
Abstract
Abstract
Background:
Chronic pain associated with serious illnesses is having a major impact on population health in the United States. Accountability for high quality care for community-dwelling patients with serious illnesses requires selection of metrics that capture the burden of chronic pain whose treatment may be enhanced or complicated by opioid use.
Objective:
Our aim was to evaluate options for assessing pain in seriously ill community dwelling adults, to discuss the use/abuse of opioids in individuals with chronic pain, and to suggest pain and opioid use metrics that can be considered for screening and evaluation of patient responses and quality care.
Design:
Structured literature review.
Measurements:
Evaluation of pain and opioid use assessment metrics and measures for their potential usefulness in the community.
Results:
Several pain and opioid assessment instruments are available for consideration. Yet, no one pain instrument has been identified as “the best” to assess pain in seriously ill community-dwelling patients. Screening tools exist that are specific to the assessment of risk in opioid management. Opioid screening can assess risk based on substance use history, general risk taking, and reward-seeking behavior.
Conclusions:
Accountability for high quality care for community-dwelling patients requires selection of metrics that will capture the burden of chronic pain and beneficial use or misuse of opioids. Future research is warranted to identify, modify, or develop instruments that contain important metrics, demonstrate a balance between sensitivity and specificity, and address patient preferences and quality outcomes.
Introduction
A
One standard analgesic treatment for moderate-to-severe pain is use of opioids. While opioids are often successful in minimizing pain, it is incumbent upon treating health professionals to be concerned about their potentially serious adverse consequences such as injury, dependence, addiction, and death. Indeed, the current opioid epidemic and associated increased death rates have highlighted these concerns. 2 Consideration of opioid use risk is an essential element for determining accountability for high-quality care delivery to community-dwelling patients with serious illnesses. This article has three aims: (1) to present options for assessing pain in seriously ill community dwelling adults according to their ability to communicate by proposing pain metrics that are effective representations of the patient's condition; (2) to discuss the use of opioids, as appropriate, and their intended and unintended consequences, in patients with serious illnesses; and, (3) to suggest accountability measures for use during pain treatment that can promote quality care and minimize adverse consequences in seriously ill patients.
Assessing and Recording Chronic Pain Metrics
Defining and classifying chronic pain through use of pain metrics
Metrics that define and classify chronic pain provide a focus for professional interventions and evaluation of quality of care. Selecting quality pain metrics requires answers to these questions: (1) what pain metrics are necessary for a screening examination to identify pain? (2) will the patient have the capacity to provide information about the pain metrics, or will input from a patient's family member, surrogate, or health professional be necessary? (3) if a screening examination is positive for chronic pain, what pain metrics are necessary to capture the dimensions, burdens, and impact of pain on the seriously ill patient and response to treatment?
The definition of pain has evolved over the years but still retains the characteristic of being a distressing experience associated with actual or potential tissue damage. (See Table 1 for a glossary of terms.) Pain is recognized as having sensory, emotional, cognitive, and social components, the latter making pain a shared experience. Chronic pain, when described by a time frame, is that which persists past the normal time of healing or lasting at least three months. 6 When chronic, or persistent, pain is associated with substantial restriction of participation in work, social, and self-care activities for six months or more, it is identified as high impact chronic pain. 7 However, looking beyond a time framework for classifying chronic pain, consideration must be given to the mechanisms and burden of pain 8 and recognize that pain classification can evolve over time and new discoveries. 9 Indeed, a new classification is currently under development. 10
Pain metrics
The important characteristics and domains of pain are identified by instruments and systems with specific pain metrics. (See Table 2 which outlines the relationship among pain domains, metrics, and instruments.) Pain domains as targets for assessment can include pain's sensory and affective qualities, its temporal characteristics, its location and bodily distribution, pain behaviors, and psychological impact on function.1,11,12 Ascertaining the details of a patient's pain relies on a patient's ability to reliably communicate their pain experience and to access individuals and systems that capture pain information. A comprehensive pain assessment would optimally include use of metrics for each domain, while a screening pain assessment would be more focused. Providers are required to gather “enough information” to make treatment decisions and evaluate outcomes for which they are accountable. Gathering pain data from community dwelling individuals with serious illnesses may require a triaging process that begins with more simple interrogations.
The first five domains on left represent those deemed most important, in order of importance, by Palliative Care clinician experts. 28
Behaviors for nonself-reporting patients.
