
Abstract
Abstract
Background:
Little is known about how decision-making conversations occur during pediatric intensive care unit (PICU) family conferences (FCs).
Objective:
Describe the decision-making process and implementation of shared decision making (SDM) during PICU FCs.
Design:
Observational study.
Setting/Subjects:
University-based tertiary care PICU, including 31 parents and 94 PICU healthcare professionals involved in FCs.
Measurements:
We recorded, transcribed, and analyzed 14 PICU FCs involving decision-making discussions. We used a modified grounded theory and content analysis approach to explore the use of traditionally described stages of decision making (DM) (information exchange, deliberation, and determining a plan). We also identified the presence or absence of predefined SDM elements.
Results:
DM involved the following modified stages: information exchange; information-oriented deliberation; plan-oriented deliberation; and determining a plan. Conversations progressed through stages in a nonlinear manner. For the main decision discussed, all conferences included a presentation of the clinical issues, treatment alternatives, and uncertainty. A minority of FCs included assessing the family's understanding (21%), assessing the family's need for input from others (28%), exploring the family's desired decision-making role (35%), and eliciting the family's opinion (42%).
Conclusions:
In the FCs studied, we found that DM is a nonlinear process. We also found that several SDM elements that could provide information about parents' perspectives and needs did not always occur, identifying areas for process improvement.
Introduction
Q
The components of healthcare DM, analysis and judgement, 2 are often depicted in three stages: (1) information exchange; (2) deliberation; and (3) plan determination.3,4 Three prevailing models describe how these stages are operationalized: (1) paternalistic DM (emphasizing physician authority); (2) “autonomous”/informed DM (emphasizing patient/family authority); and (3) shared DM (emphasizing shared authority reflecting patient/family preferences).3–5 Experts endorse shared decision making (SDM) for preference-sensitive healthcare decisions. 6 Recommendations for implementing SDM involve introducing choice, describing options, and making a decision. 7
Family conferences (FCs) are commonly used when clinicians discuss difficult decisions with patients and their families, especially in intensive care units.8–12 FCs help bring families and patients together with healthcare team members (HTMs). Effectively conducted FCs for critically ill adult patients can improve family understanding, increase satisfaction, and lessen the burden of caregiver bereavement when patients die.13–15 While many studies about FC decision-making conversations for adult patients exist,11,13–18 the literature about PICU FCs is less robust.19–23
This report provides information about decision-making conversations using a subset of data from a PICU FC study. 23 This analysis focuses on FCs involving DM discussions. We explored if and how decision-making conversations integrated the three DM stages described above (information exchange; deliberation; and plan determination), and if they included previously defined SDM elements. 16
Methods
Setting
This study took place at a university-based, tertiary care PICU from January 1, 2011 to January 1, 2012, a timeframe determined a priori. 23 Patients in the 42-bed “closed” PICU (the attending for all patients was a pediatric intensivist) included medical and surgical (general or cardiac) patients. The PICU teams included an attending, PICU fellow, and pediatric residents or PICU advance practice nurses (APNs) and subspecialists. The project was approved by the hospital's Institutional Review Board.
Identifying FCs
We defined FCs as planned meetings involving parents, HTMs (e.g., physicians, APNs, nurses, social workers, chaplains), and when present, non-HTMs providing parent support (e.g., family or friends). 23 We did not include impromptu parent updates, one-on-one bedside conversations, or discussions held during daily family-centered rounds. We identified FCs by weekday chart review and communication with the medical team. We included only weekday FCs secondary to staffing limitations. We excluded conferences when any participant did not provide written consent or did not speak English or Spanish. Further details have been described previously. 23
Data collection
We audio and video recorded FCs using unobtrusive recording devices managed by a study team member present during the meeting. Some conferences were only audio recorded at participants' requests. The study team member identified the FC “leader” as the person moderating the FC. After the conference, parents and HTMs completed a written questionnaire requesting demographics. 23 We collected patient information via medical chart review. The audio recordings were transcribed verbatim and de-identified. For FCs with Spanish speakers involving an interpreter, only English dialogue was transcribed. We did not analyze video data because our focus was on dialogue, not behaviors.
