
Abstract
Abstract
Background:
There is little data on pain management in patients with advanced chronic kidney disease (CKD) who have opted for palliative care.
Objective:
We investigated the prevalence, severity and management of pain in advanced CKD patients attending Renal Palliative Care out-patient clinics under our Division.
Methods:
Consecutive patients referred to the Renal Palliative Care Clinics at two hospitals under our Division from July 2012 to June 2016 were included. All the patients were managed according to a multi-disciplinary protocol led by palliative care specialists, including serial assessments with the Edmonton Symptom Assessment System.
Measurements:
Response to pain management was defined as a difference by 2 points or more, and factors predictive of response were assessed by logistic regression.
Results:
Data from 253 patients were analyzed. Of them 107 patients (42%) experienced pain symptoms: 45 patients (42.1%) rated their pain as mild (score 0–3), 51 (47.7%) as moderate (NRS score 4–6), and 11 (10.2%) as severe (score 7–10) by using numerical rating scale. The response rate to pain management was 53.2%. Neuropathic pain was a predictor for lack of response.
Discussion:
Pain is common in advanced CKD patients receiving palliative care. While this seems to have been underrecognized, the symptom is potentially amenable to management. We recommend routine assessment of pain burden in this patient population.
Introduction
P
Methods
Consecutive patients who were referred to the Collaborated Renal Palliative Care (CRPC) clinic of Hong Kong West Cluster (HKWC) from June 2012 to May 2016 were analyzed. Inclusion criteria were as follows: (1) advanced CKD according to the Kidney Disease Outcome Quality Initiative (K/DOQI) guidelines 12 ; (2) opted for conservative treatment (“no dialysis or transplant” option chosen by patient himself/herself or decided by attending nephrologist); (3) patients who either have one-year life expectancy estimated by the referring physician or symptomatic renal failure 13 ; and (4) age older than 18 years. The study was approved by the Institutional Review Board of the University of Hong Kong/Hong Kong Hospital Authority West Cluster (IRB HKU/HKHAHKW).
Process of the palliative care service
The CRPC is provided by both the palliative care team and the nephrology team. 14 All members work as a team and provide mutual coverage when others are on leave so as to maintain service quality. This helps the team maintain a standard approach to management and communication with patients and their caregivers. Team members include a trained nephrology nurse, a palliative care nurse, and on-site social worker counseling services. 14 Other services such as home care, pastoral support, clinical psychology counseling, day care, inpatient care, physiotherapy, and physical therapy are consulted when needed. The care of all patients follows a standardized management plan. 15 Patients and their families are initially assessed by the registered nurse using tools such as the Edmonton Symptom Assessment System (ESAS) and Palliative Performance Scale (PPS) and psychosocial questionnaires. 14 The findings are discussed with a clinician, who then conducts an interview with the patient and the family and performs a physical examination. The physician and nurse then ask appropriate members of the interdisciplinary team to participate based on the patient's and family's individual needs. These interventions and care provided by the interdisciplinary team follow international guidelines.15–17
These guidelines focus on (1) assessing and managing pain and uremic symptoms18,19; (2) facilitating patients' and caregivers' understanding of the disease and treatment goals; and (3) providing assistance to the patient and their caregivers in coping with the life-threatening illness and in decision making. 20
Pharmacological interventions
The World Health Organization (WHO) three-step analgesic ladder guides initial treatment and escalation of pain medications and is validated in advanced CKD patients. 21 For mild pain, the advanced CKD patient should be treated by step 1 analgesics, including acetaminophen or nonsteroidal antiinflammatory drugs (NSAIDs). 22 The National Kidney Foundation suggests acetaminophen as the non-narcotic analgesic of choice or patients with CKD. NSAIDs might be used in patients with advanced CKD for time limited trials under close observation for side effects, including volume retention, hyperkalemia, gastrointestinal bleed, or deterioration of residual kidney function. 23 Step two is for mild pain not responsive to the mentioned agents or pain rated as moderate. These agents include weak opioids such as tramadol and low-dose opiates such as oxycodone (2.5–5 mg) or hydromorphone (1–2 mg). 24 The next step in escalation is step three agents for severe pain, including higher dose hydromorphone or oxycodone and long-acting medications such as fentanyl. The provider could consider referral to pain or palliative care specialists for the methadone use. 22 Adjuvant therapy might be helpful as opioid-sparing medications and is particularly indicated when treating neuropathic pain. Examples of these agents can include anticonvulsants and antidepressants.
