
Abstract
Abstract
Background:
Globally, an estimated eight million children could benefit from palliative care each year. Effective communication about children with life-limiting conditions is well recognized as a critical component of high-quality pediatric palliative care.
Objective:
To synthesize existing qualitative research exploring healthcare users' experiences of communicating with healthcare professionals about children with life-limiting conditions.
Design:
The results of a systematic literature search were screened independently by two reviewers. Raw data and analytic claims were extracted from included studies and were synthesized using thematic analysis methods for systematic reviews.
Data Sources:
MEDLINE, PubMed, CINAHL, Embase, PsycINFO, Scopus, Web of Science, ProQuest, and ScienceDirect were searched for articles published in English between 1990 and May 2017.
Results:
This review included 29 studies conducted across 11 countries and involving at least 979 healthcare users (adults [n = 914], patients [n = 25], and siblings [n = 40]). The four domains of communication experience identified through thematic synthesis are: Information, Emotion, Collaboration, and Relationship. Although included studies were from a range of settings and diverse populations, further research is needed to explore whether and how domains of communication experience differ across settings and populations. In particular, further research about children's palliative care experiences is needed.
Conclusions:
Healthcare users typically value communication with healthcare professionals: that (1) is open and honest, (2) acknowledges emotion, (3) actively involves healthcare users, and (4) occurs within established and trusting relationships.
Introduction
R
Provision of specialized care to children with life-limiting conditions requires recognition that their circumstances can be radically different to those of adults with life-limiting conditions.1,9,13,14 Children are more likely to have nonmalignant conditions that follow uncertain illness trajectories.2,7,16 Their physiological resilience against these conditions and in response to treatment can contribute to this uncertainty.1,4,9,13 Children also have a different dynamic of care, as parents or guardians typically have ultimate legal responsibility for decision making.1,10,16,21–23 Moreover, children's ongoing physical, emotional, social, cognitive, and spiritual developments mean that their circumstances are constantly evolving.1,2,9,13,14 Such differences are likely to influence the specific dynamics of communicating with these children and their families. 13
This study sought to enhance understanding of effective communication about children with life-limiting conditions by systematically reviewing research, exploring healthcare users' experiences of communicating with healthcare professionals. Recognizing that pediatric palliative care can differ across countries3,24 and cultural contexts,3,10,25,26 this study aimed to explore similarities and differences by considering studies conducted across a range of nations. Although recent reviews consider healthcare users' experiences when a child has a life-limiting condition,17–19,26–29 none specifically focused on communication experiences. This review was therefore designed to synthesize high-quality evidence relating to a crucial aspect of care.
Materials and Methods
This systematic review focused on qualitative studies. This focus reflects a recognized strength of qualitative research for exploring and understanding human experiences such as communication. 30 Although a protocol for this review was published in 2015, 31 the review method is reported here to provide details that are relevant for the results that are reported below.
Selection criteria
This review aimed to identify and synthesize descriptive or interpretive qualitative studies investigating healthcare users' (hereafter referred to as “users”) experiences of communication with healthcare professionals (hereafter “professionals”) about children with life-limiting conditions. A communication experience was broadly defined as a report of an actual experience of spoken or written communication.
An inclusive definition of a user was adopted, encompassing children and youth with life-limiting conditions, their parents, other family members, and legal guardians. In recognition of different definitions of youth, 32 any study that reported a focus on a pediatric population was included. Studies were included if the authors reported a focus on children with life-limiting conditions. Sources with a focus that was broader than children with life-limiting conditions were included, so long as it was possible to exhaustively identify which primary data and associated analysis related to children with life-limiting conditions. Although there were no restrictions on study location, only studies published in English since 1990 were included. In addition to research articles, the review also included other types of scholarly reports such as theses, dissertations, and monographs.
Literature search and screening
The comprehensive search strategy developed for this review is reported in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/jpm). Customized searches were conducted in MEDLINE, PubMed, CINAHL, Embase, PsycINFO, Scopus, Web of Science, ProQuest, and ScienceDirect. An initial search was completed in April 2016 and updated on May 16, 2017.