Data analysis
Identifying FCs, including DM discussions
Three reviewers (K.M., N.H.B., and C.R.) reviewed the transcripts and ascribed goals to each FC based on previously described FC goals. 24 Ascribed goals were compared and discrepancies resolved by consensus. Goal categories included medical update (medical information regarding patient status), care planning (future medical plans during the hospitalization or discharge planning), and DM (patient care decisions). 23 In this analysis, we include FCs with DM as an ascribed goal.
Qualitative analysis of FC transcripts
We combined the inductive process of grounded theory with content analysis. 25 Two authors (K.M. and M.S.) read and labeled the transcripts identifying themes, concepts, and patterns to understand the conversation content and flow. Using these labels, we created a preliminary coding dictionary. We reread the transcripts to identify excerpts (a sentence or contiguous-related sentences) that conveyed similar content. We tagged the excerpts with the preliminary codes or created new codes as needed. We achieved saturation (no new codes created) by the third transcript. With our final coding dictionary, two researchers (M.S. and M.A.) separately assigned codes to the excerpts. Agreement between the two coders within a transcript ranged from 67% to 84% (average: 75.64%). Discrepancies between the coders were discussed and resolved through consensus. Excerpts were categorized as either spoken by a HTM or a parent. Family members and support individuals spoke infrequently and thus were grouped with parents (hereafter, “parents” refers to parents, family, or support individuals).
After coding each FC transcript, two authors (M.S. and K.M.) organized codes into themes and then grouped the themes into categories corresponding to previously defined decision-making stages—information exchange, deliberation, and determining a plan. 3 We created new categories if themes did not clearly fit into one of these predefined stages. We present the final categories as DM stages in the results below. To analyze the flow of conversation between stages, we color-highlighted the excerpts according to their coded decision-making stage. This provided a visual representation of how HTMs and parents navigated through the decision-making stages. We used Dedoose (Dedoose Version 5.2.0 (2014). Los Angeles, CA: SocioCultural Research Consultants, LLC [www.dedoose.com]) for qualitative analysis.
Quantitative analysis of FC transcripts
We modified a previously validated measure of SDM elements. 16 Two reviewers (C.R. and N.H.B.) separately reviewed parts of the transcripts that focused on the main decision discussed (as determined by consensus between the two reviewers), and noted the presence or absence of each SDM element. Initial agreement between the two coders ranged from 50% to 100% per conference (average: 81.82%). Discrepancies were resolved through consensus, or by a third reviewer (K.M.) in cases without consensus.
General quantitative analysis
We present quantitative information with descriptive statistics analyzed with Microsoft Excel (Microsoft Office 2013, version 15.0.4937.1000).
Results
We recorded 23 of the 39 FCs for which participation was requested (59%). Technical problems prohibited use of one FC recording. We reviewed transcripts from 22 FCs discussing 20 patients. Of the 22 transcripts analyzed, 14 involved DM discussions. The eight excluded conferences involved medical update and care planning discussions. (Fig. 1) Decisions included the following: introducing palliative care; withdrawal of life-sustaining therapies; “do not resuscitate” orders; agreeing to a new surgical or medical therapy; placement of a tracheostomy or gastrostomy tube; use of chronic noninvasive positive airway pressure ventilation; transfer to a chronic care facility; and initiation of long-term ventilation. 23 Some FCs involved discussions about multiple decisions.

Family conference inclusion process.
Of the 14 analyzed FCs, 11 were video and audio recorded, and 3 were only audio recorded. Five FCs involved a Spanish-language interpreter. The FCs lasted an average of 48 minutes (median 45.5 minutes, range 13–93 minutes) and occurred, on average, 45.4 days after PICU admission (median 30.0 days, range 3–172 days). On average, 6.8 HTMs (median 6.5, range 4–10) attended the FCs. FCs were led by a PICU fellow or attending physician (n = 5, 36%) or by a pulmonary (n = 6, 43%), cardiology (n = 1, 7%), neurology (n = 1, 7%), or hematology/oncology (n = 1, 7%) subspecialist. The FCs included 25 parents. Eleven FCs included two parents and four included at least one family support person. Table 1 shows the demographic data for the 20 parents (involved in 10 FCs) who completed a postconference questionnaire. Table 2 provides patient demographics and clinical characteristics.