BPI-SF, Brief Pain Inventory-Short Form; DOLOPLUS-2, Abbreviation for a French-language scale; MOBID, Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale; MPQ-SF, McGill Pain Questionnaire-Short Form; NRS, numeric rating scale; PACSLAC, Pain Assessment Checklist for Seniors with Limited Ability to Communicate; PAINAD, Pain Assessment in Advanced Dementia Scale; PD-Q, painDETECT questionnaire; PEG, Pain Intensity, Enjoyment, General Activity; PROMIS, Patient-Reported Outcomes Measurement Information System; RAI, Resident Assessment Instrument; VAS, visual analog scale; VRS, verbal rating scale.
Unidimensional pain measures and short questionnaires
Simple interrogations generate data from use of unidimensional measures and brief questionnaires by patients who can self-report and/or self-record. Well validated unidimensional numeric rating scale (NRS) and visual analog scale (VAS) are often used to quantify degree of pain intensity and, less often, degree of pain distress. 13 However, simply focusing on a pain intensity number provided by patients with chronic pain can be problematic since one number does not reflect the total burden of chronic pain. A decrease in a number may not serve as a metric of treatment outcome success 14 ; nor can chronic pain treatment be unsuccessful even when a pain intensity number does not change. 15
There are a number of brief questionnaires that focus on multidimensional domains of pain: the Brief Pain Inventory (BPI), the Short Form-McGill Pain Questionnaire (SF-MPQ), the PEG, and the painDETECT. The BPI is a short self-administered questionnaire that assesses pain severity, as well as its impact on function. 16 The BPI-Short Form (BPI-SF) has been used to identify characteristics of breakthrough pain in patients with cancer-related pain in remission. 17 The SF-MPQ is also a self-administered questionnaire that addresses sensory, affective, and cognitive (evaluative) domains of pain 18 and correlates highly with the well validated Long Form-MPQ. 19 The PEG is a 3-item scale that measures pain intensity (P), interference with enjoyment of life (E), and interference with general activity (G). 20 It has been tested against the BPI for reliability and content validity and has been shown responsivity to clinical interventions. 21 Recent Center for Disease Control (CDC) Guidelines 2 offer the PEG as one example of an instrument to assess treatment outcomes. Finally, the painDETECT questionnaire (PD-Q) evaluates symptoms associated with neuropathic versus nociceptive pain. Since patients with neuropathic pain often suffer more severely than patients with nociceptive pain, 22 a tool such as the PD-Q may help with better diagnosis and treatment.
Behavioral pain measures
Some patients with serious illnesses are unable to self-report their pain due to impaired cognitive capacity associated with delirium, dementia, and/or somnolence. Assessing behavioral indices as proxy measures of pain can help to identify people with chronic pain and make them more likely to receive therapeutic interventions.
Pain behaviors noted by healthcare workers in patient medical records in a palliative care center included patient vocalizations such as moans or groans or crying out; facial expressions such as grimaces and winces; and actions such as holding a body part and clenching fists. 23 Recognition of these behaviors in a palliative care population may assist with development and validation of a pain behavior tool for seriously ill patients in those and other settings. One such tool is the MOBID scale (Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale). 24 The MOBID has been tested in nondelirious, nonpsychotic nursing home patients with dementia suspected to have chronic pain of >3 on a 0–10 NRS intensity scale. Researchers identified the following: pain behaviors were more frequently observed during mobility than rest; observer-generated NRS pain intensity scores and number of behaviors observed were positively correlated; and the best agreement between the testers was for pain noises, although facial expression was demonstrated most frequently. Observation and recording of behaviors by family members or health professionals that may indicate pain deserve careful consideration as a metric-generating activity in seriously ill community-based patients unable to reliably self-report.
Several other pain behavior scales have been developed for older persons with severe cognitive impairment, such as the PAINAD, PACSLAC, and the DOLOPLUS-2 (see footnote of Table 2 for full name of scales). Psychometric properties of these three scales were tested in Dutch nursing home residents. 25 The PACSLAC had better psychometric attributes and was found to be more “user friendly” to raters than the other two scales. However, the testing paradigm was acute (vaccination) pain rather than chronic pain. Items on the PACSLAC and PAINAD could be examined for their applicability to a newly constructed behavioral assessment scale that may reflect chronic pain in persons with serious illnesses.
