
Abstract
Abstract
Background:
Drug interactions are a common cause for escalation of debilitating symptoms in palliative care patients. CYP3A is the most relevant CYP enzyme in humans involved in metabolism of about half of all available pharmaceuticals.
Objective:
To increase knowledge about the CYP3A enzyme and the impact of drug interactions on its activity to improve dosing in palliative care patients.
Design:
The prospective clinical trial uses a secure method of analyzing CYP3A activity in humans: Administration of a marker substance followed by the determination of its blood concentrations as well as the concentrations of its metabolite at certain points of time and corresponding metabolic clearance calculations.
Setting:
The ongoing trial is carried out at a palliative care unit under real-life clinical conditions.
Measurements:
A four-hour pharmacokinetic profile after oral administration of the marker substance (microdose of midazolam) will be obtained from each enrolled patient. Plasma concentrations of midazolam and its primary metabolite will be quantified by mass spectrometry techniques. CYP3A activity will be calculated as partial metabolic clearance from a limited sampling area under the curve. All other drugs taken by the participating patients will be considered as well as recent blood test results and the patients' diagnoses.
Conclusions:
This is the first prospective study dealing with drug metabolism in patients on a palliative care unit. The trial is based on reliable and established methods aiming to provide improved dosing regimens and thus optimize pharmacological therapies in this specialty.
Introduction
W
CYP3A is the most relevant CYP enzyme in humans and is involved in metabolism of about half of all available pharmaceuticals. It is known that activity of CYP3A has a high interindividual variability and can differ up to 30-fold. Drug interactions are also caused by pharmaceuticals acting as an inducer or an inhibitor of the CYP enzymes. 1
Drug interactions are a common cause for escalation of debilitating symptoms in palliative care patients and, therefore, can negatively impact the patients' quality of life. 2 Furthermore, evidence-based guidelines for dosing palliative drug regimens are hard to find in respective literature. Knowledge about the CYP3A activity could improve dosing in palliative care patients and help to avoid adverse effects due to drug interactions. 3
A method of analyzing CYP3A activity in humans, which causes minimal risks for the involved patients, was recently established. 4 After application of a microdose of the benzodiazepine midazolam (used as a CYP3A marker substance), the quantification of its plasma concentrations over time is carried out. The partial metabolic clearance of midazolam to its metabolite 1′-OH-midazolam can be calculated from the plasma exposure data and serve as a measure of the CYP3A activity.5,6 This method has already been used to obtain information on the CYP3A activity in healthy volunteers as well as in patients.4,7,8
With the intention to show that it is possible to conduct a clinical trial in a palliative care setting under phase I conditions, our study was carried out on a palliative care unit under real-life clinical conditions.
Methods
Study design
After approval by the local ethics committee of the medical faculty of the University of Heidelberg, this prospective clinical study started in April 2016 at the palliative care unit of Heidelberg University Hospital (Heidelberg, Germany) and is still ongoing.
Every patient admitted on the ward who is at least 18 years of age will be screened for possible participation independent of the individual performance status. Exclusion criteria are hemoglobin <7.5 g/dL at the last laboratory screening (within the last seven days), the need for red blood cell transfusions on a regular basis, inability to communicate well with the investigator due to language problems, poor mental development, or cognitive impairment such as delirium (Table 1). If a patient would qualify, he or she will be informed about the clinical study and a written informed consent will be obtained before any study-related activity.
RBC, red blood cell.
A four-hour pharmacokinetic profile after oral administration of the marker substance (a microdose of 10 μg midazolam) will be obtained from each participating patient. The marker substance will be offered to the participants in the form of a solution in water. Administration will be supervised by one of the investigators (Fig. 1). There is the option to repeat this procedure three times if required.