Missing data from five parents involved in four conferences.
Could have been given FiO2 via NC or mask.
one patient had active withdrawal of life-sustaining therapies; one died despite continuing all therapies.
CPR, cardiopulmonary resuscitation; DNAR, do no attempt resuscitation; ECMO, extracorporeal membrane oxygenation; FC, family conference; GT, gastrostomy tube; PC, palliative care; PICU, pediatric intensive care unit.
Qualitative analysis of FCs
Figure 2 depicts our DM stages and associated themes. Discussion with codes pertaining to deliberation seemed inherently linked to either information exchange—understanding the details of the decision and their impact on the patient—or determining a plan—defining the plan and how to operationalize a decision. Therefore, we redefined the DM stages as information exchange; information-oriented deliberation; plan-oriented deliberation; and determining a plan. Table 3 presents these stages, the themes within each stage, the codes assigned to each theme, and example quotes from parents and HTMs. Below, we elaborate on the DM stages and themes.
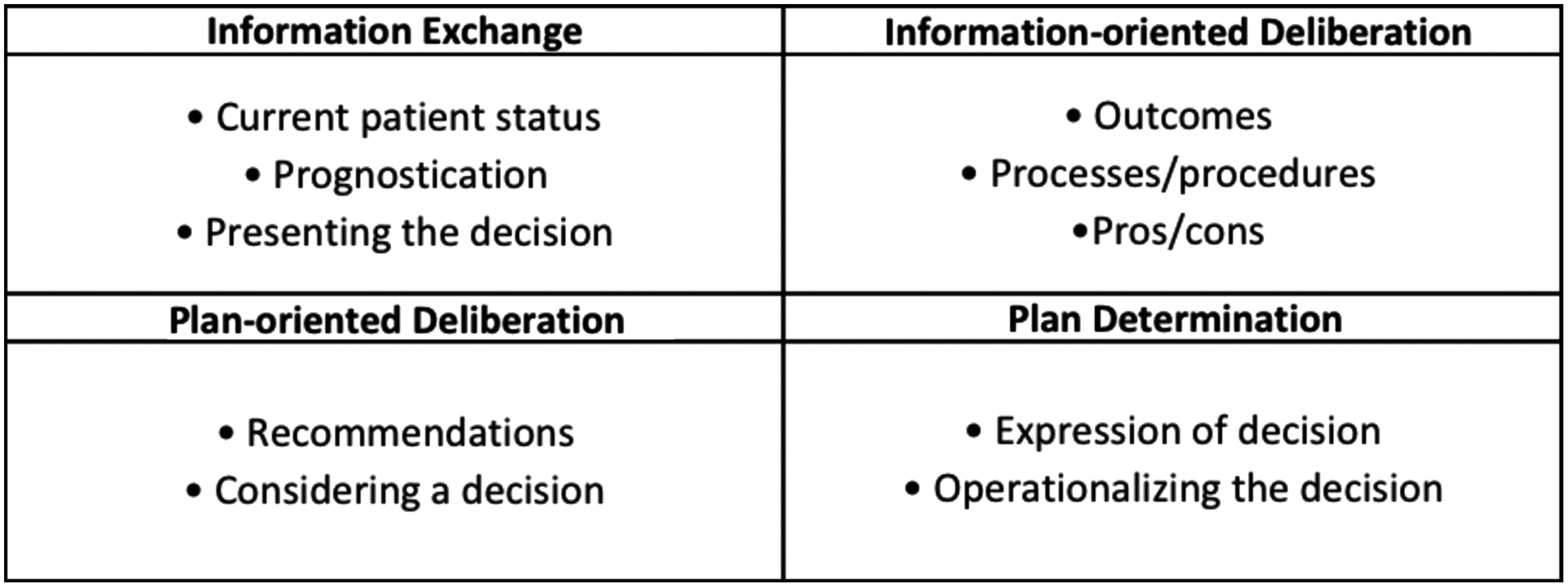
Decision-making stages and associated themes.
