twenty-eight studies suggested that parents perceive communication with the medical team as an important part of pediatric EOL care.14,16,22,26–51 Thirty-three studies focused on a facet of provider–patient/family communication regarding a difficult prognosis.22,23,27,29–32,34–37,40,42–44,46–49,51–64 Thirteen studies identified communication problems between parents and medical team such as gaps in communication among medical staff and provision of contradictory medical information to parents,28,41,44,46,48,50 use of confusing medical terminology,22,27,41 delivery of bad news in an uncaring manner,14,41,45,47 not providing enough information,29,30,47,49 and providing information too quickly.41,47
One study revealed that language can be a significant barrier to parent–provider communication, and many non-native English speakers reported that they were never informed of their right to an interpreter or that one was not available during daily care activities and important conversations with physicians. 29
Parents valued receiving information in a sensitive manner31,35,36,47,51 and expressed an appreciation for honesty about prognosis and medical plans.16,33,40,43,45,48,51 Parents also reported a desire for the medical team to show respect for the child–parent relationship and their religion and culture.32,43 Siblings are often left out of EOL discussions with the medical team,61,62 but reported a desire to be included.48,65 For example, results from one study indicated that surviving siblings felt that their distress during the dying process would have been lowered if they had received more support and consistent information about their sibling's condition from medical staff throughout the illness (rather than only when their sibling was actively dying). 65
While results consistently demonstrate that families prefer honest and timely information as described above, this may be challenging for providers who are not comfortable initiating EOL conversations. For example, one study found that the majority of physicians (53.7%) felt “somewhat uncomfortable” or “very uncomfortable” when telling their pediatric palliative patient the truth about their prognosis. 62 Another study found that 30–77% of their medical team members reported that they were “inexperienced” in communicating about pediatric EOL. 14
Specific barriers to EOL conversations included unrealistic parent expectations,66,67 different understandings of the prognosis and disagreement over the treatment plan,66–68 and a lack of parental willingness to acknowledge the child's condition or readiness to engage.66–69 Healthcare providers noted that the quality of EOL conversations are improved when there is mutual respect between the patient and their family and the medical team. 52
Communication about EOL decision making
Much (eight studies) of the pediatric EOL research on communication from a medical provider perspective focused on EOL decision making.15,56,62,66–68,70,71 Chart review studies have suggested that EOL decision-making discussions are often delayed until the patient is actively dying.69,72,73 For example, in an investigation examining adolescents with terminal cancer, 50% of initial EOL conversations began within the last 30 days of the adolescent's life. 72 Similarly, another study found that of 30 children with terminal diagnoses, 58% had do-not-resuscitate orders addressed for the first time within the last 24 hours of their life. 73 This is consistent with a study surveying clinicians regarding their opinion of patient–family involvement in EOL decision making which identified that 71% reported that advanced care planning (ACP) conversations should occur earlier than they typically took place. 67
Medical providers' approach to involving parents in EOL decision making varied on a spectrum from a more paternalistic approach to full parental autonomy. 56 Some studies showed that providers' took a collaborative approach with families with shared decision making.16,52,56,70 Others took a more paternalistic approach of making EOL decisions and informing families of their decsion.15,56,70 This latter approach may have been influenced by the severity of the child's illness (i.e., if survival was not possible, parents were less likely to be consulted in decisions). 70
Although many parents did not desire full autonomy when determining whether to limit or withdraw life-sustaining treatment, 53 research has indicated that parents may be able to manage a more active role in decision making about their child's care if they are given the opportunity.15,74 Some research has indicated that parents have a strong need to be involved in an individualized EOL decision-making process with their child's medical team,15,53,75 a factor that has been shown to decrease long-term parental grief.55,69,76 Many parents also believed that their child should be involved in the development of their own ACP in a way that was developmentally appropriate. 35 Parents reported that it was important that the medical staff affirmed EOL decisions that parents made35,54,75 and that they needed support and flexibility from the medical team when reconsidering their EOL decisions. 35
Physician hesitancy to initiate these discussions with patients and their families stemmed from an uncertain prognosis, lack of confidence in the decision, and uncertainty regarding their responsibility for the decision. 66 Medical staff sometimes lacked the knowledge and experience to feel comfortable initiating EOL decision-making discussions with the patient and their family and feared discomfort or the patient's reaction, particularly when there were little or no emotional support resources available for the patient postconversation.66,67 In one study, nurses referenced a lack of physician prioritization of family involvement as a deterrent to collaborative EOL decision making, 67 which may be encouraged by institutional norms. 66 Physicians reported additional barriers of collaboration in ACP to include impaired cognitive ability of the patient, lack of patient readiness, and patients trying to protect their parent. 66
Conclusions and Discussion
Findings from this systematic review suggest several primary conclusions as follows: (1) there is ample evidence from both families and providers that communication is very important in pediatric EOL care, (2) barriers to communication between families and providers have been consistently identified, and (3) we know very little about pediatric patients and siblings' experiences and intrafamily communication around pediatric EOL.
