
Abstract
Abstract
Objective:
To determine whether specific psychosocial interventions can ease discomfort in palliative care (PC) patients, particularly in those with high levels of pain or emotional distress.
Methods:
Changes in the psychological parameters of 8333 patients were assessed in a quasi-experimental, prospective, multicenter, single group pretest/post-test study. Psychosocial care was delivered by 29 psychosocial care teams (PSTs; 137 professionals). Pre- and post-intervention changes in these variables were assessed: mood, anxiety, and emotional distress. Patients were classified as complex, when presented with high levels of anxiety, mood, suffering (or perception of time as slow), and distress (or unease, or discomfort), or noncomplex. These groups were compared to assess changes in suffering-related parameters from baseline.
Results:
Psychosocial interventions reduced patients' suffering. These interventions were more effective in complex patients.
Conclusions:
After successive psychosocial interventions, the level of suffering in complex patients decreased until close to parity with noncomplex patients, suggesting that patients with major complexity could benefit most from specific psychosocial treatment. These findings support the importance of assessing and treating patients' psychosocial needs.
Background
A
Current models of treating suffering in cancer patients define distress as the expected psychological reaction of patients facing their own death. Holland et al. 5 defined distress as an unpleasant emotional experience of psychological (cognitive, behavioral, and emotional), social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, or treatment. Such is the importance of psychological aspects that distress was recognized as the sixth vital sign by the Canadian Strategy for Cancer Control (CSCC) 6 in 2005.
Psycho-oncological care for EOL patients includes interventions to alleviate suffering in accordance with the patient's personal characteristics (values, principles, personality, life history, and personal affective relations, among others) and the specific circumstances at the time of intervention (symptoms, disease progression, perception of the proximity of death, fears, etc.). Breitbart and Heller 7 proposed a therapy based on Viktor Frankl's logotherapy, 8 focused on the search for meaning. A similar approach is dignity therapy, 9 the main tenet of which is that all people should be treated with dignity until the time of death. Maté et al. 10 proposed a model of care based on meeting the essential needs of patients.
All adaptation models7–10 share the same key components: everyone is unique, and the adaptation process will necessarily be different for each person.
Jünger and Payne 11 noted that psychologists working in PC face specific challenges related to the limited time available for interventions in the context of complex needs of patients nearing EOL. Campbell et al. 12 recommended the use of evidence-based psychological treatments whenever possible. Breitbart et al.13,14 and Chochinov 15 performed clinical trials to assess the effectiveness of psychological interventions. Both authors created schools of thought about how to treat the psychological aspects of EOL patients, with a strong evidenced-based approach. 16
In Spain, thanks to La Caixa Foundation,17–19 which had spread out the psychosocial assistance to EOL patients and their family since 2008, developing a Program of Comprehensive Care for people with advanced illness. This program has showed that specific teams, which provide psychosocial and spiritual care, can improve well-being of EOL patients and caregivers. 20 In this sense, Mateo-Ortega et al., 17 who evaluated in nearly 9000 EOL patients, included in the above program a range of variables (anxiety, distress, suffering, adaptation, meaning, etc.). Results showed that all the variables improved with treatment, thus underscoring the effectiveness of psychosocial interventions in this patient group.
Objective
The main objective of this study is to determine whether specific psychosocial interventions can reduce suffering and distress in patients with advanced illness or at EOL, particularly in those with high levels of suffering or distress.
Secondary objectives
To show that interventions performed by specialized psychosocial care team (PST) can improve psychosocial symptoms, even among patients previously treated by a conventional PC team. It is important to stress that the study population had already received general psychological support from a standard PC team, as recommended by the NICE guidelines. 21 This is relevant because any improvements in the patients' psychological status after the PST intervention can be attributed to that intervention rather than to the general psychological treatment previously provided by the PC team.
Finally, the study seeks to determine if the presence of high levels of suffering and distress at initiation of the PST intervention influenced the effectiveness of interventions.
Design
Quasi-experimental, prospective multicenter design with a single pretest/post-test group to assess efficacy.