Two reviewers (S.E. and N.B.) independently screened search results, first by title and then by abstract, to identify sources that potentially met inclusion criteria. Divergences in opinion were resolved by the reviewers on a case-by-case basis. One reviewer (S.E.) screened all sources determined to meet inclusion criteria through the abstract screening phase by reading the entire document. Where there was uncertainty about inclusion, the entire document was checked by another reviewer (N.B.).
Sources were excluded if they did not report studies that focused predominantly on experiences following the diagnosis of a life-limiting condition. For example, three sources studied recordings of actual conversations involving users and professionals,33–35 but did not specifically consider users' experiences of those conversations. The screening process identified studies exploring communication during end-of-life care that were not restricted to life-limiting conditions. The inclusion criteria were revised to encompass these studies.
Each included source was used to identify additional sources that may not have been identified through the search strategy. First, Scopus was used to identify sources citing the included sources. This citation search was initially conducted in July 2016, and then updated on May 16, 2017. Second, one reviewer (S.E.) screened the reference lists of all included sources. Any titles that potentially met inclusion criteria were screened using the process described above.
Critical appraisal
Each included source was appraised using the Consolidated Criteria for Reporting Qualitative Health Research (COREQ). 36 Two reviewers (S.E. and N.B.) assessed each source independently. Divergences in assessment were resolved on a case-by-case basis.
Data extraction and appraisal
All data and analytic comments that met the inclusion criteria for this review were extracted by a reviewer (S.E.). In this review, data were direct quotes from participants, and analytic comments were any text by the authors that explicitly used data to make some claim about their stated phenomenon of interest. Extracted material excluded data and analysis that focused on users' recommendations about communication rather than their actual communication experiences. Two reviewers (S.E. and N.B.) independently appraised each extracted analytic claim against the primary data reported to support that claim. Where an analytic claim was appraised to be clearly grounded in reported data, this was classified as being based on a sufficient level of reported evidence. Where an analytic claim was judged to be ambiguously grounded in reported data, this was classified as being based on an unclear level of reported evidence. Where an analytic claim was appraised to be inadequately grounded in reported data, this was classified as being based on an insufficient level of reported data. Divergences between the reviewers were resolved on a case-by-case basis.
All claims, along with their classifications, were incorporated into the synthesis stage of the review. This inclusive approach incorporated analytic claims that were judged to be based on an insufficient level of reported evidence. This enabled synthesis of the full range of analytic findings reported in the included studies, while appraising the level of reported evidence for each finding.
Data synthesis
The findings of included studies were synthesized using thematic analysis methods for systematic reviews. 37 This approach was used because thematic analysis methods were most closely aligned with the methods used in the majority of included studies. The qualitative analysis software NVivo was used to facilitate analysis. Two reviewers (S.E. and N.B.) independently coded data in NVivo to inductively identify different types of communication experiences. Following independent coding, these two reviewers compared their analysis and discussed divergences. This process was followed by further rounds of coding and comparison. This initially identified themes that encompassed similar types of communication experiences and subsequently organized identified themes according to higher order themes. Other study investigators contributed to the analysis of coded data throughout this process.
Results
Literature search and screening
The search strategy identified 1317 unique sources. As broad search strategy was adopted for this review, a large number of results did not meet inclusion criteria. Common reasons included the following: not clearly focused on children with life-limiting conditions, reporting data from healthcare professionals rather than healthcare users, not focusing on communication, and focusing on recommendations rather than actual experiences. Following screening, 36 sources were deemed to meet inclusion criteria (Fig. 1).
