
Abstract
Abstract
Objective:
The aim of this study was to illustrate the characteristics of patients with palliative care (PC) needs, early identified by general practitioners (GPs), and to analyze their care process in home PC services.
Background:
Early identification and service integration are key components to providing quality palliative care (PC) services ensuring the best possible service for patients and their families. However, in Italy, PC is often provided only in the last phase of life and for oncological patients, with a fragmented service.
Methods:
Multicenter prospective observational study, lasting in total 18 months, implemented in a sample of Italian Home Palliative Care Units (HPCUs), enrolling and monitoring patients with limited life expectancy, early identified by 94 GPs. The study began on March 1, 2014 and ended on August 31, 2015.
Results:
Nine hundred thirty-seven patients, out of a total pool of 139,071, were identified by GPs as having a low life expectancy and PC needs. Of these, 556 (59.3%) were nononcological patients. The GPs sent 433 patients to the HPCUs for multidimensional assessment, and 328 (75.8%) were placed in the care of both settings (basic or specialist). For all patients included in the study, both oncological and nononcological patients, there was a high rate of death at home, around 70%.
Discussion:
This study highlights how a model based on early identification, multidimensional evaluation, and integration of services can promote adequate PC, also for noncancer patients, with a population-based approach.
Introduction
W
Integrated models are internationally recognized7,8 to ensure continuity of care between different settings (primary care, specialized home care, and hospital care) and at different stages of the disease. 9
In Italy, the development of these care models has been clearly described in Law 38/2010 and in the State Conference of 25/07/2012,10,11 but their application is still incomplete or inefficient.
In our country, the Palliative Care Local Network has the task of delivering PC through hospitals, hospices, residential nursing homes, and home care. The observational study “ARIANNA” focused on the assistance provided by Italian Home Palliative Care Units (HPCUs), which, as defined by the Italian legislation, have to ensure both basic home-care interventions, coordinated by the general practitioner (GP), and interventions of specialist teams.
Through the ARIANNA project, the primary care—PC integrated organizational model has been studied, monitoring patients throughout their care process, from early identification to eventual death, recording their path and clinical conditions throughout the study, using tools shared by the different settings.
The aim of this study was to illustrate the characteristics of patients, focusing on their early identification by GPs and analyzing the care process in home PC services.
Methods
Study design
ARIANNA a multicenter prospective observational study performed over 18 months was implemented in a sample of Italian HPCUs, enrolling and monitoring patients with limited life expectancy. The study began on March 1, 2014 and ended on August 31, 2015.
Participants
A total of 94 GPs were involved in 10, not randomly selected, HPCUs distributed throughout the Italian territory (Biella, Lecco, Brescia, Padua, Conegliano, Trento, Genoa, Gubbio, Rome, Palermo). According to the aims of the integrated model, GPs identified, among their patients, individuals who could benefit from an early palliative approach, enrolling them in the study and starting their monitoring. The time window for identification and enrollment lasted 12 months, from 1st March 2014 to 28th February 2015. There was then a further six-month follow-up period, until 31st August 2015, to further monitor patients. Figure 1 summarizes the different paths that were monitored. Patients, once identified and then included in the study (T0), could be sent from the GPs to the HPCU for a MDE, and if deemed appropriate, care could be activated (T1) in the basic home setting (T1b) or with specialist teams (T1s). For all patients, observation ended with their death or with the end of the observational study (censored patients—T2).