Use of electronic healthcare data to assess pain and its impact on the person
von Korff et al. 1 pilot tested a 25-item electronic pain survey in a sample of patients in a large group health plan in Washington, with most items derived from established questionnaires. Answers to three specific questions allowed for categorization of respondents as persons with high-impact chronic pain (14% of 365 respondents) versus those with moderate-impact chronic pain (19% of respondents.) There were clear differences between the two groups in responses to survey questions regarding frequency of healthcare use, level of pain intensity, level of life interference, and higher number of painful body sites. This led to researcher confidence that responding to questions on an electronic health survey would be feasible and beneficial in identifying primary care, population-based patients with moderate-to-high impact chronic pain.
A second electronic database, Patient-Reported Outcomes Measurement Information System (PROMIS), 26 was developed by academic scientists, primarily for research purposes, from several institutions and the NIH as a computerized bank of measures of patient symptoms, functional status, and quality of life. There is a pain intensity question as part of a global health scale, and there are two pain measures, pain behavior (a 7-item short form) and pain interference (a 6-item short form), that showed good reliability and validity. The PROMIS short form was a less sensitive measure of pain interference than the BPI or the PEG when used with patients with moderate musculoskeletal pain. 21 Nevertheless, PROMIS has shown to be efficient, flexible, and precise; its item bank is available for public use and items can be made part of an Internet survey platform. 26
A third large electronic database is one used in nursing homes certified by Medicare and Medicaid to assess residents' strengths and needs through comprehensive assessments to help ensure that a resident's quality of life is maintained or improved through quality care. The Long-Term Care Facility Resident Assessment Instrument (RAI) 3.027 contains one section, “Section J, Health Conditions in the Minimum Data Set,” which includes questions about pain that require self-report by the resident: pain presence, intensity, frequency, and effect on function. When residents are unable to self-report, staff complete questions about behavioral indicators of pain or possible pain. These data are used to identify interventions to meet the resident's individual needs and to monitor the quality of care provided. However, these metrics are specific to pain that the resident experienced over a previous five-day period of assessment, not necessarily chronic pain.
A palliative care perspective on assessing pain
Pain metrics deemed important to assess in patients with advanced cancer receiving palliative care were identified during a systematic search of pain assessment literature. 28 Six pain and palliative care physician experts ranked pain dimensions for relevance and importance. The first five of a list of 10 in order of deemed importance were the following: pain intensity, temporal pattern, treatment and exacerbating/relieving factors, location, and interference. In an update to this work, 29 11 new tools were identified in the literature, but none was found to be inclusive. Experts (n = 32) again ranked the five most relevant dimensions of pain to be assessed within a 24 hour time window, with the substitution of pain quality for interference (No. 6 on this list).
Despite the work described above, no one pain instrument has been identified as “the best” to assess pain in seriously ill patients. However, consideration of the “right metrics” for capturing a seriously ill individual's experience of chronic pain is based on an understanding of the possibilities. These data may lead the healthcare provider to conduct a more comprehensive assessment to consider factors that may be influencing current and proposed pain treatment.
Treatment of Chronic Pain Through Use of Opioids
One important avenue of exploration is the role of opioid therapy for seriously ill patients with chronic pain. It is essential to consider that all pains are not equal; there are some conditions that are opioid responsive; some that may be; and others for which opioids are not indicated. Recent CDC Guidelines 2 recommend that prescribers reconsider the use of opioids for chronic noncancer pain, leading to an increased awareness of patients of the dangers of opioids. However, they fall short in providing guidance for use in patients with cancer or other serious illnesses. In addition, Baker 30 warns that care should be taken in establishing new standards, as is being done by The Joint Commission, to avoid the risk of moving the care pendulum away from good pain management. Decreased opioid prescribing may leave a subset of patients, such as those who are seriously ill, with no effective options to manage their unique chronic pain. For this reason, it is important that we continue to gather evidence to determine condition-specific guidelines for pain management. According to recent Clinical Practice Guidelines from the American Society of Clinical Oncology, 31 consideration should be given to the use of nonopioid and adjuvant analgesics for chronic pain in patients with cancer. The Guidelines note that, for patients who do not respond to these more conservative measures and have continued distress and impairment of function, a trial of opioids can be considered. While they are not effective for many conditions, 32 there is evidence to identify when opioids should and should not be used, even within the context of serious illness. 33 It is essential to consider metrics to evaluate the effectiveness of opioids, as well as the risks of their use, especially considering the current opioid epidemic.
