
Abstract
Abstract
Background:
Pain is a widely neglected symptom in patients with amyotrophic lateral sclerosis (ALS), even though it may be common and have a significant impact on the quality of life.
Objective:
The aim of this study was to determine the frequency and characteristics of pain and its treatment in ALS patients.
Design:
A multicenter cross-sectional study.
Setting/Subjects:
Eighty patients with ALS from eight hospitals.
Measurements:
Data on demographics, functional status, and pharmacological treatment were collected. The Barthel Index (BI) was used to assess functional status. Pain was measured using the 0–5-point Wong-Baker FACES Pain Rating Scale.
Results:
Pain was reported by 53.8% of ALS patients, and 36.3% reported receiving pain medication. Opioids were the drugs most commonly used to treat pain. The differences in pain frequency according to functional status were not statistically significant (p = 0.38). The pain intensity in patients whose functional status was total dependence (BI 0–20, 2.5 ± 1.2) was significantly worse than that in those with better functional status (BI 21–60, 1.4 ± 0.7; BI 61–99, 1.4 ± 0.5; p < 0.01).
Conclusions:
Our study indicates that all patients with ALS have the potential to suffer from pain, the intensity of which increases with decreased functional status.
Introduction
A
Although pain has been a widely neglected symptom in patients with ALS, several recent studies have focused on pain in these patients.2,3 Pain has been reported to occur in less than 15% to up to 85% of patients with ALS.4–10 Pain has been shown to be associated with diminished quality of life and a higher incidence of depression in patients with ALS,4,6,11 and to be the main cause of suffering in the final stages of the disease. 12 The cause of pain in patients with ALS is presumed to arise from inactivity because of atrophy, muscle cramps, spasticity, or pressure areas on the skin caused by immobility. Moreover, there have been occasional reports of pain with neuropathic characteristics in these patients.6,13 Treatments for pain in ALS include pharmacological and nonpharmacological interventions and are selected according to the cause of pain. The first-line treatment is usually nonopioid analgesics, including acetaminophen or nonsteroidal anti-inflammatory agents (NSAIDs). Opioids are generally used if these drugs fail to relieve the pain. 14
The objective of this study was to determine the frequency and characteristics of pain and its treatment in patients with ALS and to describe the relationship between pain and functional status in these patients.
Methods
This multicenter cross-sectional study was conducted in eight hospitals that are members of Tokai Hokuriku National Hospital Pharmacists Association in Japan (National Hospital Organization Iou Hospital, National Hospital Organization Toyama Hospital, Shizuoka Institute of Epilepsy and Neurological Disorders, National Hospital Organization Shizuoka-Fuji Hospital, National Hospital Organization Tenryu Hospital, National Hospital Organization Higashinagoya National Hospital, National Hospital Organization Mie Hospital, and National Hospital Organization Suzuka Hospital). The study protocol was approved by the Institutional Ethics Boards of all the participating hospitals and was performed according to the principles set out in the Declaration of Helsinki and Japanese Ethical Guidelines for Clinical Research. All study participants provided informed consent.
Subjects
Eighty patients with a diagnosis of ALS according to the El Escorial criteria 15 were recruited for this study between May 1, 2015 and May 31, 2015. The only exclusion criterion was cognitive impairment, including frontotemporal dementia, which would have affected the patient's ability to respond to a questionnaire.
Pain questionnaire
The patients were asked to answer a questionnaire about pain. Patients who were unable to write, provided feedback verbally or by other means of communication. The questionnaire was administered after ethical approval was received. The outcome measures were: presence of pain; description of pain; location of pain; type of pain; and average and worst pain intensity on the previous day, assessed by the Wong-Baker Faces Pain Rating Scale (WBS), where the patient marks one of six faces that best describes the pain intensity. This scale is numbered from 0 to 5 points. 16 The WBS was chosen because most of the participants in this study had a serious communication problem.
Physical parameters
Data on disease duration, time since diagnosis, anatomic site of onset, information about drugs used for pain relief, and whether or not the patient was being ventilated (invasively or noninvasively) and/or tube fed were obtained from medical records at the same time as patients completed the pain questionnaire. Functional status was assessed using the Barthel Index (BI), which includes 10 items, that is, feeding, grooming, bathing, dressing, bowel and bladder care, toileting, ambulation, transfers, and climbing stairs. Each performance item is rated, with the sum of all items indicating the patient's ability to perform activities of daily living. 17 The maximum possible score is 100, which indicates that the patient is fully independent in physical functioning. The lowest score is 0, which represents complete physical dependence and a bedridden state. The BI score is classified into four categories: 0–20, total dependence; 21–60, high dependence; 61–99, moderate dependence; and 100, full independence.