Stages of decision making are bolded, the themes within each stage are underlined, and the codes assigned to each theme are indented.
ADA, Americans with Disabilities Act; CPAP, continuous positive airway pressure; DNR, do not resuscitate; HTMs, healthcare team members.
Information exchange
The information exchange stage included discussions about the patient's status, comments about prognosis based on the patient's current situation, and a presentation of decisions. HTMs always discussed the reason for the FC and provided information about the patient's current status. Parents always discussed their perceptions of the patient's current condition. HTMs and parents both asked questions about the patients' current medical situation in the majority of FCs. In about half of the FCs, parents asked about the patients' prognoses. HTMs provided prognosis information more often than it was asked for. In all FCs, HTMs used a transition or introduction to conversations about a decision, and this often involved HTMs describing why a decision needed to be addressed. In all conferences HTMs talked about the different options available.
Information-oriented deliberation
The information-oriented deliberation stage described conversation involving information about the patient and decisions that helped parents and HTMs deliberate. It included three themes: potential decision outcomes; details about processes/procedures relevant to the decision; and the pros/cons of different choices. Almost all conferences included discussion from HTMs about known, unknown, and predicted outcomes. Most HTM statements involved details about processes and procedures related to a decision, including explaining pros and cons. In contrast, most parent speech involved asking questions. Although fewer questions came from HTMs, typically this was a HTM asking a question of another HTM.
Plan-oriented deliberation
Themes in the plan-oriented deliberation stage included recommendations and considering a decision. Although asked for by parents explicitly in less than half of the FCs, HTMs provided recommendations in most FCs. The recommendations were typically explicit and directive. However, providers often also made “subtle” recommendations, using indirect language without explicitly endorsing a course of action (e.g., “… if you choose to have her on the machine 24/7 … that would be pretty uncomfortable in the long run”). In a few instances, HTMs used language to avoid or defer making a recommendation. Also included in this plan-oriented deliberation stage were comments justifying a decision. Following such comments were statements weighing the presented options, thus we considered them related to the deliberation process.
Determining a plan
Plan determination included two themes, making and operationalizing the decision. A final decision was made in most, but not all, FCs. Most dialogues during this stage focused on operationalizing decisions and discussing the plan—when and how care would be provided to the patient. Operationalizing decisions also often included a discussion of support needs (social, structural, or financial) following hospital discharge or death.
Conversation flow
We found that conversations rarely flowed in a linear manner through the four decision-making stages. Figure 3 depicts an example portion of text with excerpts labeled according to their coded decision-making stage. This example was typical of how discussions flowed unpredictably between all the stages, with physicians and parents frequently working through different stages multiple times.