Balancing the use and misuse of opioids
Determining if an opioid is effective and if a patient is using an opioid appropriately requires considerable vigilance and time.34,35 While opioids can diminish suffering for those in pain, their abuse, misuse, and addiction potential (see Table 1 for definitions) can impact community and population health. Figure 1 provides an algorithm for a screening or a comprehensive assessment of pain and opioid use. The CDC has demonstrated that opioid-related deaths have been increasing over the past 10 years (Fig. 2) with much of the increase attributable to increasing opioid prescriptions. Currently, the estimation is that 3–20% of patients prescribed an opioid will be addicted.2,36 However, rather than stigmatizing individuals who are susceptible to opioid addiction, monitoring and instituting a shared plan for aiding individuals who do become addicted is necessary.
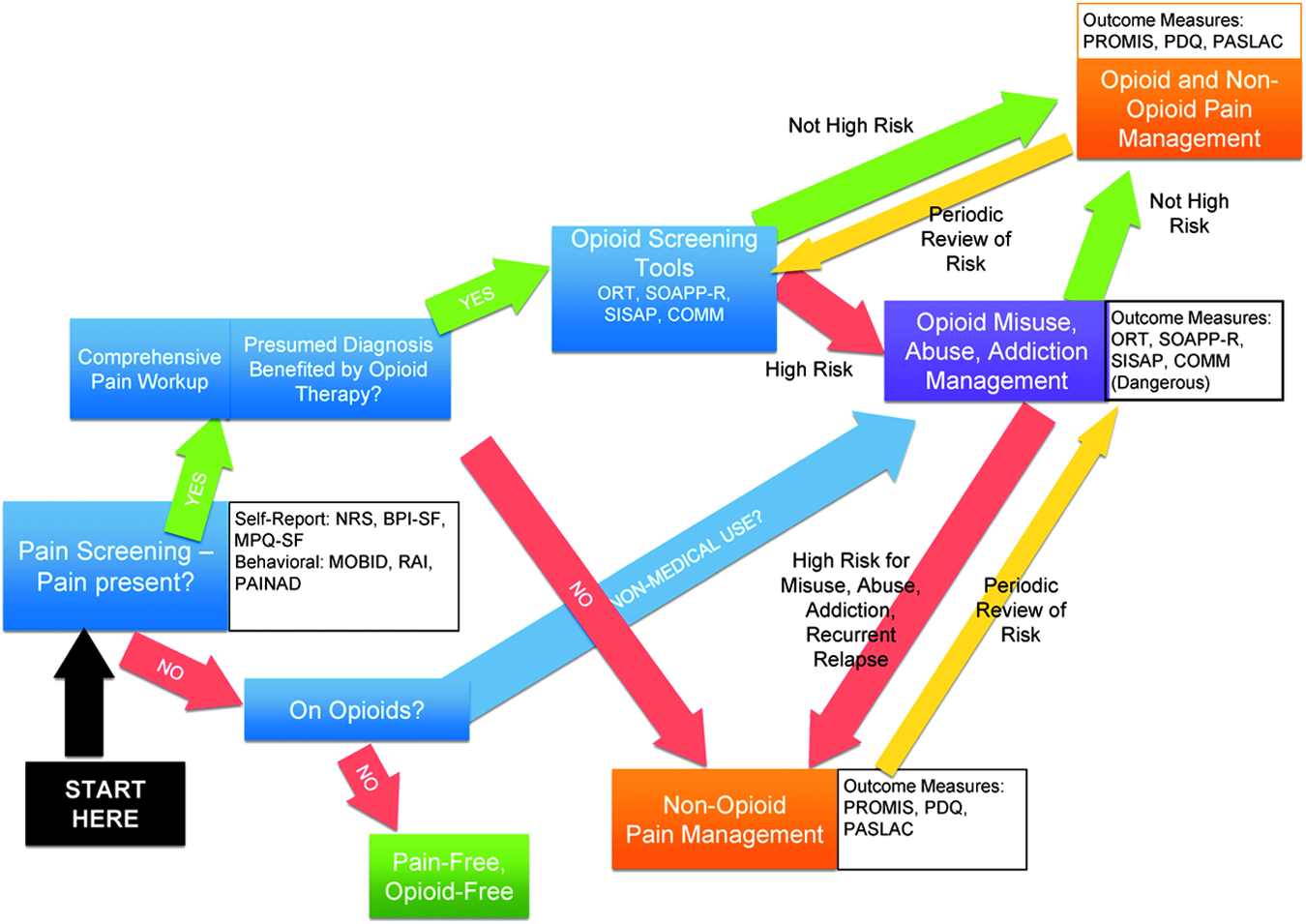
Algorithm for pain screening metrics in the setting of Potential Opioid Misuse, Abuse, and Addiction. In this figure, we present a decision tree highlighting the interplay among pain assessment, pain management, opioid risk assessment, opioid benefit, and opioid management for community-based care. BPI-SF, Brief Pain Inventory-Short Form; COMM, Current Opioid Misuse Measure; MOBID, Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale; MPQ-SF, McGill Pain Questionnaire-Short Form; NRS, numeric rating scale; ORT, Opioid Risk Tool; PAINAD, Pain Assessment in Advanced Dementia Scale; PACSLAC, Pain Assessment Checklist for Seniors with Limited Ability to Communicate; PD-Q, painDETECT questionnaire ; PROMIS, Patient-Reported Outcomes Measurement Information System; RAI, Resident Assessment Instrument; SISAP, Screening Instrument for Substance Abuse Potential; SOAPP-R, Screener and Opioid Assessment for Patients with Pain—Revised.
