
Abstract
Abstract
Background:
Outpatient palliative care (PC) has been shown to positively impact quality of life and decrease healthcare utilization, but there are limited data describing what activities render these benefits.
Objective:
Describe the topics addressed by an outpatient PC team during scheduled visits.
Design:
Longitudinal cohort study.
Setting:
The Symptom Management Service, an ambulatory PC program at an academic comprehensive cancer center.
Measurement:
Between March 23, 2015 and June 14, 2016, outpatient PC providers completed a checklist after each clinic visit, documenting topics covered during the visit.
Results:
During the study period, 1243 visits were conducted for 577 unique patients. Symptom management was the topic most commonly addressed during initial visits (in 92% of visits), followed by an introduction of PC (69%), support for family caregivers (47%), and communication with other clinicians (38%). Providers also supported patients to understand their prognosis (28%), treatment options (36%), and to make care decisions (22%). Formal advance care planning activities occurred infrequently, however, including designation of a Durable Power of Attorney for Healthcare (26%), completion of an advance directive or Provider Orders for Life-Sustaining Treatment form (10%), and discussing hospice (8%). Follow-up visits were dominated by symptom management (93%) and caregiver support (27%).
Conclusions:
Symptom management, support for family and caregivers, and care coordination are the most common activities that occurred during scheduled outpatient PC visits. These findings can guide developing PC practices, as well as clinicians who provide primary PC.
Introduction
P
Yoong et al. conducted a retrospective chart review study comparing the topics addressed during ambulatory PC and oncology visits at a program with documented efficacy. 23 They found that early PC visits focused on relationship building and promoting illness understanding; later visits focused on end-of-life planning; and symptom management and coping were addressed throughout. In this study we build on this work by describing the topics addressed during outpatient PC encounters at another cancer center to provide additional understanding about what we do—what is in the “palliative care syringe”—to guide teams developing outpatient PC services.25,26
Methods
Symptom Management Service
The outpatient PC program at UCSF's Helen Diller Family Comprehensive Cancer Center is called the Symptom Management Service (SMS). 27 This name was chosen when the practice was founded, over 12 years ago, with the goal of reducing barriers to referral. The team includes physicians, a nurse practitioner, a nurse, a program coordinator, and an administrative assistant. The team meets weekly to discuss cases with providers of multiple additional disciplines, including oncology social workers, chaplains, psychologists, and psychiatrists. The SMS provides care using a longitudinal co-management model, with routine collection of patient-reported outcomes regarding symptoms, quality of life, and spiritual well-being. “Telehealth” video conference visits are offered when patients are too ill to travel to clinic. Unscheduled communication between patients and the SMS team, through telephone and secure online messaging, occurs frequently between visits, including at the time of acute events, including hospitalizations.
Dataset
After each scheduled SMS visit, providers completed a checklist to document topics addressed during the visit (Table 1). The contents of the checklist were informed by recent literature and the experience of SMS providers.20,23,28 Because SMS visits are typically conducted by billing providers, the checklist pertained primarily to medical aspects of care; however, the family support item on the checklist inquired about psychosocial and/or spiritual support provided. Providers also documented information about the patient and visit (e.g., visit date, reason for referral, primary diagnosis, and Karnofsky Performance Status). 29
AD, advance directive; DPOA, durable power of attorney for healthcare; EMR, electronic medical record; POLST, Provider Orders for Life-Sustaining Treatment; SMS, Symptom Management Service.
Data for this study were collected from March 23, 2015 until June 14, 2016. Providers were directed to complete a checklist after every patient visit. However, as these data were collected by clinicians in the course of usual patient care, some data were missing; there was no effort to obtain missing data. Chart review was performed to determine if patients had died. This study was approved as part of the institutional review board approval for ongoing SMS quality improvement (QI) initiatives.
Statistical analysis
Descriptive statistics was calculated using Excel for Mac version 14.7.3. Patients who initiated care at the SMS and died within the study time period were further analyzed as a prespecified subgroup selected for further evaluation to provide information about what a full course of care in the SMS entails. There was no adjustment or imputation for missing data.
Results
During the study period, there were 1243 visits (330 initial and 913 follow-up) for 577 patients. Mean patient age was 59 years with 59% women. The most common diagnoses were breast (22%), lung (11%), and prostate (10%) cancer; 43% had metastatic disease. Median Karnofsky Performance Status score was 70. The most common reason for referral was pain (30%); advance care planning (ACP) was a reason for referral for only 7% of patients. The mean number of visits during the study period was 2.2 (Table 2).