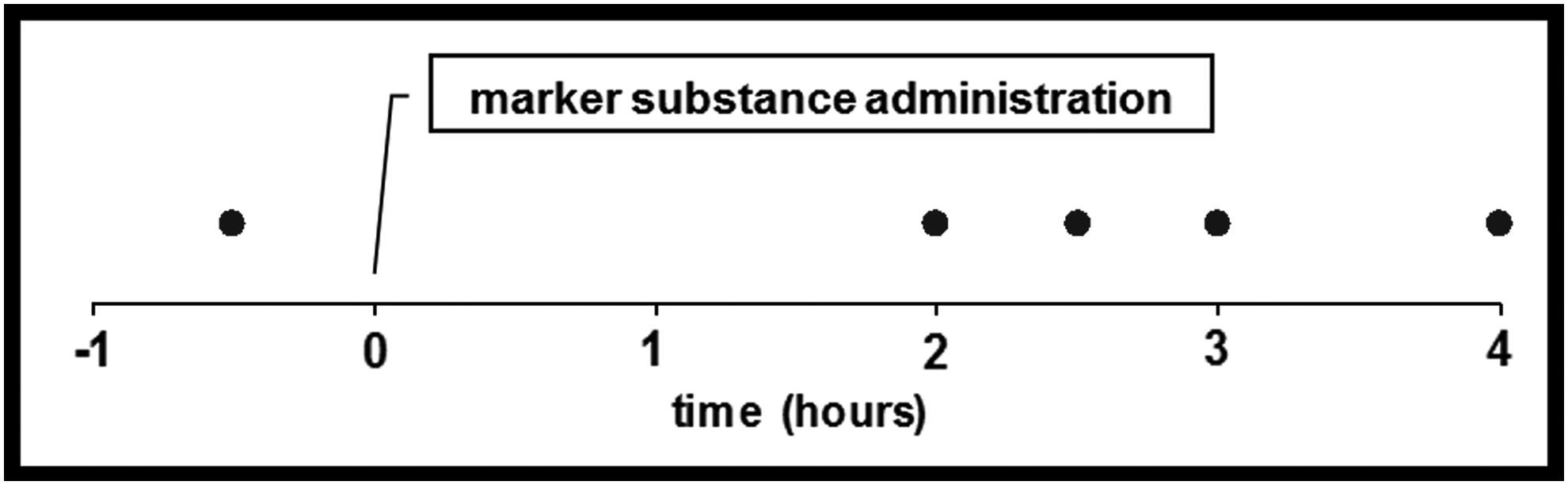
Blood sample collection in case of oral administration of the marker substance.
If an enrolled patient receives an intravenous midazolam infusion out of a medical indication to treat a certain debilitating symptom as regular drug therapy, a steady-state blood sample is necessary to determine the CYP3A activity. Steady state is declared after 12 hours constant dosing without administration of bolus doses. In this case, midazolam is prescribed by the treating physicians for medical reasons and will not be modified in any way for study reasons by the investigators (Fig. 2).

Blood sample collection in case of intravenous midazolam administration.
Definition of endpoints
1. CYP3A activity in individual patients with various genetic predisposition and specific underlying diseases on a palliative care unit during real clinical conditions in comparison with healthy volunteers or other patients.
2. Necessity of dose adjustment for palliative care patients if CYP3A inductors or inhibitors are combined with CYP3A substrates.
Sample collection
Blood samples (2.7 mL) for determining plasma concentrations of midazolam and its metabolite will be collected in lithium heparin tubes immediately before dosing and at two, two and half, three, and four hours postoral administration of the marker substance.
In case of intravenous midazolam administration out of a medical indication of the treating physicians, a steady-state blood sample will be collected not earlier than 12 hours after the start of a constant rate infusion to assure steady-state conditions. Up to four blood samples can be taken at steady state.
Blood samples will be immediately centrifuged at 4°C and the separated plasma will be stored at −20°C until analysis.
Data collection
Duration, dosage, and type of administration of all other drugs taken by the participating patients will be evaluated to identify possible drug–drug interactions. 9 Furthermore, recent blood test results and principal as well as secondary diagnoses will be considered.
Analytical assays
Midazolam and 1′-OH-midazolam plasma concentrations will be quantified by using high-performance liquid chromatography with tandem mass spectrometric (LC/MS/MS) detection methods as previously described with a lower limit of quantification of 0.093 pg mL−1 for midazolam and 0.281 pg mL−1 for 1′-OH-midazolam. 4
Sample size and data analysis
As there are no data available so far providing a hypothesis regarding the defined endpoint of CYP3A activity (alteration of CYP3A activity), no sample size calculation is done. The maximum of individuals being examined in this trial should not exceed 100 patients.
CYP3A activity will be calculated by the partial metabolic clearance of midazolam (limited sampling strategy) as done in other trials before.4,6,7
In respect of the participants' heterogeneous and complex medications, each patient has to be investigated individually. Comparison of CYP3A activity of the enrolled subjects and published data of healthy volunteers or other patients of former trials will undergo nonparametric analysis with the Mann–Whitney test.
Discussion
This is the first prospective study dealing with drug metabolism in patients on a palliative care unit. The trial will be closed prematurely if only a deficient number of patients are willing to attend. Drop-out criterion for participating patients will be the individual withdrawal of the informed consent. The study is based on reliable methods described and published before aiming to improve dosing regimens and thus optimize pharmacological therapies in this specialty. The outcomes are planned to be presented at scientific meetings and will be submitted for publication in a peer-reviewed journal.
Footnotes
Author Disclosure Statement
The authors declare that they have no actual or potential competing interests.
The study protocol was approved by the ethics committee of Heidelberg University Hospital (Heidelberg, Germany; approval number S-398/2015). The ongoing trial is conducted in accordance with good clinical practice and the Declaration of Helsinki. We obtain written informed consent from each patient before any study-related activity. The trial was registered at German Clinical Trials Register (DRKS00011753).