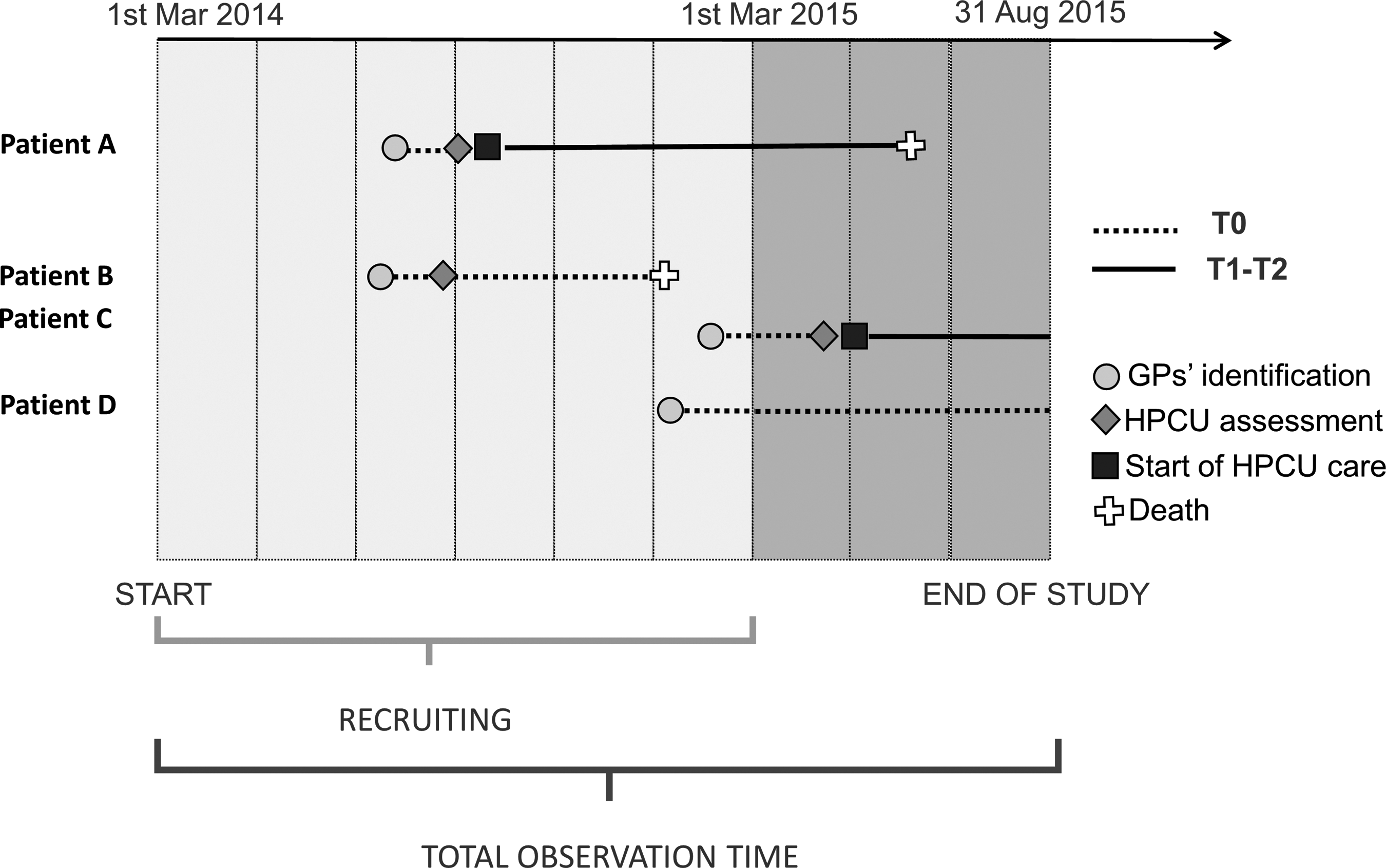
Possible paths monitored in the study.
Inclusion criteria
To enroll patients in the study, GPs used a version of the Gold Standard Framework (GSF) Prognostic Indicator Guidance (GSF) adapted for the Italian context. 12 This tool, internationally applied and validated, aims to guide GPs and other healthcare professionals in the early identification of adult patients approaching the end of life. The tool focuses on anticipating the needs of patients to ensure proper care planning. The inclusion criteria of the GSF are based on the negative answer to the Surprising Question (SQ: “Would you be surprised if the patient died in the next 12 months?”), on general criteria of decline deterioration and other specific clinical indicators, as well as on subscribing to a special form for informed consent.