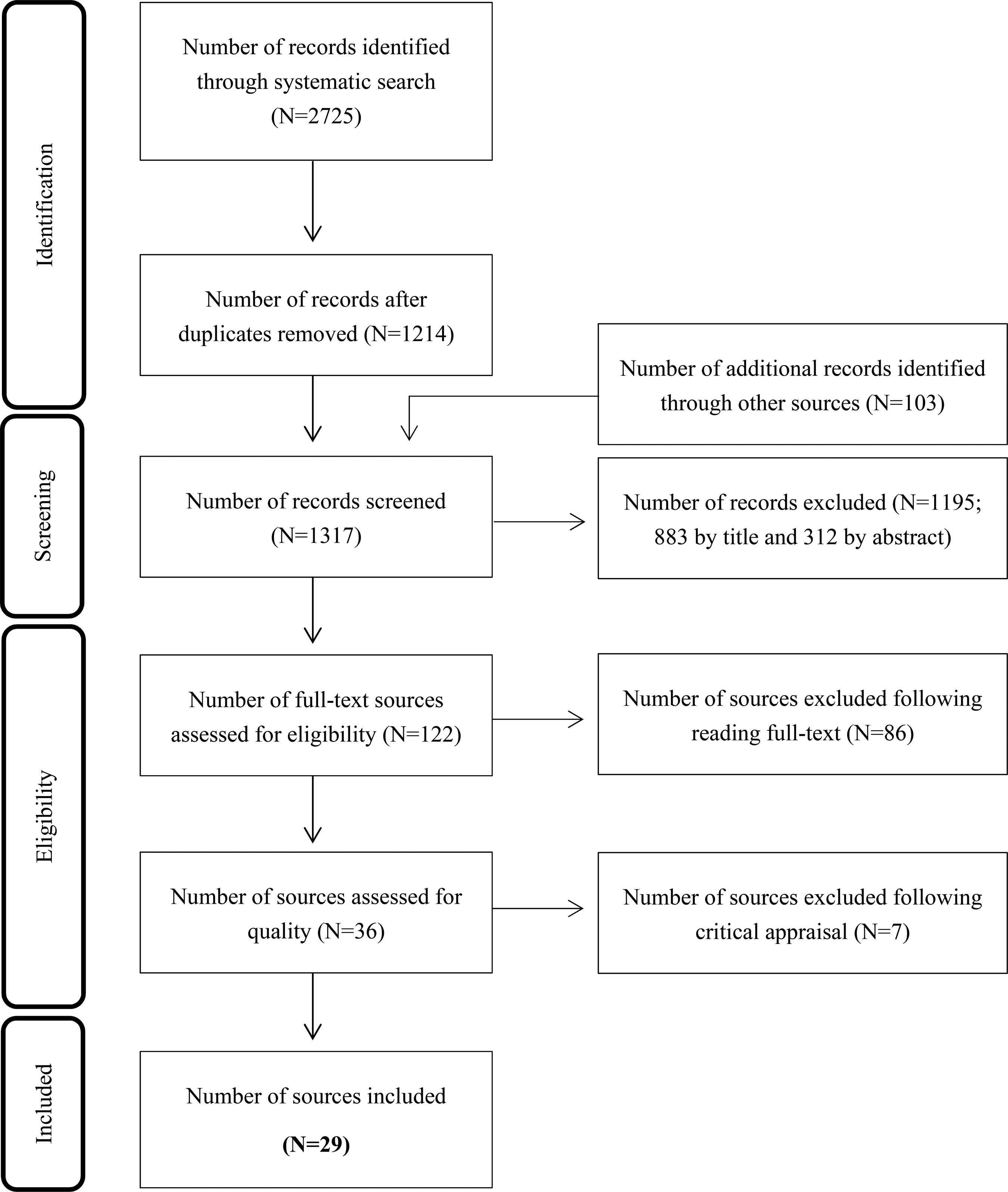
Screening results.
Critical appraisal
Critical appraisal, using the COREQ checklist described above, identified seven sources that did not report information deemed essential for inclusion in this systematic review. Six sources8,38–42 did not name or describe the analytic methods used in sufficient detail that is necessary to meaningfully compare and synthesize their findings with other sources. 43 One source 44 was excluded because the reported results were not explicitly connected to the analysis of data, which is incongruent with thematic synthesis. 37 Exclusion of these 7 sources resulted in 29 sources being included in the review. Details of these studies are reported in Table 1 and Supplementary Table S2.