Participants
All consecutive patients treated by the PST during one natural year (July 1, 2013–June 30, 2014) were included. Inclusion criteria were as follows: (1) treatment by ≥ one of the PC teams, (2) suitability for psychosocial intervention after PC team assessment, (3) acquiescence to receive at least three PST visits, and (4) diagnosis of advanced and/or terminal illness. Exclusion criteria were as follows: (1) age (<18), (2) inability or severe difficulties to participate in the clinical interview, and (3) difficulty understanding the interview questions due to poor general condition or cognitive impairment. If cognitive impairment was suspected, a cognitive screening test such as the Pfeiffer test was administered; patients who failed it were excluded. 22
Each PST was composed of 3–4 professionals, mostly psychologists and social workers (110 psychologists, 27 social workers, and 20 professionals from other disciplines). The PST worked in close collaboration with 171 conventional PC teams (67 hospital-based and 104 home care teams). In fact, the PC teams were responsible for contacting the PST to request interventions in patients/families with psychosocial care needs.
Figure 1 shows the treatment process for patients referred to the PST. After the initial visit, the PST is responsible for patient follow-up until discharge, which occurred for: (1) patient's death, (2) improvement in psychosocial care needs, or (3) transfer to another care team or to home care.

Referral and PST process. PST, psychosocial care team.
Procedure
Data were collected by professionals of the PST through the standard clinical interview process, guided by a semistructured interview specifically created for this purpose. This gave PST members sufficient flexibility to conduct an individualized assessment and intervention while, at the same time, providing a systematic evaluation process to assure the relative standardization of the PST interventions conducted by different teams.
All PST members received intensive training prior the start of their activity to establish a specific interventional model of care provision and to guarantee a standard approach to assessment, interventions, and data registration. This consisted of a postgraduate course of 30 European Credit Transfer and Accumulation System (ECTS), with a minimum attendance of 25% and the rest consists of autonomous work of the student together with continuing education provided semiannually thereafter.18–20
The psychosocial interventions comprised specific psychological techniques aimed at addressing the issues that caused the patient the most distress. According to Astudillo et al., 23 care of EOL people must always be adapted to the unique situation and characteristics of each patient. Thompson 24 stressed the importance of taking a flexible approach to therapy in cognitive-behavioral psychotherapeutic interventions, both regarding therapeutic intensity and respecting the patient's desire to speak (or not to speak) about thoughts or feelings.
Based on Anderson et al., 25 the inherent difficulties to end-of-life situations that can determine interventions were taken into account; we prioritized flexibility and adaptability of the interventions to suit the specific needs and priorities of patients, as well as the mean length of stay in the PC ward. Although the assessment and monitoring of the variables were identical for all cases, as well as the program for the registration of data, the intervention was adapted and tailored to the needs of the patient in each visit, based on a common model of care and focusing on the patient's well-being.
The emphasis of the psychological intervention was based on the “threats-resources” model, 26 with a humanistic focus 27 designed to help the patient mobilize his/her internal resources to face the threatening situation. Care was individualized according to the needs and priorities of each patient, using diverse psychotherapeutic techniques (or the key components of these) of proven efficacy in PC, including assertive communication, counseling techniques, 21 cognitive-behavioral therapy, problem-solving techniques, narrative therapy, life review therapy, saying goodbye to loved ones, and therapies (or parts of these) based on the search for meaning,13,14 dignity,9,15 or compassion,16,28 among others. Professionals offered a psychosocial intervention, homogenous and systematic, made of specific psychological techniques, basic personal aptitudes, and an approach focused on patients' main needs. 19
The objective of psychosocial intervention4,5,7,8,10 is to reduce patients' distress to facilitate adaptation to the EOL process. This is a brief, individual person-centered psychotherapy that respects the patient's principles, values, and preferences. 10 The key aspects of this psychological intervention are shown in Figure 2.