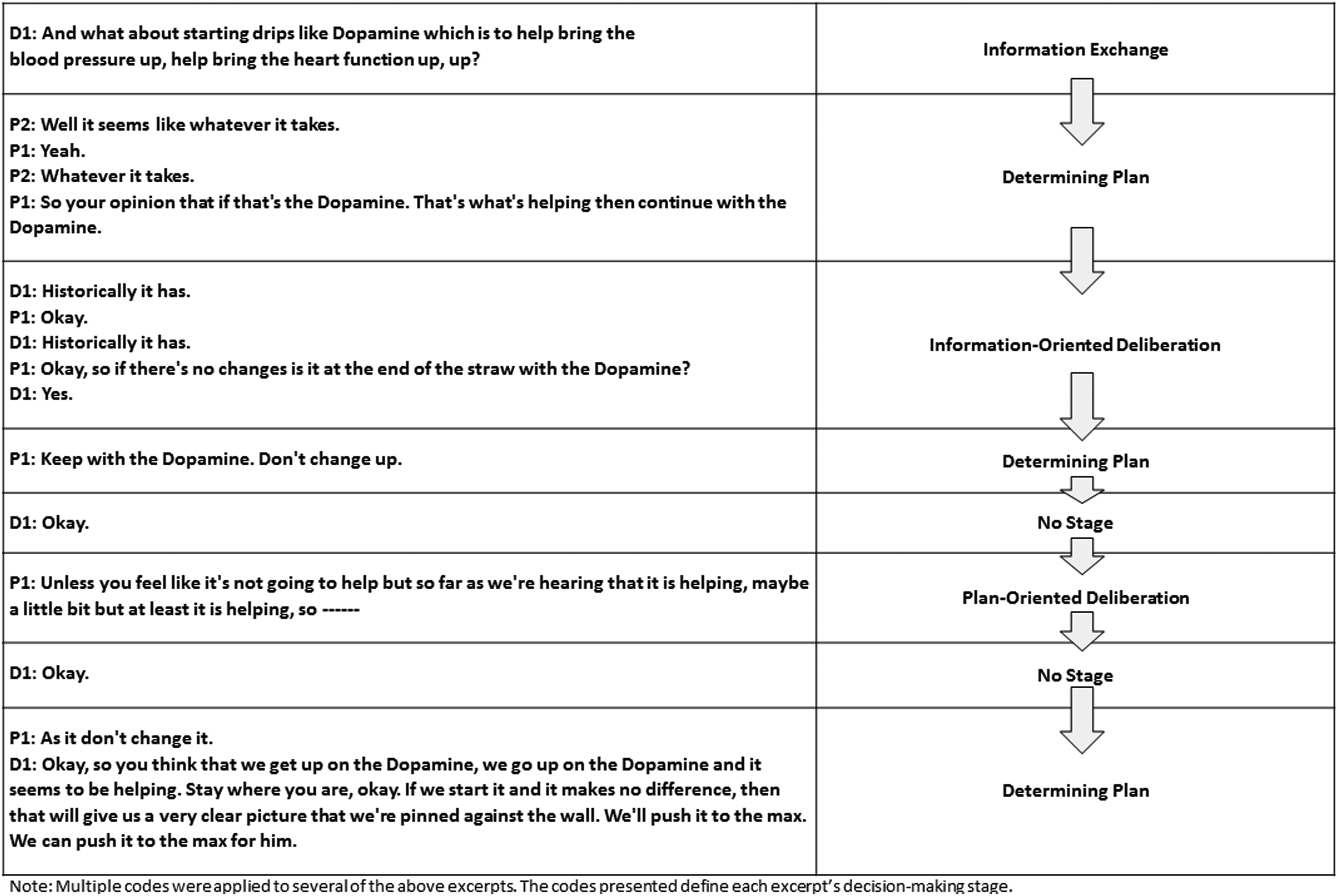
Example conversation with excerpts labeled by decision-making stage. This example highlights the unpredictable flow of conversation through the different stages of decision making.
Results from quantitative analysis of FCs
Table 4 shows the 11 SDM elements adapted from previous work 16 and the percentage of conferences, in which each activity occurred. The number of elements present in the FCs ranged from 4 to 10 with an average of 6.9.
Only assessed in five conferences involving patients for whom preferences might be known or obtainable.
Discussion
This study provides insight into the content and flow of DM conversations during PICU FCs. We found that deliberation was integrated into information exchange and plan-making discussions. In these FCs, HTMs infrequently obtained information about parents' perspectives about decisions discussed, missing important SDM elements. We also found DM to be a nonlinear process that flows unpredictably between the decision-making stages. In the nonlinear flow of DM, we describe echoes reflections of other researchers—that SDM is dynamic, provisional, and iterative.26–28 Our results demonstrate the complexity of these discussions and highlight the need for HTM patience and flexibility with communication during FCs.