Characteristics of included studies
Studies were conducted across 11 countries, the majority in the United States of America (hereafter “US”). It was not possible to determine the precise number of participants across the included studies. One source reported the number of participating families, but not the number of individual participants. 59 Two sources appear to report data obtained from the same sample, although slight differences in overall numbers of participants made this difficult to determine.53,58 Nevertheless, the sources reported studies including at least 979 participants.
Every source included adults (n = 914 participants), but only two involved patients (n = 25 participants)55,60 and two involved siblings (n = 40 participants).64,71 Six sources focused exclusively on children diagnosed with cancer;57,59,63–65,73 the remainder focused on children diagnosed with a range of conditions or did not report this information. Most sources focused on children of a variety of ages; five focused specifically on neonates.45,47,49,50,69
The majority of sources reported studies that collected data through semistructured interviews. Twenty-one sources reported studies where data were collected following a child's death. Three reported studies where data were collected during treatment.52,55,61 The remaining five sources reported studies where data were collected from both groups.45,56,60,67,71 Just under half of included studies reported using some form of Content Analysis. Other approaches reported in one or more studies included Grounded Theory, Thematic Analysis, and Discourse Analysis. Further details are reported in Supplementary Table S2.
Data appraisal
All primary data and analytic claims that met the inclusion criteria for this review were extracted. Each extracted analytic claim was critically appraised against the primary data provided to support for that claim. This critical appraisal identified that 59.3% of claims were based on a sufficient level of reported evidence, 8.6% on an unclear level of evidence, and 32.1% on an insufficient level of evidence. Although all analytic claims were included in the synthesis, they were color-coded according to their level of supporting evidence to ensure that this information could inform the synthesis phase.
Data synthesis
The findings of the included studies were synthesized across multiple rounds of coding, with consensus achieved following three rounds.
The first round of coding was undertaken independently by two reviewers, who generated a total of 91 codes. Comparison of these codes found that the reviewers had often organized data into a code that they had independently given a similar descriptive label. The reviewers' discussion of the first round of coding also identified ways that codes could be interpreted and organized into six themes. In the second round of coding, the reviewers independently analyzed data into codes that were organized by the identified themes. Following a review of this coding, three of the six themes were combined into a single, more general theme. This produced an interpretation of the data according to four higher order themes. A third round of coding confirmed the suitability of analyzing the data into these four themes.
Analysis of the four higher order themes identified across multiple rounds of coding indicated that each corresponded with a different domain of communication experience: information, emotion, collaboration, and relationships. As more than a year had passed between the initial literature search and completion of the data synthesis, an updated search was conducted to include recently published sources in the review. Two additional sources were identified.45,67 The data and analysis reported in these sources were congruent with the synthesis that was generated using the sources identified through the initial search.
Analysis of each theme identified a sufficient level of reported evidence supporting of each domain of communication experience reported by adult users, but not necessarily patient or sibling users. Given the predominance of adult perspectives within the included sources, the below synthesis primarily focuses on adult perspectives. Across the four domains of communication experience, users often provided accounts that went beyond describing their communication experiences with professionals to also positively or negatively evaluate these experiences. Close analysis identified trends, in which particular types of communication experiences were consistently, although not necessarily uniformly, described as positive or negative.
Domain 1: Information
This was the most pervasive domain, with primary evidence identified in studies from all 11 countries represented in this review. Twenty-four of the 29 studies incorporated content relating to information experiences that users tended to evaluate positively, while 23 studies incorporated content relating to experiences that users tended to evaluate negatively. Both positively and negatively evaluated experiences were reported by patient and adult users, but a sufficient level of reported evidence could not be identified for siblings. Illustrative quotes of users' experiences are reported in Table 2.