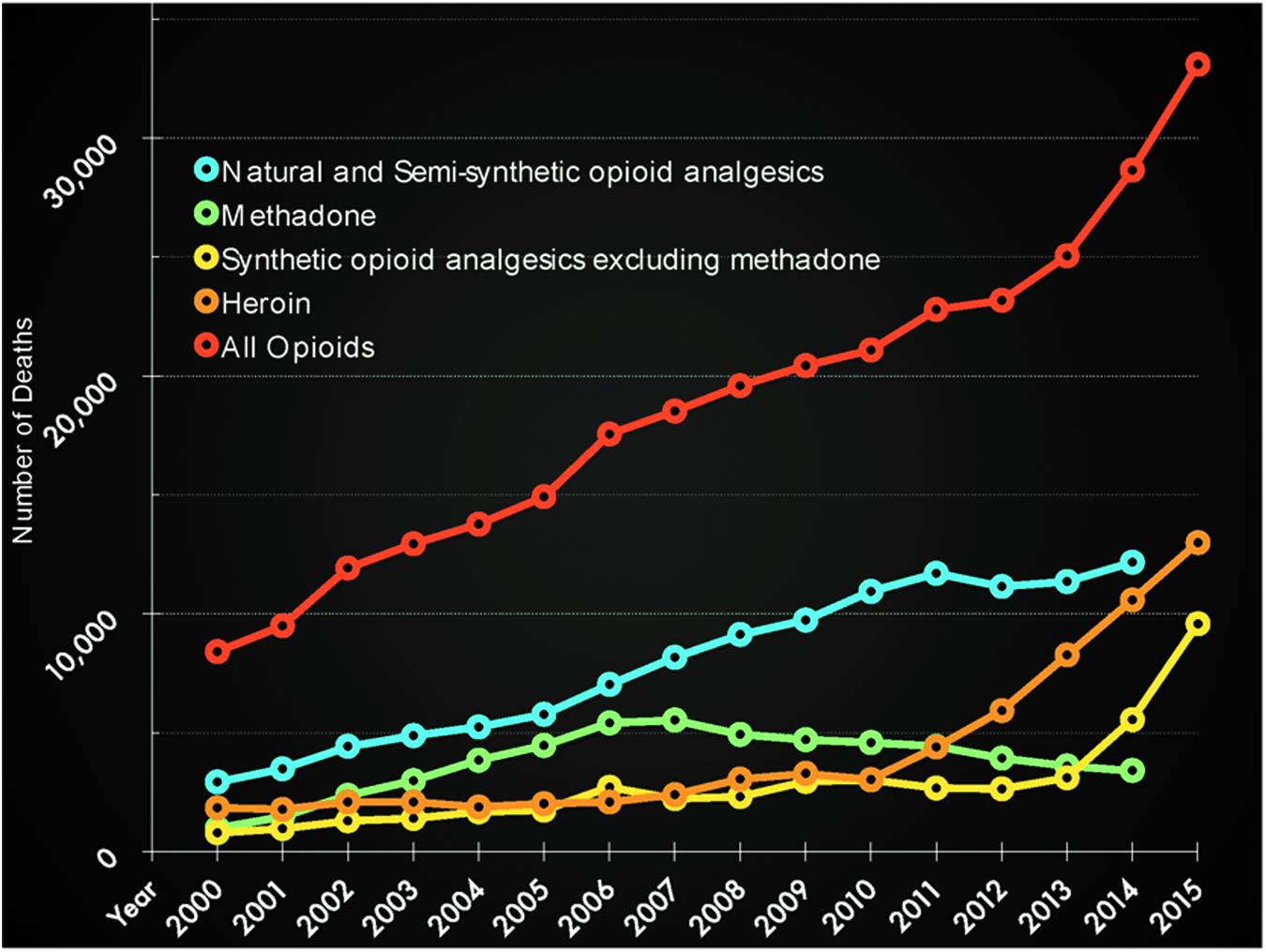
Number of deaths related to opioids per year in the United States 2000–2015. CDC Wonder Data. Stratification based on opioid type: Natural and Semi-Synthetics (e.g., morphine, hydromorphone), Methadone, Synthetics excluding Methadone (e.g., fentanyl, carfentanil), Heroin, and All Opioids. CDC, Center for Disease Control.