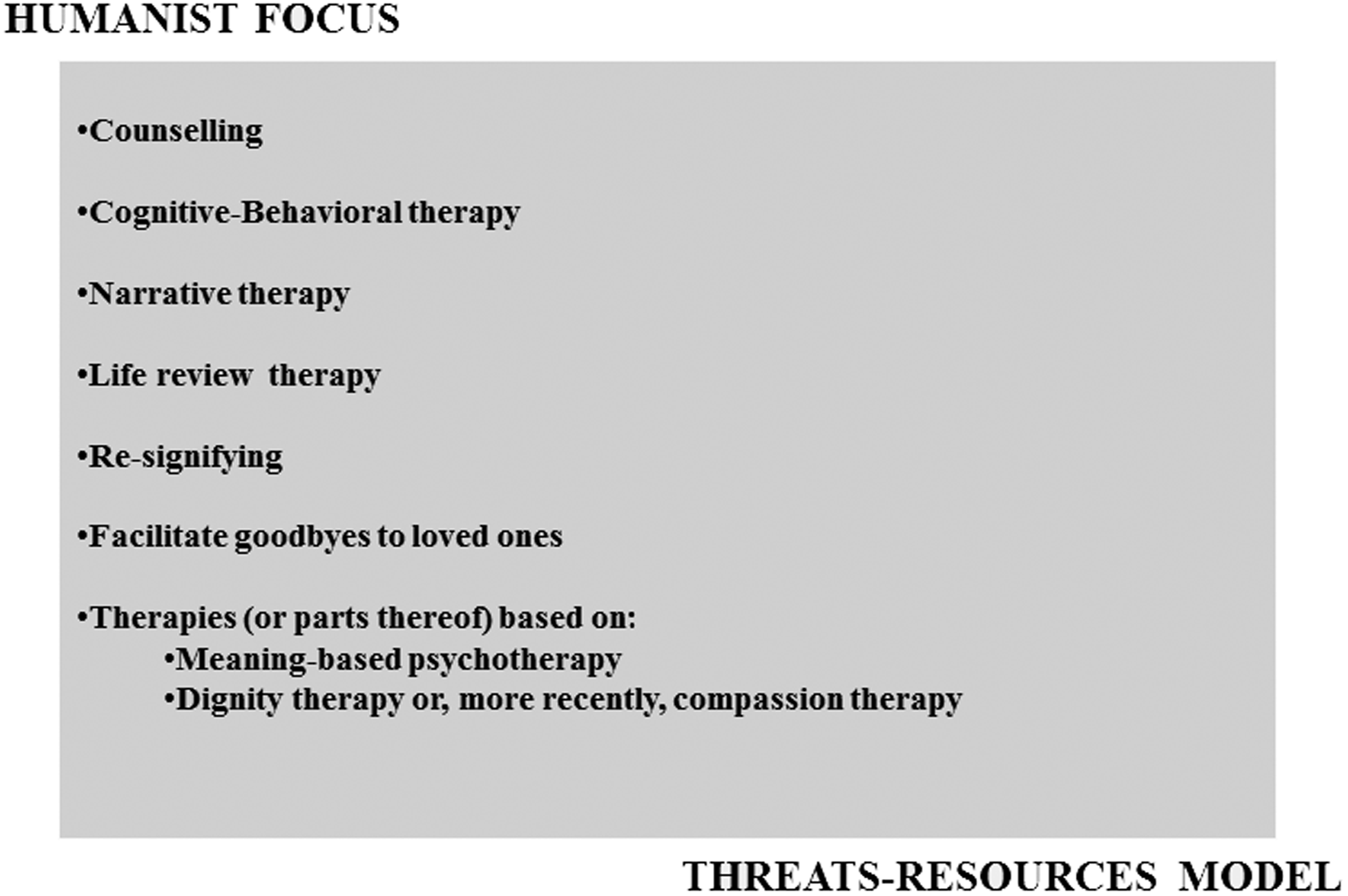
Summary of psychological interventions performed by PST.
Measurements
Materials and tools
Data used in this study were collected by members of the PST after each interview and registered in an online database. The database variables included: (1) sociodemographic data and primary illness; (2) social/family information (family composition, degree of emotional impact, overload, capacity for organization of patient care, etc.); (3) emotional data, including levels of anxiety, distress, and suffering; (4) spiritual aspects; (5) and an overall assessment by the PST professional about the patient's general adaptation to his/her situation at the time of the initial interview.
Variables
We evaluated changes from baseline in anxiety, mood, and distress. To measure clinical improvement, we measured the magnitude of change over time for all variables up to the fifth visit (baseline included).
Mood
It is a global measure of how the patient perceives his/her own mood, as proposed in the Detection of Emotional Distress (DED) Scale29,30 where the patient is asked to rate his mood on a Verbal Numerical Rating Scale (VNRS) ranging from 0 to 10 (0 is “very bad” and 10 “very good”). Overall, the DED Scale has a good sensitivity and specificity and an internal consistency (Cronbach's alpha) of 0.69.
Anxiety
According to similar studies to assess anxiety,31,32 the patient was asked to rate his/her level of anxiety on a VNRS from 0 to 10, where 0 is no anxiety and 10 is the maximum anxiety. Davey et al. 33 found that a single-question VNRS was highly correlated (Spearman's rho, 0.75) with the State Trait Anxiety Inventory (STAI) in determining anxiety levels.