Our results also highlight important aspects of the approach to and content of DM discussions. For example, how HTMs made recommendations was notable. While, many providers made direct recommendations, some providers used less explicit, indirect language. In a few instances providers failed to make any recommendation. Admittedly, HTMs may feel more or less comfortable providing recommendations, depending on the type of decision discussed or the degree of uncertainty associated with a decision. Where uncertainty is high, providers might feel less comfortable providing a recommendation. The latest policy statement on SDM from the American College of Critical Care Medicine and American Thoracic Society states that many critically ill patients and their surrogates prefer to make decisions after considering HTM recommendations, even in “value-laden” decision-making scenarios. 6 This suggests that clinicians should make direct recommendations. However, in one study, White et al. showed that 42% of ICU surrogates preferred not to receive recommendations regarding the continuation of life support. 29 Perhaps HTMs should ask patients/surrogates about their preferences regarding clinician recommendations. Acknowledging differences in surrogate preferences about how or if HTMs provide a direct recommendation accords with the SDM approach. We cannot determine if the HTMs' approach to providing recommendations matched parent preferences in the FCs studied. Such questions could be considered in future research.
We found that assessing parental understanding occurred throughout most FCs. In this study, we did not explore how such understanding was obtained, for example, whether HTMs accepted a “yes/no” response to questions about understanding or if they requested that parents describe the issues and situation in their own words. In looking for the presence of SDM elements, we found assessing family understanding present in only 21% of discussions related to the main decision considered. This suggests that while assessing understanding may occur throughout FCs, it may not occur regularly for all decisions discussed. Further work into the process of assessing family understanding is warranted.
Finally, our analysis of SDM elements present or absent in these conferences identifies potential areas for improvement. Less frequently occurring SDM elements included assessing family understanding of decisions, asking families if input from others would help them make decisions, exploring the family's preferred DM role, and eliciting the family's opinion about a decision. Addressing each of those elements may not always have been warranted. For example, perhaps HTMs wanted to introduce a decision, but did not necessarily need to determine a final choice, obviating the need to elicit a family's preference. However, these less frequent SDM elements represent efforts to obtain information from families. That these elements occurred inconsistently in the FCs suggest that HTMs might consider directing more effort toward encouraging families to share their views, perspectives, and needs.
This study has a number of strengths. We analyzed actual FCs, not simulated FCs or comments provided retrospectively about FCs. Conferences were convened to discuss patients with a broad range of medical conditions and decision topics and were not focused on one particular kind of decision, allowing us to learn about discussions related to a range of DM challenges. Parent participants represented people from mixed racial, ethnic, and educational backgrounds. We included Spanish speakers and enrolled a high proportion (45%) of fathers.
We acknowledge some limitations. First, FCs represent one component of a complex decision-making process that also involves family-centered rounds, bedside conversations, input from family and friends, previous experiences, and so on. Second, we analyzed a relatively small number of conferences, limiting generalizability. The small sample also obviates our ability to statistically analyze associations between SDM elements, types of decisions, and parent/HTM outcomes as well as to explore other interesting areas within FC communication, particularly the role of supportive statements and emotion in FCs. The small sample partly reflects our refusal rate of 41%. Third, we analyzed audio data and do not comment on the impact of body language. Fourth, we acknowledge our somewhat low initial interrater agreement rates for the content analysis coding and coding of SDM elements, as low as 67% and 50%, respectively, in some FCs. To ensure the validity of our results, all coding discrepancies were resolved among the group. Finally, recording FCs and having a study team member present during the FCs may have influenced the conversations, although we feel this is unlikely based on similar work.30–32
Conclusions
We found decision-making discussions during PICU FCs nonlinear with deliberation integrated into information exchange and plan-making conversation. SDM elements meant to obtain parents' perspectives were not always present. We highlight needed areas of study related to concordance of HTM recommendations with family preferences for such information, approaches to assessing parent understanding, use of supportive language during FCs, and the relationship between SDM elements and parent/HTM outcomes.
Footnotes
Acknowledgment
This work was supported by a grant from The National Palliative Care Research Center (NPCRC) entitled, “Evaluating Family Conferences in the Pediatric Intensive Care Unit.”
Author Disclosures Statement
No competing financial interests exist.