Assessing the risk/benefit ratio of treating pain with opioids
Provider education of patients regarding the myriad risks of opioids is time consuming. The patient–provider relationship in American medicine has been affected by multiple forces, including managed care, medicine as a business, and shortened physician visits leading to quick decision making. Yet a shared decision-making model of medicine is paramount when it comes to the complex issue of opioid management. Assessing risk for opioid misuse can help providers understand how their patients may fare with potentially abusive and addictive substances. Guidelines suggest that clinicians take a “universal precautions” approach to minimize adverse consequences of opioid use 31 (p. 3339). The beneficial effects of opioids are important to note: improved function in activities of daily living, decreased pain severity, decreased pain interference, and improved quality of life. Clinicians must also recognize the risks of opioid therapy with an individual patient. Table 3 provides a checklist of opioid therapy risks. In addition, clinicians can use specific opioid risk screening tools to assess risk based on substance use history, general risk taking, and reward-seeking behavior. There are several screening tools specific to the assessment of risk in opioid management that can be incorporated into a community-based assessment of chronic pain and opioid use37–39 (Table 4). Research is still needed on continued psychometric evaluation of these existing and newly developed instruments and the effects of their use in evaluating clinical outcomes. 40
Determining Accountability for Quality Care: Selecting Pain and Opioid Metrics
Determining accountability for quality care of patients with serious illness who have chronic pain is complex. Selection of pain metrics is a context-dependent process depending on the patient's ability to report their pain; whether patients are in primary care, managed care, or residential care and; what type of data is required by health systems and funding agencies to address their outcomes of interest. Quality outcomes of interest would include whether pain was identified through proper screening and comprehensive assessments and that the patient's relief from pain and their quality of life and functional capacity are improved with pain treatment. 31 Table 2 provides a grid of pain instruments that can be considered according to whether pain self-report is an option or whether proxy observation of patients' behaviors is required. Quality outcomes would include assessment of the appropriateness of pain treatment and treatment results. Ineffective or adverse results from treatment require accountability.
Measures of accountability regarding the use and effectiveness of opioids must take the particular patient's situation in mind. Clinician concern about the use of opioids can sometimes depend on their estimates of the patient's life expectancy, being less concerned with patients in hospice settings and more concerned with patients who have a longer course of treatment. Nevertheless, clinicians' decision making regarding opioid use, especially with their attendant risks and ongoing monitoring of the balance of their effectiveness and risks, should be transparent. Table 4 suggests opioid risk tools that can be used on an ongoing basis for patients with chronic pain receiving opioids, to identify special needs. Identifying, intervening, and evaluating intervention results can improve accountability and quality care. Figure 1 offers an algorithm for screening patients' pain and opioid use while identifying instruments for consideration.
Conclusion
Accountability for high quality care for community-dwelling patients with serious illnesses requires selection of metrics that will capture the burden of chronic pain whose treatment may be enhanced or complicated by opioid use. Community-based care will need to be accountable through selection of, and attention to, appropriate pain and opioid metrics. Future research is warranted to identify, modify, or develop instruments that contain important metrics, demonstrate a balance between sensitivity and specificity, and, importantly, speak to the preferences of patients with serious illnesses.
Footnotes
Author Disclosure Statement
K.P., RN, PhD has no competing financial interests. R.K.N., MD receives honoraria from Abbott, Halyard Health, and Sonosite.