Across the studies, users consistently reported the importance of open and honest discussions with professionals (e.g., the quotes in Table 2 labeled with identifiers 1–3). Positively evaluated experiences tended to involve professionals providing detailed and yet understandable explanations, explanations of different treatment options, and checking to ensure that users understood the information that had been conveyed.
Some users described situations where professionals provided the same information more than once. Usually, this was reported as a positive experience because users were not always able to understand all information when they first received it (e.g., Table 2, Quote 4). However, there was one reported experience of repeating information that was regarded as unhelpful. This user did not consider it necessary to constantly refer to the poor prognosis of her son's condition (Table 2, Quote 5).
The most common negatively evaluated experience across the studies in relationship to the information domain involved circumstances where users reported receiving an inadequate level of information (e.g., Table 2, Quotes 6 and 7). This could range from receiving no information to receiving insufficient or unclear information. Some users reported perceiving that professionals were intentionally withholding information.
In some studies, users described difficulties in understanding information. The most common reported reason was feeling overwhelmed by the amounts of information provided (e.g., Table 2, Quote 8). This may account for the generally positively reported experience of being provided information more than once. A less frequently reported difficulty in understanding information involved circumstances where users believed that hope influenced their interpretation of the information (e.g., Table 2, Quote 9).
Domain 2: Emotion
Primary evidence of an emotion domain of communication experience was identified across 8 out of the 11 countries represented in this review; the exceptions were Iran, 45 Norway, 52 and Switzerland. 56 Eleven of the 29 studies incorporated content relating to this domain that users tended to evaluate positively, while 22 studies incorporated content relating to experiences that users tended to evaluate negatively. Both types of experiences were reported by adult users, but a sufficient level of reported evidence could not be identified for patients or siblings. Illustrative quotes are reported in Table 3.
Across the studies incorporating content related to this domain, users positively evaluated their experiences of professionals communicating with compassion and sensitivity to families' needs while also displaying a level of emotion that users reported was appropriate for the situation (e.g., Table 3, Quotes 10 and 11). Although experiences that tended to be evaluated as positive were reported across 11 studies, it was not possible to identify across these studies specific practices that professionals used to orient to emotion.
Although there was not a great amount of specific detail about positively evaluated experiences of the emotional domain, there was more detail relating to experiences that tended to be evaluated negatively. Many studies incorporated users' descriptions of professionals who delivered information as though it were routine, and was therefore insensitive to the emotional impact that this could have on families (e.g., Table 3, Quotes 12–14). This sometimes included a lack of compassion in the moments surrounding a child's death. For example, some users reported professionals who engaged in trivial or even cheerful conversations with one another in close proximity to families at a time when they were confronted with highly distressing experiences. Others reported what they regarded to be the poor timing of requests for autopsy or organ donation.
Domain 3: Collaboration
Primary evidence of a collaboration domain of communication experience was identified across 9 out of the 11 countries represented in this review; the exceptions were Iran 45 and Slovakia. 73 Sixteen of the 29 studies incorporated content relating to experiences that users tended to evaluate positively, while 15 studies incorporated content relating to experiences that users tended to evaluate negatively. Both positively and negatively evaluated experiences were reported by adult users. In contrast, a sufficient level of reported evidence of patients' experiences could only be identified in relationship to positively evaluated experiences of collaboration, and a sufficient level of reported evidence of siblings' experiences could only be identified in relationship to negatively evaluated experiences. Illustrative quotes are reported in Table 4.
Across the studies incorporating content relating to the collaboration domain, being actively involved in discussions and decision making was as a positively evaluated experience for most users in most situations (e.g., Table 4, Quotes 15 and 16). There were, however, instances where users reported being overwhelmed by an expectation that they would actively contribute to a decision (e.g., Table 4, Quote 17).