Furthermore, results from this review suggest that communication could be improved between (1) parents and children receiving EOL care, (2) parents and their surviving children, and (3) families and their medical team. A primary role of PPC teams is improving the communication between families and medical teams and helping to facilitate discussions within families. PPC is particularly well poised to promote communication and be of great value to both families and medical teams. Expanding our knowledge about communication gaps and developing tools to promote communication in context of EOL discussions should be of high priority to our pediatric medical community.
Parents differ in their approach to communicating with their child and surviving siblings about EOL care and anticipatory death in a number of ways (frequently avoiding the topic, although often with good intentions).13,17,18 Results from this review suggest that parents make thoughtful decisions regarding whether and how to discuss death with their child when they are given a terminal diagnosis. It is unlikely that any single solution will work across all families. However, parents may benefit from education about what kind of information to provide children and siblings during this difficult journey; medical teams may want to consider how they can support intrafamily communication.
While there are a number of very well-articulated, well-theorized models of PPC and the importance of communication within family members and between family and medical teams is recognized,9,10,16,19–21,27,32,33 many parents continue to report communication challenges with medical teams.13,22,27–29,41,44–50 In addition, pediatric patients and siblings are often left out of EOL care discussions.61,65 Healthcare providers also report barriers, including unrealistic parent expectations,66,67 different understandings of the prognosis and disagreement over the treatment plan,66–68 and a lack of parental willingness to acknowledge the child's condition or readiness to engage.66–69 Many medical professionals reported little or no preparation in how to initiate EOL discussions with pediatric patients and, consequently, felt uncomfortable including the patient and family in this decision-making process.15,63 Institutions in which providers regularly care for children at EOL may want to offer additional training to support providers in communication about EOL challenges. Given that EOL communication and ACP may be delayed for many families,57,68,73 trainings may want to include information on how to introduce ACP as part of a standard approach to care and before when the child is actively declining. Trainings may also want to integrate existing recommendations of how to facilitate family meetings and communication with parents. For example, providers may benefit from rehearsing what they are going to say and how to say it, preselecting a meeting location and those individuals who will be present (e.g., including a psychosocial provider), offering a plan for the next step, creating an atmosphere for families to ask questions, and bringing an awareness of the family's cultural background as it may relate to the understanding or reactions to a difficult prognosis.32,34 The exact content and intensity of training for optimal comfort in EOL communication is an avenue for future research. In addition to training, medical teams can consult PPC teams (where available) earlier in the child's medical path, as those families who have received PPC report improved communication. 12
Several limitations of this review should be considered. First, a few factors may limit generalizability of conclusions: many of the studies have small samples and provided qualitative data only, research included in this review was conducted across the world and some of the findings may have been influenced by cultural factors, and much of the research presented was conducted with either neonatal intensive care unit samples or pediatric cancer. In addition, as mentioned previously, only a few studies have been conducted regarding intrafamily communication, so conclusions based on the results of these studies should be interpreted with caution.
These limitations highlight avenues for future research. When examining communication between parents and medical teams, researchers may want to consider conducting larger multisite studies using either a quantitative or mixed methods approach to enhance generalizability of research findings. In addition, more research is needed to better understand how medical teams can support pediatric patients and their siblings when EOL care is necessary. Medical teams can be integral in guiding families in supporting their children through the EOL path, but more research is needed to determine the best approach for this support.
Footnotes
Acknowledgments
The authors thank Paul Miller Mazda (Lexington, KY) for their funding contribution toward this research.
Author Disclosure Statement
No competing financial interests exist.