General criteria included factors related to psychophysical decline and increasing needs such as a growing dependence in most activities of daily living, presence of comorbidities, reduced response to treatments, progressive weight loss (>10%) over the previous six months, and repeated unplanned/crisis admissions. Specific clinical indicators were particular subcriteria depending on the specific patient diagnosis: cancer, organ failure, renal disease, neurological disease, frailty, stroke, and dementia. 13
GPs applied GSF for every patient they assisted and the application of the GSF allowed GPs to identify, and thus include in the study, all age-related, oncological, and noncancerous patients with chronic-degenerative pathologies with limited life expectancy.
Data collection
In this study, all patient data were collected using computer-based technology.
These tools, in addition to ensuring a standardized collection of information, have allowed us to integrate services and data shared among professionals in the different settings.
GPs and HPCU professionals collected all data, and no external health records were consulted.
GPs used software designed specifically for this study, integrated within their standard clinical folders.
GPs collected all sociodemographic data, and clinical evaluation scales are described below. GPs were also responsible for collecting and entering information regarding the date and place of death.
HPCUs used multidimensional evaluation of totally web-based software interoperable with the software already present in the involved Regions and Local Health Services.
HPCU professionals collected clinical information (not shown in this work) at the time of multidimensional evaluations that they performed on patients placed in HPCU care.
Data collected by GPs and HPCUs, after being archived, were rendered anonymous before being sent for statistical analysis, in accordance with national legislation.
Evaluation scales used
For the assessment of patient status, both at time of identification and subsequent evaluations, specific internationally validated scales were used, and information recorded in the electronic medical folder. Among these, the Karnofsky Performance status (KPS) Scale 14 was applied to evaluate the patient's physical function. The index is made up of 11 categories and ranges from 100 (patient with no signs or symptoms of disease) to 0 (death).
For pain evaluation, Numeric Pain Rating Scale 15 was used, with values of 0 (no pain) to 10 (maximum pain level).
The patient's performance in day-to-day activities was evaluated through the Activities of Daily Living (ADL) scale. 16 The values of this index vary from A (maximum autonomy) to G (total dependency). There is also an H level (dependent for at least two activities but not classifiable as C, D, E, or F).
For the analysis, the scores were categorized into groups, referring to some of the experiences already reported in the literature.17,18
Statistical analyses
Qualitative variables have been described by analyzing absolute and relative frequencies, while quantitative variables have been summarized as mean or median.
Different multivariable logistic regression models have been applied to examine predictors associated with HPCU involvement and death at home.
Global survival and stratified survival were analyzed using the Kaplan–Meier method. The differences in survival rates among the different categories were evaluated with the Log-rank test. A Cox regression model was also developed to analyze the factors associated with the likelihood of death. For all analyses, a p-value <0.05 was considered indicative of statistical significance.
The only missing data were the ADL values recorded by the GPs for 39 patients who were therefore excluded from the logistics analysis and the COX regression model.
All data were analyzed using statistical software R (version 3.3.1/2016) and its analysis packages.
Ethical approval
The study was approved by AGENAS (National Agency for Regional Health Services). Patient enrollment in the study did not affect the patient's participation in care, diagnosis, and treatment pathways.
GPs requested formal written consent from all participants, and only the patients who provided such consent were included in the study after a dedicated talk with physicians.
Results
Identification
Out of a total pool of 139,071 assisted, 94 GPs identified 937 patients with a low life expectancy. The proportion of identified subjects of the total of assisted patients was thus 0.67%, rising to 3.67%, when including patients over 75 years of age only. The percentage of patients identified by different GPs ranged from 0.02% to 2%.
The GPs sent 433 patients to the HPCUs for MDE, and 328 (75.8%) were placed in the care of both settings (basic or specialist).
Table 1 summarizes some of the sociodemographic and clinical information of enrolled patients, highlighting the most relevant measures. Identified patients had a median age of 82.9 years, were mainly women (55.0%), and were more frequently affected by nononcological (59.3%) diseases. The clinical data in the table are reported based on what was recorded at the time of GP (T0) identification.
HPCU, home palliative care unit; KPS, Karnofsky Performance status; IQR, interquartile range; ADL, activities of daily living; NRS, numerical rating scale; na, not available.
Table 1 (column 2 and 3) shows sociodemographic and clinical differences comparing patients under HPCU care and those who did not receive it.