Although the majority of users positively evaluated being involved in the decision-making process, there were differences in the extent to which users wanted to influence a final decision. Most users in most situations preferred a greater level of involvement (e.g., Table 4, Quote 18), although some users in some situations expressed a preference for a relatively lower level of involvement (e.g., Table 4, Quote 19). Among those users reporting a responsibility for making decisions, there were consistent reports of positive experiences when professionals explicitly supported their decisions (e.g., Table 4, Quote 18).
In contrast to positively evaluated experiences of collaboration, some users identified negative experiences where they felt left out of discussions and decision making. On some occasions, users reported that professionals could miss important information by not engaging with a family's knowledge about their child (e.g., Table 4, Quote 20).
Domain 4: Relationship
Primary evidence of the relationship domain of communication experience was identified across 9 out of the 11 countries represented in this review; the exceptions were Iran 45 and Slovakia. 73 Sixteen of the 29 studies incorporated content that related to experiences that users tended to evaluate positively, while 15 studies incorporated content relating to experiences that users tended to evaluate negatively. Both positively and negatively evaluated experiences were reported by adult users. In contrast, sufficient reported evidence of patients' experiences could only be identified in relationship to positively evaluated experiences of relationships, and no sufficient evidence could be identified for reports of positively or negatively evaluated experiences by siblings. Illustrative quotes are reported in Table 5.
In many of the studies incorporating content relating to this domain, developing and maintaining trust and ongoing relationships with professionals were described by users as enhancing communication (e.g., Table 5, Quotes 21 and 22). They reported how this provided them with a sense of reassurance that professionals understood their circumstances and took this into account when communicating with them.
In addition to positively evaluated experiences of the impact of relationships on communication, some users identified negative experiences. One circumstance that was identified as difficult was when recommendations were provided by professionals who had little or no acquaintance with a user (e.g., Table 5, Quote 23). Without time to establish a relationship, users reported difficulties trusting a professional's recommendation. Inconsistent information provided by different professionals was also reported as difficult (e.g., Table 5, Quote 24). In both circumstances, the relationship domain appears to influence another domain of communication experience (in these cases, the information domain). However, although inconsistent information was negatively evaluated by some users, others identified benefits of obtaining different opinions (e.g., Table 5, Quote, 25).
Discussion
Communication is the most commonly used procedure within healthcare, 10 and effective communication is well-recognized as critical for ensuring the best quality care of children with life-limiting conditions and their families.1,3,6–14 The results of this systematic review indicate that it is common for this group of users to positively evaluate communication with professionals that (1) is open and honest, (2) acknowledges emotion, (3) actively involves healthcare users, and (4) occurs within established and trusting relationships. Conversely, when user-professional communication did not exhibit these features, it was common for users to evaluate this negatively.
This review highlights that users do not usually report their communication experiences with professionals in a neutral manner. Rather, users routinely evaluate their experiences. 53 Moreover, negatively evaluated experiences are often highly salient for users and can play a strong role in their overall evaluation of the healthcare that they have received.19,51,53,55 The clear identification of both positive and negative experiences within each domain of communication experience highlights how users' experiences appear to be shaped by the conduct of professionals. The four domains identified through this review, therefore appear to be crucial components of communication underpinning the successful care of children with life-limiting conditions and their families.
Recent reviews exploring users' experiences of professionals' conduct when caring for children with life-limiting conditions identified comparable domains to the four identified through the current review.17–19,26–29 Although each of these reviews did not necessarily identify all four of these domains, this is likely attributable to their differing foci to the current review. Through use of thematic synthesis and by focusing specifically on communication experiences, the current study extends the findings of these reviews by highlighting robust evidence in support of four domains of communication experience that are important for users when accessing healthcare for a child with a life-limiting condition.
This review has identified evidence that four domains of communication experience are identifiable across nations comprised different languages and cultures. This includes countries, such as Brazil 70 and France, 49 cultures in which the authors of these studies report different communication dynamics than countries such as the US. This review also incorporated several studies that specifically considered communication experiences of users whose predominant language was different from the predominant language used within the services they accessed.48,51,65 One of these studies, which directly compared experiences of English- and Spanish-speaking users in the US, did not find experiences of poor communication to be more common among Spanish-speaking users. 65 These findings warrant further investigation.