Distress
Using the emotional thermometer proposed by the NCCN,5,34 we assessed an overall measure of “emotional distress” perceived by the patient with a VNRS ranging from 0 to 10, where 0 indicates no distress and 10 “maximum possible distress.” A value of 5 is considered the cutoff point for clinical distress, but higher or lower scores can be used to program the appropriate level of social or psychological intervention (Roth et al. 35 ).
Variables for sample stratification
To assess the influence of these variables on the effectiveness of interventions, we created a psychosocial complexity model. This included psychological and spiritual complexity criteria and was used to stratify the sample. This model assumed that patients with more emotional complexity at the first visit would be most likely to benefit from the PST interventions, as reported in previously described models.5,9,10,13–16,24–28,36,37
Thus, patients were considered to have high emotional complexity when presented with three or more of the following inclusion criteria at the initial visit:
Suffering or slow perception of the passage of time Anxiety ≥7 points Distress ≥7 points Mood ≥7 points Adaptation ≥7 points Patients who had spiritual beliefs and said that they thought they were not being useful in the current situation.
Patients with ≥4 variables with a missing value were considered nonevaluable. In addition, patients who had only 1 visit were excluded of the analyses, just because they had not any visit to comparison. Measures of the effectiveness of the PST interventions included changes on the rating scales for the psychological variables assessed at each visit. We evaluated the absolute and relative increase in mean scores between the initial and final visit in the complex patient group. To check for statistically significant differences, we used a multilevel regression analysis adjusted by patient age, gender, diagnosis, and the percentage of psychologists in the PST to determine overall trends for the whole sample through multiple linear regressions. Statistically significant increases (or decreases) in scores from visit to visit of each patient were indicative of treatment effectiveness. The percentage improvement on each variable compared to the mean baseline level was also calculated (beta index from baseline visit divided by the beta index in the constant model).
Ethical considerations
This study was approved in May 2011 by the Clinical Research Ethics Board of Bellvitge University Hospital, Barcelona, Spain (Ref. LACAIXAPROGMARC-2011) and adhered to the Spanish Law 15/1999 governing protection of personal data. Given its nature, written informed consent from the study participants was not considered necessary.
Results
General sample characteristics
We collected evaluations for 10,524 patients treated by 29 PSTs. We excluded from the analysis underage patients (n = 169), patients with missing data (n = 34), and patients who received only one visit (n = 1988). Consequently, the final sample consisted of 8333 patients, most of whom (75.1%) were cancer patients. The mean age was 72 (SD, 14) years, and 46.1% of the patients were women (Table 1).
In relation to spirituality variables, 78% of patients said that they had spiritual beliefs. Regarding the practice of religion, 96% were Catholic, 0.68% were Protestant, 0.68% Islam, and 0.46% Orthodox Christians and other minoritarian groups.
The median number of days elapsed between the first and last visit was 25 days. The median duration of the visits was 40 minutes for the baseline interview and 30 minutes for the follow-up visits.
Comparison of patients stratified by complexity
The sample was stratified into complex versus noncomplex patients: 5024 patients (60.3%) were considered complex, while 3309 (39.7%) were considered noncomplex patients.
Using Student's t test to compare means (t = 16.66; d.f. = 11,107; p < 0.001), we found that complex patients were younger (70; SD = 14.1) than noncomplex patients (73; SD = 14.5). Likewise, chi-squared tests showed that the complex group of patients had significantly more females than the noncomplex group (X2 = 4.7; d.f. = 1; p < 0.05) and fewer cancer patients (X2 = 15.69; d.f. = 1; p < 0.001).
The mean change per visit for the variables mood, anxiety, and distress in the noncomplex patient group appears to remain relatively stable over time. By contrast, these variables clearly improve after each visit in the complex patient group (Fig. 3).