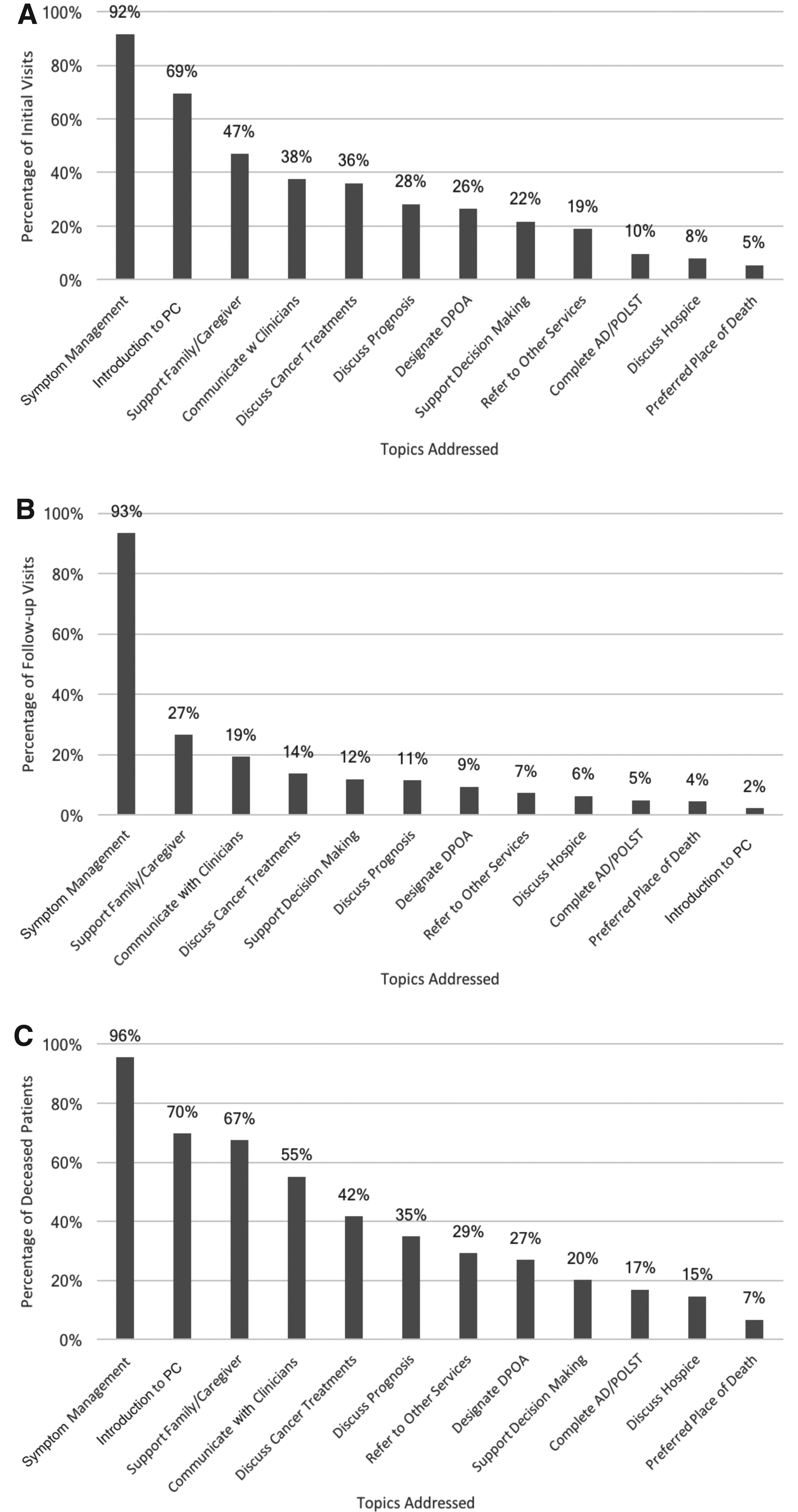
Symptom management was addressed in the vast majority of initial visits (92%) (Fig. 1A). The next most common activities were an introduction to PC (69%), support for family caregivers (47%), and communication with other clinicians (38%). Patients were also supported to understand their prognosis (28%), treatment options (36%), and to make decisions about their care (22%). Formal ACP activities occurred in a minority of initial visits, including designation of a Durable Power of Attorney (DPOA) for healthcare (26%), completion of an advance directive (AD) or Provider Orders for Life-Sustaining Treatment (POLST) form (10%), and discussion of hospice (8%).
(
During follow-up visits, symptom management dominated (93%), and support was also extended to caregivers (27%), while other topics were addressed less commonly (Fig. 1B).