Assessment of clinical data and symptoms
All patients included in this analysis completed the ESAS questionnaire 15 for at least the initial and follow-up visits within a range of 7 and 30 days of the initial visit.
The symptoms, including pain score, were assessed during each clinic visit. Patients were asked to score the maximum pain experienced during the previous one week on a 10-cm visual analog scale ranging from “no pain” to “unbearable pain” (0–3: mild pain, 4–6: moderate, and 7–10: intense). Patients were also asked to indicate the site and characteristics of pain. Duration of pain is defined as acute (recent onset), subacute (up to three months), and chronic (more than three months). 25 While more than one site of pain could be reported by patient, only the site with the worst score will be analyzed. Patients were also asked to complete the modified ESAS used in palliative care, as well as for dialysis patients, to assess the overall symptom burden. 15 The modified ESAS consists of eleven items (pain, fatigue, nausea, depression, anxiety, drowsiness, dyspnea, anorexia, insomnia, and feeling of well-being) and one patient-specific symptom. 16 Associated psychosocial factors were assessed by palliative care nurses, and the etiology and the pathophysiology of the pain were determined by the attending physician. Data on baseline functional status were also collected using PPS version 2, which is a version of the Karnofsky Performance Status scale. 26
Definition of response
Pain treatment response was defined as at least a two-point improvement on the ESAS pain item at the first follow-up visit. 17
Statistical analyses
Continuous variables are expressed as mean (standard deviation or SD) or median (range) and analyzed with t test (paired or unpaired), Mann-Whitney test, or analysis of variance where appropriate. Categorical variables were expressed as frequencies (percentages) and analyzed with chi-square test or Fisher's exact test where appropriate. Predictive factors for pain treatment response were assessed by univariate followed by multivariate analyses (for those variables with p < 0.1). All analyses were performed by the SPSS statistical package 22.0 (SPSS, Inc., Chicago, IL), and p value of <0.05 was considered statistically significant.
Results
Demographics
A total of 253 patients with advanced CKD opting for renal palliative care were included for analysis (Table 1). All these patients opted for conservative treatment and had never received dialysis or kidney transplantation. The median time for follow-up was 26.6 days (range 7–28 days). Of these patients, 107 patients experienced pain symptoms, whereas the other 146 patients did not experience pain. Among the 107 patients who reported pain, 45 (42.1%) rated their pain as mild (NRS score 0–3), 51 (47.7%) as moderate (score 4–6), and 11 (10.2%) as severe (score 7–10) by using numerical rating scale. Using ESAS as baseline assessment, the prevalence of pain is 42% in the first consultative visit. And 49%, 27%, and 24% of patients had chronic, subacute, and acute pain, respectively. The symptom scores of depressed mood in patients with pain were significantly higher than those without pain at baseline (p < 0.05) (Table 1).
Number with percentages of subtotal is used for categorical variables and mean with SD for numerical variable.
CKD, chronic kidney disease; ESAS, Edmonton Symptom Assessment Scale; NS, not significant; PPS, Palliative Performance Score 0–100% with 11 categories (0% = dead, 100% = totally independent); SD, standard deviation; SOB, shortness of breath.
Pain treatment response and changes in pain scores
The overall change in pain mean scores was reduced from baseline 4.5 (SD 1.9) to 2.3 (2.2) significantly (p < 0.05) at the first follow-up. For those with ESAS pain score ≥4, the mean score for pain was reduced from baseline 5.8 (SD 1.9) to 2.9 (2.5) (p = 0.007) at the follow-up visit (Table 2). Figure 1 showed the types and percentage of pain symptoms in the first consultative visit. Of the 62 patients, 33 (53.2%) met the criteria for pain treatment response (p < 0.001). Five (15%) responding patients still had an NRS score of ≥4 at the first follow-up visit. After multivariate analysis, only neuropathic pain remained a significant predictor for poor pain treatment response (odds ratio 3.8; 95% CI 1.8–8.3, p < 0.05). There was no relationship between sex, gender, anxiety, sleep, shortness of breath, nausea, well-being, anorexia, creatinine clearance, and PPS with pain treatment response (p > 0.05 for all) (Table 3).