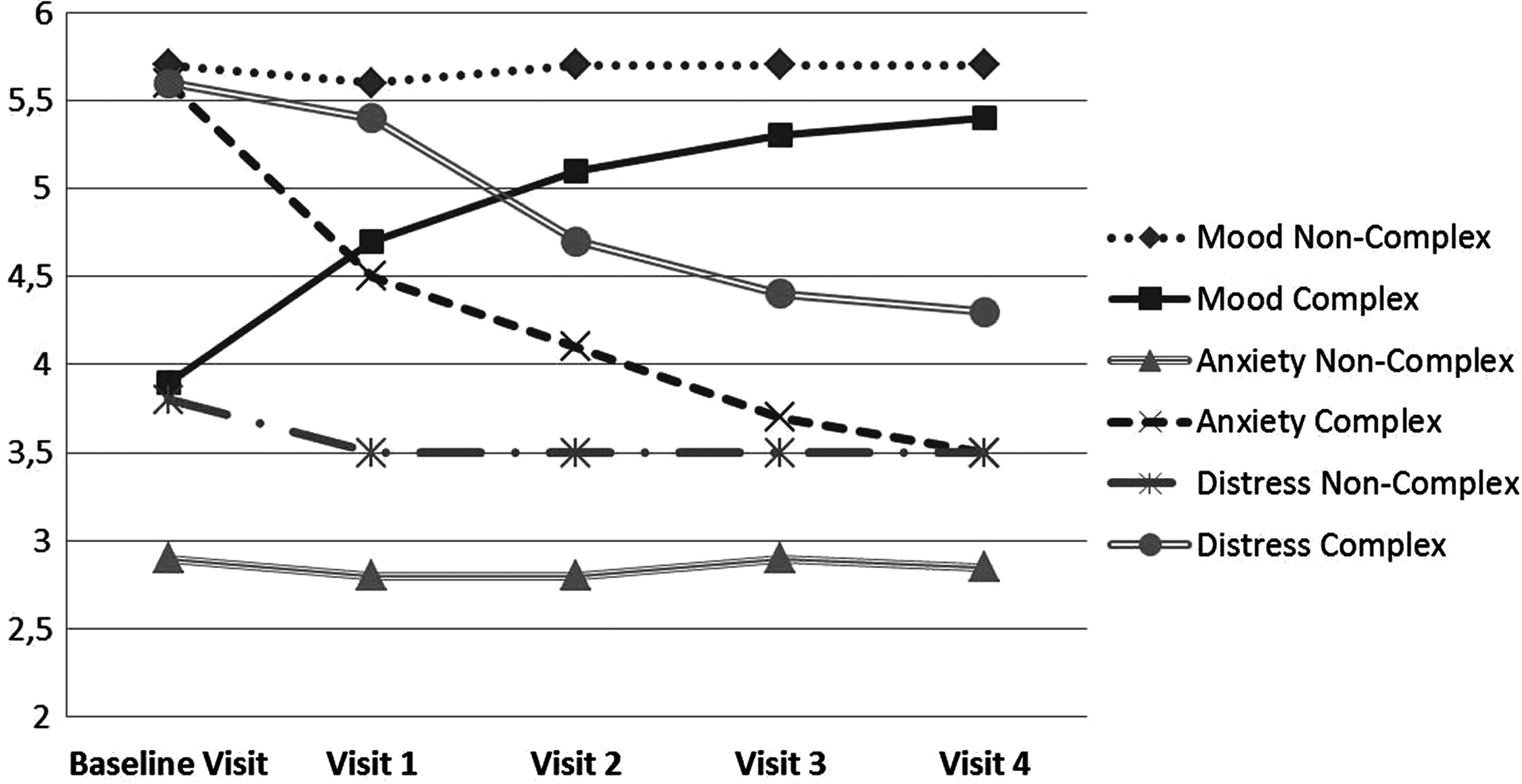
Mean mood, anxiety, and distress scores by patient complexity at each visit.
Mood
On the multilevel regression model, mood remained stable in the noncomplex patient group (Table 2), with no significant improvement per visit (β visit = 0.02; β constant = 5.78; p > 0.05). By contrast, mood improved as the number of visits increased (β visit = 0.456; p < 0.001) in the complex patient group. Compared to the mean scores at baseline (independent of age, gender, and diagnosis) each extra visit improved mood scores by a mean of 13% (β constant = 3.51; p < 0.001).
Anxiety
Based on a visual analysis, the mean change per visit in anxiety scores (Fig. 3) in the noncomplex patient group appears stable (mean baseline score, 2.9 [SD = 2.0] vs. mean score at visit 4 = 2.8 [SD = 2.1]). In the complex group (mean baseline score, 5.6 [SD = 2.3] vs. mean score at visit 4 = 3.5 [SD = 2.2]), we found an absolute improvement of 2.1 points between the first and last visits and a 38% relative decrease in anxiety (β constant = 3.77, p < 0.001).
The independent model for both complex and noncomplex patients (Table 2) showed that anxiety decreased significantly in noncomplex patients as more visits were performed (β = −0.09; p < 0.001). Compared to the mean baseline level (independent of age, gender, or diagnosis), each extra visit resulted in a mean improvement of 2.4%.