Statistical analyses
Data are reported as the mean and standard deviation or as the median or frequency. Medians were compared using the Mann–Whitney U test. Frequencies were compared using the chi-squared test. The correlation between pain intensity and BI score was analyzed using the Kruskal–Wallis test. A p-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS version 19.0 software (IBM Corp., Armonk, NY).
Results
The demographic and clinical characteristics of the 80 patients with ALS enrolled in this study are listed in Table 1. The mean patient age was 65.0 ± 10.6 years and the average time since onset of symptoms was 5.0 ± 7.7 years. Forty-four patients (55.0%) were receiving mechanical ventilation and 51 (63.8%) were being tube fed. Forty-three patients (53.8%) reported having pain. Patients with pain were younger than those without pain (63.0 years vs. 67.0 years; p = 0.04). The other demographic characteristics were very similar between the groups with and without pain; there was no significant difference in sex distribution (p = 0.93) or in time since symptom onset between the two groups (p = 0.57). Twenty-nine (36.3%) of the 80 patients were receiving pain medication, which was usually an opioid (10/29, 34.5%). All patients using opioids were in the BI 0–20 category. Other frequently prescribed pain medications were nonopioid analgesics (NSAIDs and acetaminophen), antidepressants, antiepileptics, and muscle relaxants.
Data are shown as either the n (%) or the median (range).
IPPV, intermittent positive pressure ventilation; NPPV, noninvasive positive pressure ventilation; NSAIDs, nonsteroidal anti-inflammatory drugs.
Table 2 shows the relationship between presence of pain and functional status (BI). The difference in frequency of pain according to BI score was not statistically significant (p = 0.38). The relationship between pain intensity and BI score is shown in Table 3. On the day before completing the questionnaire, the average pain intensity was 2.1 ± 1.2 on the 0–5-point WBS. The pain intensity was significantly greater in patients who were totally dependent (BI 0–20: 2.5 ± 1.2) than in patients in the other functional status groups (1.4 ± 0.7 in the BI 21–60 group and 1.4 ± 0.5 in the BI 61–99 group; p < 0.01). The anatomic distribution of pain is shown in Figure 1. The most frequent location of the pain was in the upper and lower extremities, shoulder, neck, back, and hip in patients with a BI of 0–20 and in the shoulder, neck, and upper extremities in patients with a BI of 21–60 or 61–99.
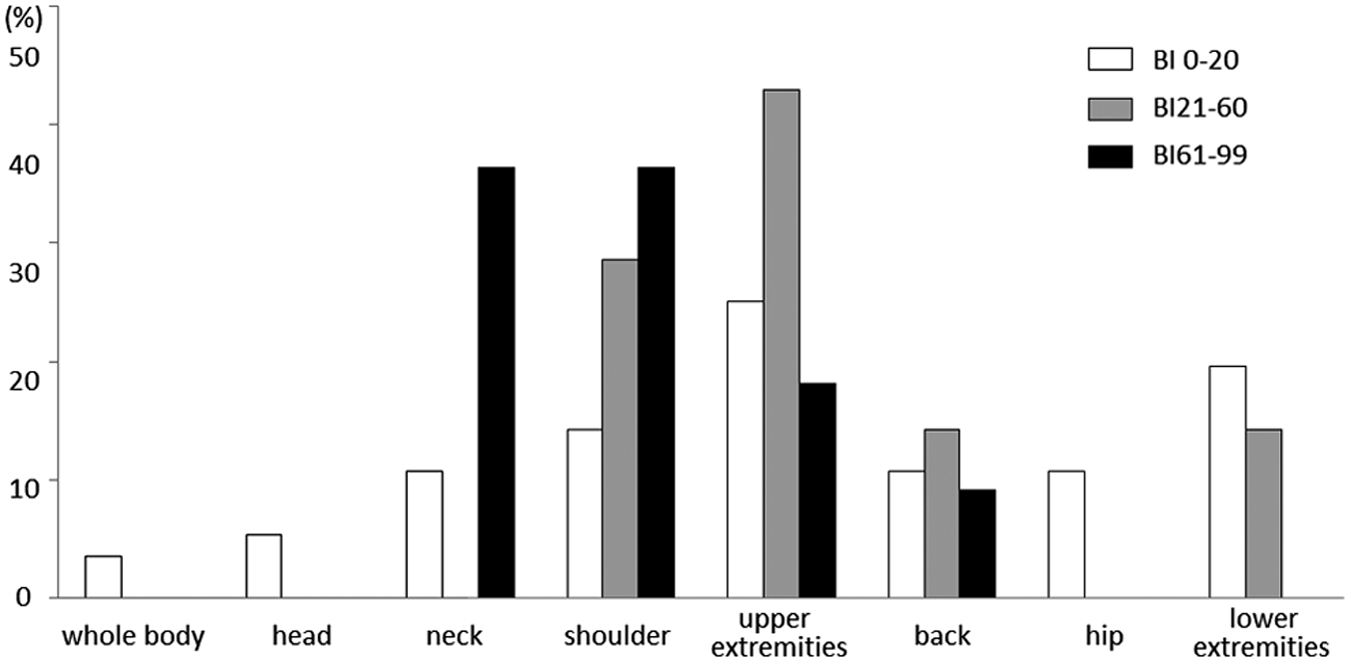
Pain distribution in patients with amyotrophic lateral sclerosis. BI, Barthel Index.