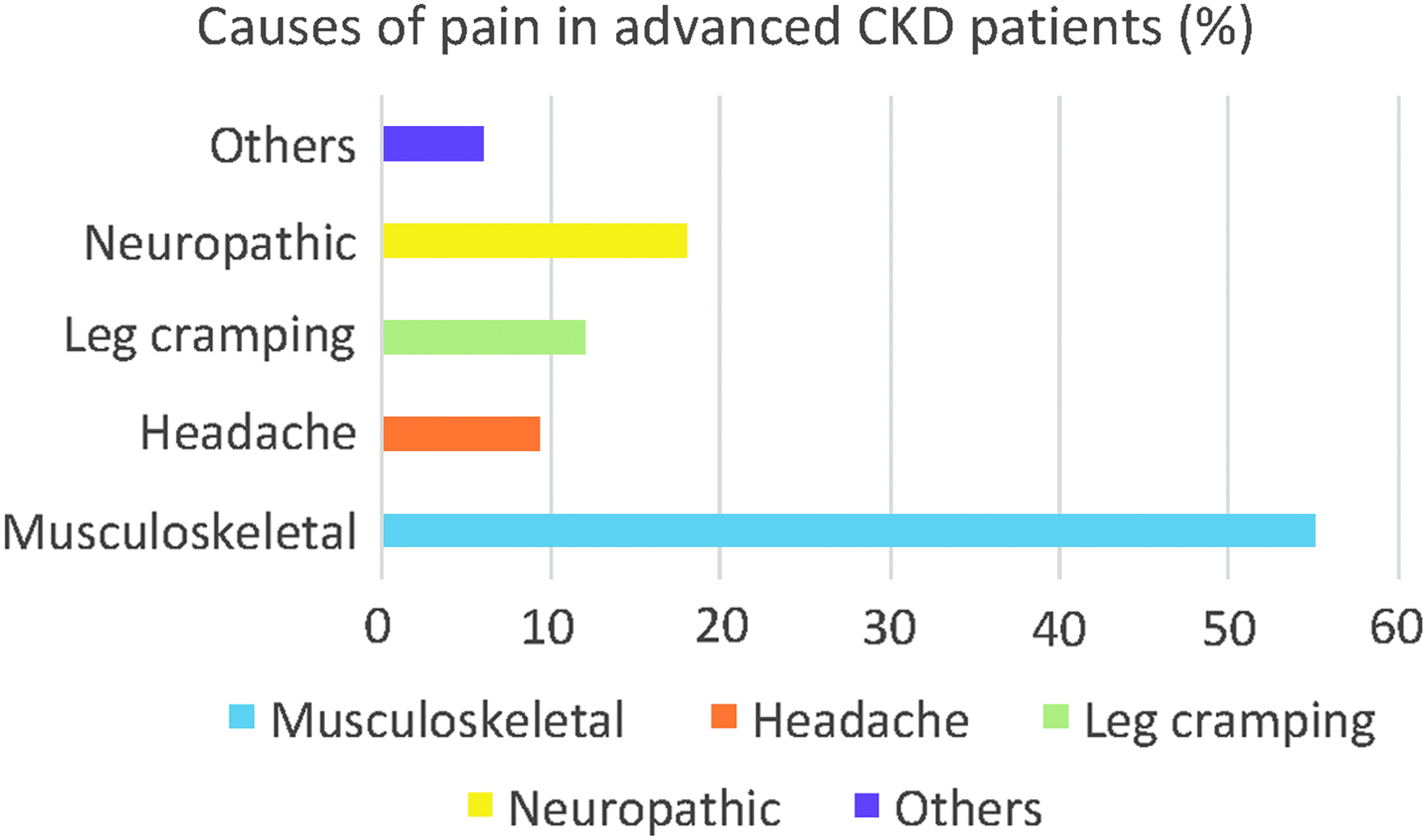
Causes of pain in advanced CKD patients. CKD, chronic kidney disease. Color image is available online at www.liebertpub.com/jpm
ESAS, Edmonton Symptom Assessment Scale; NRS, numerical rating scale.
No pain response = 1; pain response = 0.
p < 0.1 in univariate analysis; **p < 0.05 in multivariate analysis.