Cancer patients had a significantly greater chance of being seriously affected by their illness than patients with a major nononcological diagnosis (56.4% vs. 43.6%, p < 0.001).
Among the scales used, the main difference was observed in KPS values (p < 0.001).
Patients with a KPS <40 had a significantly greater chance of being affected than patients with a minor clinical condition (KPS 0–40: 58.8% vs. 49.8% of patients not taking p < 0.001).
As reported in Table 2, in the logistic analysis, after adjusting for sex, age, primary diagnosis, and scales values recorded at the time of identification, a primary cancer diagnosis significantly increased the likelihood of being taken into the care of a HPCU (odds ratio [OR] = 3.89; 95% confidence interval [CI] = 2.79–5.47). Higher values of KPS decreased the probability of major effects from the illness (OR = 0.50; 95% CI = 0.34–0.71).
OR, odds ratio; CI, confidence interval.
Survival analysis
There were 517 deaths among 937 identified patients with a median survival time of 293 days (95% CI = 245–359). As illustrated in Figure 2, stratifying the survival time for the type of diagnosis (cancer vs. noncancer) and for the possible takeover by the HPCUs (Taking charge/Not taking charge), there is a statistically significant difference between the oncological patients and the other three groups (Log-rank Test <0.001). In particular, in patients with a primary cancer diagnosis, a higher mortality was observed. By stratifying the analysis only for the primary diagnosis, in cancer patients median survival is significantly lower than in nononcological patients (144 days for cancer patients vs. 524 days in noncancer patients, Log-rank Test <0.001). This finding was also confirmed in the Cox regression analysis, shown in Table 3. After adjustment for age, sex, primary diagnosis, HPCU care, and values from scale evaluation, it is evident that patients with a primary cancer diagnosis have a significantly greater chance of dying than patients with other diagnoses (hazard ratio [HR] = 2.34, 95% CI = 1.92–2.86). Despite this fact receiving HPCU care is positively associated with death (HR = 1.62, 95% CI = 1.34–1.95).

Survival rate estimated through the Kaplan–Meier, stratified by primary diagnosis and HPCU care. HPCU, home palliative care unit.
HR, hazard ratio.
Place of death
Considering all the subjects included in the study, the most frequent place of death was home (70.3%). In Table 4, it is also possible to observe the difference between patients in HPCU care and those who were not. Distribution of place of death is similar but with a large difference in the percentage of patients dying in the hospital (1.2% of those in HPCU care vs. 23.3% not in HPCU care).
NA, not available.
The data are also confirmed by the logistic analysis shown in Table 4. By adjusting for age, sex, diagnosis, and values recorded by the different scales, it is noted that referral to an HPCU is a predictor associated with the likelihood of dying at home (OR = 2.07; 95% CI 1.35–3.21), while primary diagnosis does not seem to have a significant influence.
Discussion
For the first time in Italy, a prospective study was used to evaluate an integrated model of home-based PC, based on early identification with a multidimensional evaluation. The goal was to promote the integration of PC services, as is now increasingly desirable. 19 Regarding early identification of patients with limited life expectancy and PC needs, GPs were able to identify 0.67% of the total of their patients. In Italy, the mortality rate for nonpediatric subjects is about 1%, excluding deaths resulting from unpredictable and traumatic events. The rate of identification is thus in line with what could be expected. These data are lower than in other reported studies, 1 which have identified a prevalence rate of people with PC needs of 1.5% of patients. This difference could, at least in part, be attributable to a less sensitive approach to enrollment by the Italian GPs. Of 937 identified with GSF with PC needs and limited life expectancy, 556 identified subjects died during the observation period, with a positive predictive value (PPV) of 55.2%.
This value is identical to that recorded by Gómez-Batiste et al. 20 in a recent cohort study, where the prognostic capacity of an early identification tool based on the SQ was assessed. It is important to emphasize that the PPV, according to Gómez-Batiste, is much higher in cancer patients (69.5% in oncologic vs. 45.4% in noncancerous). This seems to suggest that a diagnosis of cancer, as a good predictor of death, lends itself to accurate and appropriate early identification. However, more studies could be necessary to find tools that could increase early identification especially for nononcological pathologies. As is well known, 21 cancer is one of the major determinants of access to PC services and it has been observed that these patients make up ∼75% of all patients in PC pathways. 22 There are currently many barriers to extending PC to noncancer patients, because of both the unpredictable trajectory of their illness and the difficulty in identifying a terminal stage. 23 Our instrument was able to identify and enroll well over 59% of patients with a nononcological diagnosis. However, these, as described above, had a much lower take-up and death rate than cancer patients.