Among decedents (89 patients, 162 visits), the mean time between first SMS visit and death was 135 days. The mean number of visits was 1.8. Topics addressed during the course of SMS care included symptom management (96%), introduction to PC (70%), support for family caregivers (67%), and communication with other clinicians (55%) (Fig. 1C). Elements of ACP were less commonly addressed, including designation of a DPOA (27%), support for decision making (20%), completion of an AD or POLST form (17%), and discussion of hospice (15%).
Discussion
We described topics covered during outpatient PC visits at our comprehensive cancer center. We found that introducing PC, managing symptoms, supporting families, and coordinating care are the most common activities that PC clinicians engage in. For a sizeable proportion of patients, time was also spent helping them understand their illness, prognosis, and treatment options. Formal ACP activities occurred for a minority of patients, although more frequently than requested by referring providers and at a similar rate as reported in previous literature. 30 This information can guide developing PC practices regarding how to structure their team and visits to efficiently cover core topics and develop systems to ensure important issues are addressed consistently. It can also inform clinicians providing primary PC about the activities central to this work.
The infrequency of formal ACP activities was surprising, and there are several likely explanations. First, our practice is called the SMS. Accordingly, symptom management is what referring providers and patients typically seek and expect from us. Developing practices should consider how the name they choose will influence their practice. Second, while we have a large interdisciplinary team available for support in challenging cases, our typical clinic visits are conducted by a physician or a nurse practitioner. We do not routinely have social workers or chaplains present at our visits and this undoubtedly impacts the content. Practices should carefully consider which team members are present at visits depending on the intention of those visits. Third, severe symptoms, such as pain and anxiety, are so distressing and distracting that we often focus on them first and sometimes we are not able to move on to important but less urgent topics such as ACP.
Notably, recent data from our institution demonstrated that early PC (provided more than 90 days before death) is associated with improved end-of-life care, including decreased healthcare utilization. 31 This raises the question of whether patients who receive care in the SMS make different decisions compared to patients who do not receive early PC, despite not commonly engaging in traditional ACP during SMS visits. We hypothesize that effective symptom management is an important way that we build trusting relationships with patients and families, allowing us to subsequently support them when they face care decisions. Even when we have focused on symptom management during clinic visits, we often support families between visits—through phone, secure messaging, and hospital or home visits—when they are facing a transition or crisis. We postulate that at those times we are able to draw upon what we know of patients' values and priorities to guide them and, in this way, provide “just-in-time care planning” rather than ACP. In fact, it may be that while discussing and documenting healthcare preferences in advance is helpful for some patients, developing trusting relationships with a care team who knows them and is available to them is a meaningful and appropriate goal for others. We aim to explore these hypotheses through future study examining the content and mode of our between-visit interactions and which aspects of outpatient PC are associated with outcomes of interest.
At the same time, we also see the infrequency of ACP in our clinic as quality gap and opportunity for improvement. The systematic measurement of the topics covered during our visits has highlighted this and allowed us to track our progress as we engage in QI, demonstrating the value of routine data collection. One early change that we have made is to ask patients on their previsit survey if they have a DPOA, who that person is, and whether they need more information about this topic. We have also started ACP workshops in which patients and families can learn about ACP and are supported to complete an AD. Furthermore, we now use an evidence-based online platform to support families to engage in ACP outside clinical encounters. 33 Similar processes could be adopted by other practices.
There are several important limitations of this study. First, this is a single-center study conducted in a large academic cancer center by a “Symptom Management Service,” which limits generalizability. The checklist was completed only during scheduled visits, rendering an incomplete view of care. In addition, the checklist was completed by busy providers; it is possible that some of the topics addressed were not indicated on the checklist or that providers could have varied in their interpretation of the topics, despite efforts to make them clear. As this work was conducted primarily for QI purposes, we did not formally test the inter-rater reliability of the provider checklist. Finally, our conceptualization of ACP was conservative; discussions about patients' disease, prognosis, and treatment options, which weren't considered formal ACP activities, may have substantially influenced care decisions.
In conclusion, key functions of our outpatient PC team are to provide symptom management, support for family caregivers, and care coordination. Formal ACP activities occur less frequently. Developing PC practices can learn from both our strengths and weaknesses. We also aim to explore these findings further through future study and engage in QI work informed by our findings.
Footnotes
Acknowledgments
The authors acknowledge the entire SMS team past and present, the other providers with whom we are lucky to collaborate, and our patients and families most of all. Without the stimulating, supportive community that surrounds us we wouldn't be able to do this work and learn from it.
Author Disclosure Statement
No competing financial interests exist.