Use of pain medications for those with significant pain (ESAS pain score ≥4)
At T0, information on medication of all 62 patients was available from the health electronic system: 43.5% (n = 27) patients received regular acetaminophen; 2% on weak opioid (tramadol); and 11% on other alternatives (gabapentin/pregabalin/sodium valproate). Grouping of patients according to the WHO analgesic ladder is shown in Figure 2. During the baseline visit (T0), only 56.5% (n = 35) of patients received regularly scheduled analgesics, compared to 92% (n = 57) at their first follow-up visit (T1). Types and frequency of different analgesics used in our patients at T0 and T1 are shown in Figure 2. Only 3.2% (n = 2) patients required strong opioid at T1. Regular nonopioid (acetaminophen)/weak opioid was added in 18 (29%) out of 62 significant pain patients. In 3 (4.8%) patients, the opioid dosage was escalated. Anticonvulsants (gabapentin or pregabalin) were added in 6 (9.7%) patients. No patient has consumed NSAID in this study.
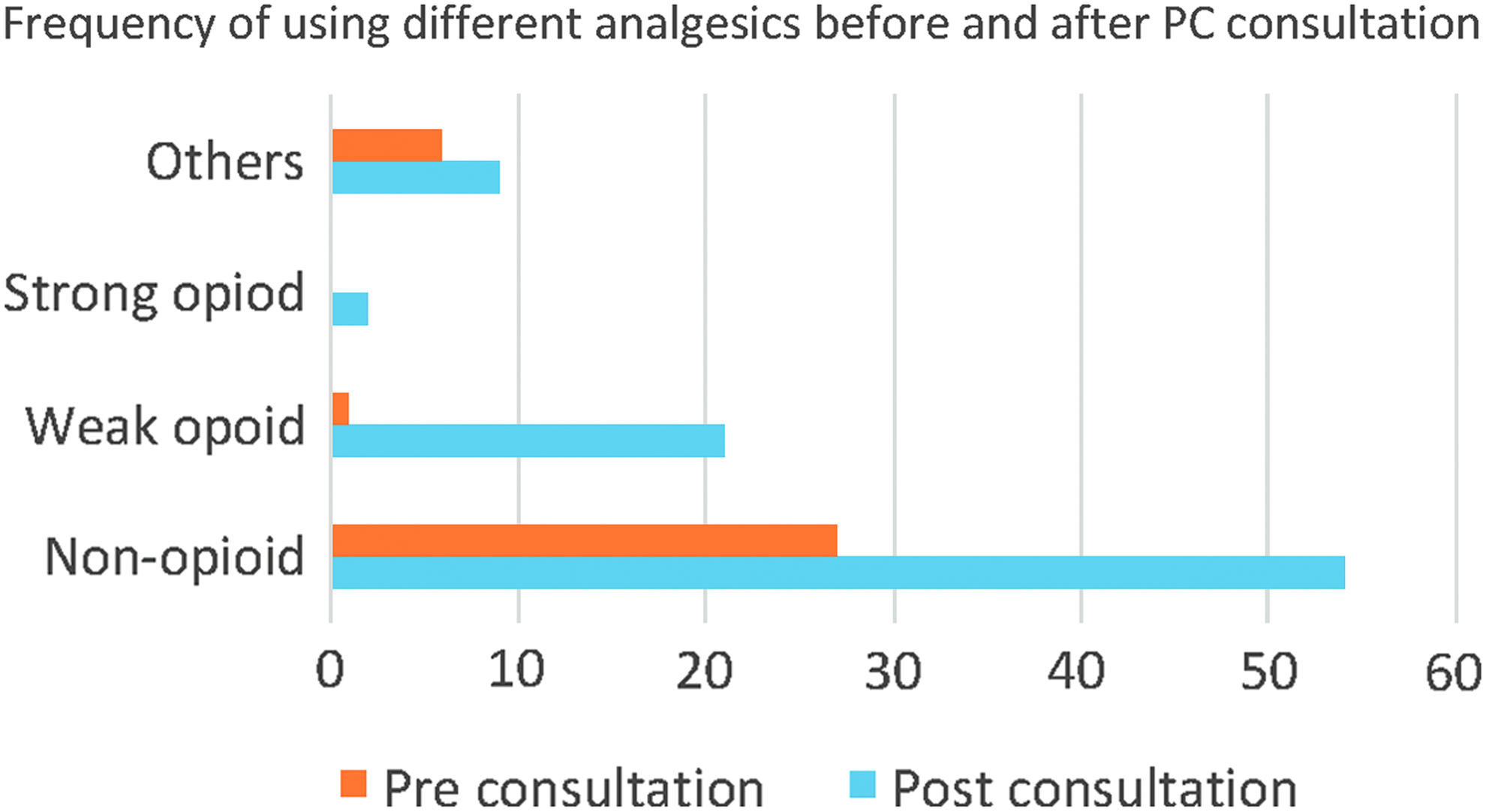
Use of different analgesics before and after renal PC consultation. PC, palliative care. Color image is available online at www.liebertpub.com/jpm
Discussion
Our current data suggested that a substantial proportion of advanced CKD patient who opted for renal palliative treatment suffered from pain symptoms, and >50% of them had moderate-to-severe pain on presentation. Such alarming clinical observations might be contributed by the low use of regular analgesics before their presentation to the renal PC clinic and such prescription practice might be related to the fear of toxicity and adverse reaction of analgesics in advanced CKD patients who were not on dialysis. In this context, the considerable variability in pharmacokinetics and pharmacodynamics of analgesics in advanced CKD patients who did not receive dialysis had resulted in paucity of data to support their dosing recommendations. Therefore, dosing of analgesic in advanced CKD patient who opted for conservative management should be individualized, and vigilant monitoring of treatment efficacy and side effects (by phone calls, home visits, and clinic follow-ups) should be carefully exercised.
Our results also suggested a benefit of collaborative renal palliative care on pain management in advanced CKD patients who opted for conservative management. In this study, we observed significant reduction in pain scores, especially in patients who had moderate-to-severe pain on presentation. In this cohort, the pain response was similar to cancer patients who required palliative care (53.2% vs. 45%). 27 Despite a decrease in pain scores, it was notable that the overall pain response was relatively modest as only half of the patients showed treatment response, and significant pain burden still exists in 15% of those who showed treatment response. In this cohort, the presence of neuropathic pain was a significant risk factor for poor response to pain treatment. In fact, renal failure patients often present with wide spectrum of pain syndromes, and delineation of contributions of these pain syndromes would potentially help optimize pain control. Furthermore, the current pain management guidelines might not have adequately addressed advanced CKD patients, and the effect of pain treatment could also be limited by renal dose adjustment and side effects of current analgesics.