As already noted in the literature,24,25 many barriers in accessing PC are at the level of primary care offered by GPs, including the reluctance of some doctors to provide PC, lack of skills and knowledge, poor coordination between operators, and confusion over roles and responsibilities. Our study highlights the rather uneven identification percentages, probably also as a result of the above mentioned problems. Very low and surprising recruitment rates among primary care doctors are also found in other countries where the identification and recruitment practices of the Healthcare System are now well established. In this respect, it is interesting to note a study conducted in Scottish primary care 26 that reports the results of applying an identification algorithm to doctors' databases using read codes (codes used by NHS-UK since 1985, identifiers of diseases, social status, and problems). This simple process allowed the average of those enrolled to be doubled (from 0.24% to 0.5%) 25 and highlighted how coordinating activities between GPs and specialist care services are theoretically well defined in the policy, but are not adequately defined and implemented in practice. The model we tested has been shown to favor the work of GPs by placing them in direct communication with HPCUs in their territory, including through a shared data exchange system, which allowed GPs to send the most critical and complex patients (433 out of 937 total) to HPCUs allowing 0.23% of patients to be enrolled, a number higher than that recorded by the classical Italian model.
Comparing the mortality-related factors with those associated with HPCU care, it can be noted that GPs are primarily guided by a major cancer diagnosis and they are not driven by high levels of pain and poor ADL. From our data, taking into account these latter two aspects, it would be very helpful to encourage GPs to signal patients, without cancer diagnosis, who could benefit from HPCU care.
Both for patients under care of HPCUs and those followed by a GP alone, there was a high rate of death at home, around 70%, compared to the other Italian areas, where only 30% died at their home. As noted by Gomes et al. 27 receiving home PC doubles the likelihood of dying at home. This percentage is close to that observed in England, in an integrated system with availability of 24 hour care and where 77% of patients died at their home while in the control group only 35% died in their home. 28 Recently, a retrospective analysis of the deaths recorded at an Italian Local Health Unit recorded that only 40.9% of all deceased patients in that province died at their home, regardless of the type of service received at the end of their life. 29 The data we collected show, therefore, how the implemented model can assure death at home to the vast majority of the identified, both of those enrolled by the HPCUs and not.
Strengths and limits
This study has some limitations. First, the 10 HPCUs enrolled in the study did not have an organizational structure that was already oriented toward service integration, and in some of them the interaction between GP and HPCU was not very effective. In contrast, this captures the current situation of the country and the state of implementation of the normative standards. The main strength of this study is to have observed an operating model whose distinctive features, as intended by Italian legislation but rarely implemented in such a systematic manner, are as follows: early identification, multidimensional evaluation, integration of services, and use of information and communication technology (ICT) tools. The study also demonstrated the validity of the identification tool for oncological patients, while for nononcological patients it requires some insights and specifications to increase its utility. A further strength lies in the design of the study. As a prospective observational study, it was possible to follow all the subjects enrolled over time, overcoming the intrinsic limits of traditional cross-sectional information collection from the GP registers.
As has recently emerged in other retrospective analyses in Italy, 30 the data from this observational study suggest that the application of early identification tools and a formalized and integrated relationship between GPs and HPCUs can lead to improved PC. In the future, it would be necessary to strengthen these data, looking not only at home environment but also at all the settings in the Local Palliative Care Network.
Footnotes
Acknowledgments
This study was supported by Fondazione G. Berlucchi Onlus (Brescia, Italy) and AGENAS (National Agency for Regional Health Services). The authors are also grateful to Fondazione Floriani for the support in the publication process. Finally, the authors thank Dr. Samantha Austen for language revision of the article.
Author Disclosure Statement
No competing financial interests exist.