In this same model, complex patients also showed improvement as more visits were performed (β = −0.09, p < 0.001, β constant = 3.77, p < 0.001). Compared to the mean baseline level (independent of age, gender, or diagnosis), each extra visit resulted in a mean improvement of 9%.
Distress
The independent regression model (Table 2) showed that distress in the noncomplex patients decreased as age increased (β = −0.01; p < 0.001) and distress decreased as the number of visits increased (β = −0.15; p < 0.001). Compared to the mean baseline levels (independent of age, gender, or diagnosis), each extra visit resulted in a 3.7% improvement in the noncomplex patient group. In the complex patient group, women presented greater levels of distress than men. In addition, distress was lower in younger patients and decreased as the number of visits increased (β = −0.75, p < 0.001; β constant = 7.69, p < 0.001). Compared to the mean baseline level (independent of age, gender, or diagnosis), each extra PST visit resulted in a mean improvement of 9.8%.
Conclusions
This study sought to determine if specific psychosocial interventions can reduce suffering and distress in PC patients, particularly in those presenting high levels of psychosocial complexity. In addition, to determine if these same interventions, performed by specialized PST, could improve psychosocial symptoms in patients previously treated by a conventional PC team.
Our results show that patients with higher levels of suffering at the baseline visit experienced greater improvements in mood, anxiety, and distress levels. Our findings are consistent with those obtained by Breitbart and colleagues,15,16 who observed that meaning-based group psychotherapy improved patient perception of meaning in life and of well-being, thus reducing their suffering. Chochinov et al. 38 found that dignity therapy improved patients' subjective perception of depressive symptomatology.
The fact that a high percentage of patients (39%) received only one visit from the PST could be consistent with other studies that reported a dropout rate of >50% due to patient's death or poor general condition 39 and with studies that included high proportions of patients with poor prognosis. 12
The high percentage (60.3%) of patients classified as complex supports the need for specialized PC teams with expertise in psychosocial interventions, as recently recommended2,21,34 by various scientific societies.
The condition of noncomplex patients appears to remain relatively stable after the psychosocial intervention and, importantly, does not worsen over time even though the disease continues to progress. This suggests that the psychosocial intervention in patients without complexity criteria limits suffering to manageable levels in EOL situations.
Clinical implications
As it is known that suffering is usually involved in dying process, the intervention of the PST seems to contribute significantly to maintain the levels of suffering to tolerable degrees, even through the progression of the disease.
Considering the efficacy of these teams in the improvement of patients' welfare, it seems necessary to improve equity in psychosocial assessment, prioritize PST interventions on complex patients, and perhaps consider an increase in the number of professional teams so that more patients can benefit.
Study limitations
Although positive results were obtained, this study presents some limitations. The first one is related to the nonexistence of a control group to compare patients and monitor some of the possible factors affecting the situation. The second limitation is associated with not having validated and specific tools to assess psychosocial needs in our context. This has been partially solved using some of the items and dimensions of wider validated tools.
Finally another important limitation is related to data collection where data were collected by the same PST members who were delivering the intervention, rather than an independent researcher. We opted to prioritize on collecting the maximum quantity of data as possible. This potential bias in the results was always taken into consideration in the design of this study. In this sense, data were collected through the regular clinical interview performed by the professionals and registered immediately after the visit by the same professionals. Although this may suppose a potential bias, authors considered that this could be compensated by the high number of data collected and decided to prioritize on keeping the therapeutic atmosphere and the well-being of the patient.
Footnotes
Acknowledgments
The authors express their deep gratitude to the staff of the Area of Social Integration at “la Caixa” Foundation (Barcelona, Spain)—Marc Simón, Montserrat Buisan, Verónica de Pascual, Marta González, Lidia Albert, Mireia Guardiola, Eulàlia Cardeña, and Elisabet Serra—for their commitment and support in the implementation of the Program of Comprehensive Care for people with advanced illnesses and their families in Spain. The authors are also thankful for all the healthcare professionals who worked in the psychosocial teams of this program.
The authors also specifically thank the following institutions for their support in the implementation of the program: the Spanish Ministry of Health, the general management of the Catalan Institute of Oncology, and the Catalan Department of Health. The authors also thank Mr. Brad Londres for his support in translating into English, reviewing, providing final language editing, and improving this document.
Author Disclosure Statement
The authors hereby certify that they have no conflicts of interests to declare.