Clear guidelines for pain management in advanced CKD patients opted for palliative care are warranted to avoid underprescription of analgesics. Whether the modulation of inflammation or increase in the follow-up frequency (dose and intensity of palliative care visit) will improve pain treatment response in advanced CKD would be worthwhile directions of future research in pain management among renal failure patients.28–30
The strength of this study includes the longitudinal data on pain assessment both at the initial and subsequent follow-up visits, using validated tools in the outpatient Renal Palliative Care Center. 15 Pain assessment was completed by the patients under supervision of nurses trained specifically in palliative care, and standardized management was provided by a specialist-led palliative care team in accordance with our institutional protocol, based on the findings from these pain assessments. 15 Thus, our results represented accurate and realistic reference data regarding the effectiveness of outpatient renal palliative care when standard palliative care is applied to advanced CKD patients with different causes of pain syndrome.
One important limitation of this study is the lack of a control patient group receiving care from a usual nephrology clinic. Our collaborative renal palliative care service, with frequent follow-up visits, used a multidisciplinary approach for pain management, and thus, the data might not be applicable to patients who have not received renal palliative care similar to our model. Being retrospective in nature, there are missing data on the prevalence of incidental pain and the mean dose of opioid, which are both recognized risk factors for pain control. Last but not the least, only a single assessment tool (ESAS pain item) was used to gauge pain intensity, and more comprehensive tools such as the Brief Pain Inventory or other multidimensional instruments should be adopted to complement the ESAS for pain assessment in future prospective studies.
Conclusions
Pain burden remains substantial in advanced CKD patients who opted for palliative care, and the response to treatment was suboptimal. Neuropathic pain is a significant risk factor for poor response to pain treatment. While our retrospective data suggest that collaborative renal palliative care approach might help alleviate pain symptoms in advanced CKD patients who opted for conservative management, further prospective controlled studies are required to demonstrate its effectiveness and impact on clinical outcomes.
Footnotes
Acknowledgments
This study received no funding.
Author Disclosure Statement
The authors declare no conflicts of interest.