Data are shown as n (%). BI 61–99 is categorized as moderate dependence, BI 0–20 as total dependence, and BI 21–60 as severe dependence.
BI, Barthel Index.
Data are shown as the mean ± standard deviation.
Determined using Kruskal–Wallis test between the three groups. BI 61–99 is categorized as moderate dependence, BI 0–20 as total dependence, and BI 21–60 as severe dependence.
Statistically significant.
WBS, Wong-Baker Faces Pain Rating Scale.
Discussion
This study investigated pain in patients with ALS. Pain was reported by 53.8% of all patients, many of whom had a long disease duration and severe disability (43.8% had a disease duration >5 years, 55.0% were using a respirator, and 63.8% were being tube fed). Although more ALS patients with decreased functional status were included in this study than in previous reports, the frequency of pain in our patients was similar to the rate of 15%–85% previously reported in patients with ALS4–9 and consistent with the findings of studies in other severely impaired or terminally ill patients (57% 18 and 52% 19 ).
Twenty-nine patients (36.3%) with ALS used pharmacological treatments for pain, which is lower than the rate reported in other studies (54%, 6 74%, 20 and 77% 12 ). This discrepancy may be explained by differences in the frequency of pain and the fact that ALS patients with decreased functional status are very likely to be severely dysarthric and have difficulty reporting their pain. Opioids were the most widely used pain medications in this study, and were used alone or in combination with NSAIDs. Opioids would be expected to be a second-line option for pain in these patients because most of them had advanced disease, meaning that they also had respiratory insufficiency. However, a recent systematic review 14 highlighted the paucity of reliable efficacy data on pharmacological treatment of pain (including for opioids, NSAIDs, and adjuvant analgesics) in patients with ALS.
Although the results of some studies4,11,12 have suggested that pain in patients with ALS is correlated with progression of functional impairment, those of others6,21 have reported no correlation between pain frequency and disease progression. In this study, pain frequency was not associated with duration of ALS or ability to perform activities of daily living. However, a high proportion of patients who were totally dependent complained of moderate-to-severe pain. This result is consistent with that reported by Rivera et al. 21 It has been reported that the anatomic distribution of pain in patients with ALS involves the upper and lower extremities and the back4–6,8,21,22 or is more widespread. In our present study, patients who were totally dependent reported pain that was widely distributed throughout the body, whereas those who were only partially dependent with regard to activities of daily living reported pain that was localized to the upper body.
The main limitation of our study is its cross-sectional design, which precluded determination of the course of pain during the history of the disease, so there is a possibility that the correlation between pain and functional status was not evaluated accurately. However, the study was conducted at multiple centers, so we were able to avoid selection bias. Other limitations are that the study was observational, and no data were available on combination treatment; so, we could not remove the influence of treatment for pain. Therefore, longitudinal studies are needed to determine the influence of disease progression and pharmacological treatment on pain.
Our findings indicate that all patients with ALS are at risk of developing pain and that the intensity of this pain increases with decreasing functional status with or without treatment. Pain has been reported to be the most significant contributor to suffering in the final stages of ALS. 12 Moreover, patients with decreased functional status have difficulty communicating, so cannot report their pain. Therefore, we suggest that there is a need for aggressive pain monitoring and management in ALS patients with decreased functional status.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.