Many domains identified through this review also have been identified in general reviews of user-professional communication,74–77 including adult palliative care. 78 A major difference in this review is an emphasis on the value of established long-term relationships between users and professionals. Although previous reviews highlight the importance of relational aspects such as trust, they do not identify the same emphasis being placed on communicating within long-term relationships.
The importance of long-term relationships may be associated with, at least, in part, the uncertain illness trajectories that characterize many of the life-limiting conditions children suffer from,2,7,16 along with their physiological resilience against these conditions and in response to treatment.1,4,9 Because of this, many of these children and their families will be long-term users of specialist healthcare, and therefore have opportunities to develop and value long-term relationships with particular professionals. The principles of family-centered care that underpin pediatrics in general and pediatric palliative care in particular, 79 specifically an emphasis on high-quality communication, may also contribute to this finding.
There may be connections between the domains that were not identified through this review. For instance, close analysis during the synthesis phase gave an impression that the relationship domain was influenced by some, if not all, of the other domains and that, in turn, the relationship domain influenced some of these domains. For example, users were more likely to accept information from professionals that they had been trusting and had long-term relationships with. Although this interpretation of mutual influence between the relationship and other domains of communication experience is consistent with analysis reported in some of the studies included in this review,55,60 further research is needed to determine the robustness of this finding.
Limitations
A number of limitations should be taken into consideration when interpreting the findings of this review.
First, the majority of studies focused on adult family members, so the findings of this review should be applied to patients and their siblings with caution.
Second, although the included studies were conducted across 11 different countries, the majority of studies were conducted either in the US or another predominantly English-speaking country. There were no studies conducted in Africa or Eastern Asia, and only one in South America. 70 Moreover, the review was limited to studies reported in English. For these reasons, the findings of this review may not necessarily translate to different cultural and linguistic settings.
Third, only a few of the studies explicitly compared communication experiences relating to children of different ages48,55 or diagnosed with different conditions.55,56,71 The domains identified through this review appear to be common across these differences, but this was not entirely clear.
Fourth, only a few of the studies considered how users' communication experiences may, or may not, change over time,48,60,62 or how relatively compressed timeframes in settings such as intensive care can influence communication. 58
Fifth, specific consideration of the role of specialist pediatric palliative care was rare. This may be attributed to the recent emergence of pediatric palliative care as a recognized subspecialty and ongoing challenges to providing equitable access to this type of specialist care.7,24,80,81 Given recent research indicating that the involvement of specialist pediatric palliative care may influence users' communication experiences,12,82 this warrants further attention.
Sixth, focusing on self-reported experiences of communication required the exclusion of other qualitative approaches suitable for studying communication. For instance, recordings of actual interactions between users and professionals can be used to explore how they communicate with one another.33–35,83
Future research should consider ways to address these limitations.
Practice implications
There are clear practice implications highlighted by this review. A palliative approach to caring for children with life-limiting conditions aims to manage pain and other symptoms, enhance dignity and quality of life, and support psychosocial and spiritual wellbeing, encompassing both the patient and the family that cares for them.1,3,84,85 High-quality communication is crucial for achieving these aims.1,3,7,9–11,14
By systematically reviewing and synthesizing qualitative research investigating users' experiences of communicating with professionals, the present study highlights principles that should underpin professional practice. Wherever possible, professionals should focus on (1) exchanging information with users in a clear, open, and honest manner; (2) acknowledging the emotions of the different parties that are involved (patients, families, and professionals); (3) actively involving users in circumstances where this is appropriate and consistent with users' preferences; and (4) focusing on establishing trust and ongoing relationships, in which users can confidently communicate with professionals.
Footnotes
Acknowledgments
Peter Sondergeld and Sarah Howard, both librarians from the Queensland University of Technology library, assisted in the development of the search strategy used for this review.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.