
Abstract
Abstract
Background:
Patient-reported outcome (PRO) measurement is crucial to assess the benefit of psychotherapeutic interventions. Is repeated assessment of psychometric self-report data possible, as inpatient palliative care patients suffer from physical and psychological symptoms? What is the self-perceived strain caused by the assessment?
Objective
The main objective of this study was to investigate the feasibility of a repeated comprehensive psychometric self-assessment of inpatient palliative care patients. Secondary objectives were the PROs of the psychometric assessment.
Design:
We conducted a prospective cohort study. Patients admitted to our palliative care unit (PCU) were reviewed for eligibility within 72 hours. They were asked for weekly self-reports regarding hope (HHI-D), well-being (FACIT-Sp), anxiety and depression (STADI), and quality of life (QoL; EORTC-QLQ-C-30 single item). The strain caused by the assessment was assessed by a numeric rating scale (0–10) and free comments.
Results:
Within 11 months, 219 patients were admitted to the PCU. In total, 92 patients were eligible. The most frequent exclusion criterion was “life expectancy <1 week.” A total of 60 patients participated at the first point of measurement. The mean of self-perceived strain (Likert scale 0–10) due to the assessment was 1.44 (SD 1.99) at T1. Twenty-four patients participated twice. Here we found increased scores for physical well-being and QoL.
Conclusion:
Repeated assessment of psychological conditions is feasible for 27.4% of inpatients at a German PCU. The most limiting factor is life expectancy of only days at admission to the PCU. However, the self-perceived strain is low.
Introduction
S
Psychometric tests are an economic method for assessing subjective components of psychological phenomena. But, is this also true for patients approaching the end of life at a palliative care unit (PCU)? Are they cognitively, emotionally, and also regarding time requirements able and willing to repeatedly report their symptoms?
Limiting factors for research with PCU patients are their vulnerable health condition, usually short stays6,7 and ethical challenges. 8 Nevertheless, palliative patients self-report positive effects of study participation.9,10
Investigating the feasibility of repeated psychometric measurement using self-reports is required for decisions on conducting further intervention studies, for example, to design protocols that anticipate and manage changing clinical conditions, cohort mortality, attrition, and missing data.11,12
The aim of this study was to investigate the feasibility of a repeated comprehensive psychometric self-report package of inpatients in palliative care. Secondary outcomes were the PROs of the psychometric assessment.
Materials and Methods
The study was conducted with the agreement of the local ethics committee.
Sample
The study was conducted at the PCU of the University Hospital Mainz, Germany, caring for about 200 patients per year. It was planned to approach patients until 60 patients could be included within 12 months as this would lead to a 95% confidence interval with 90% coverage and half width of maximally 14% for the proportion of patients, who may repeat the assessment. Eligibility criteria included estimated life expectancy ≤12 months, age ≥18 years, and ability to give informed consent. Patients without fluency in German and cognitive impairment or a clinical estimation of life expectancy of less than one week (both assessed by the treating physicians) were excluded.
Patients were screened for inclusion within three days after admission to the PCU and gave informed consent. Patients could read and fill out the questionnaires on their own or ask for assistance. If patients were eligible and willing, measurement was repeated every seventh day.
Instruments
The HHI-D is the validated German version of the Herth Hope Index.13–15 The FACIT-Sp has been designed to measure spiritual well-being, based on the FACIT measurement system.16,17 Item 30 out of the EORTC QLQ C-30 was added to rate the overall quality of life (QoL) on a 7-point Likert scale. 18 The STADI 19 measures anxiety and depression on state and/or trait level. We focused on the trait part to discriminate changes over time from the patient's current state. In agreement with the test authors, the test instruction was adapted from indicating what applies to the patients in general regarding the item contents to indicate what applies to them since getting the diagnosis. The subjective assessment of strain was evaluated on an NRS from 0 = no strain to 10 = maximum strain, complemented by free comments on what was straining and what was helpful. This tool was used by our group and others in former studies, although not validated.20,21
Data analysis
We computed exact 95% confidence intervals for the recruiting probability and for the proportion of recruited patients participating in a second assessment. The first confidence interval was obtained using the negative binomial distribution, 22 the second was obtained using the Clopper–Pearson method. To estimate possible changes across measurement points, we calculated dependent samples t-tests regarding hope (HHI), spiritual well-being (FACIT-Sp), anxiety and depression (STADI), and QoL (EORTC QLQ C-30) with the respective scores at T1 and T2. At T3 and further measurements points, the remaining sample was too small for further analyses. Statistical analyses were performed using IBM SPSS Statistics 22, R 3.3.1 and SAS 9.4. Quantitative data of the perceived strain caused by the assessment are described by mean, standard deviation, range, and number of available cases for each point of measurement. Missing values for HHI-D, STADI, and FACIT-Sp subscales were replaced by mean if >50% of the items were answered; other cases were excluded. Free comments were analyzed according to qualitative content analysis by Mayring. 23
Results
Sample
Consecutive recruitment was carried out for 11 months. In total 219 patients were admitted to the PCU. The mean age was 70 years (range 20–95), 99 patients (45%) were female, and 90.4% had a primary diagnosis of cancer. Further subject characteristics are presented in Table 1. In total 92 patients (42%) were eligible. Sixty patients (27.4%) agreed to participate at T1. Out of the T1 participants, 28 (46.7%) also participated at T2 (+7 days). Figure 1 provides a complete overview of drop-out reasons. Fifty-nine of the 60 (98.3%) participants had cancer; 29 were female and mean age was 65 years (range 37–89). Characteristics for participants at T1 are listed in Table 2.

Flow-chart for study participation.
N = 218, time of first diagnosis unknown for one patient.
ECOG, performance status of the Eastern Cooperative Oncology Group; PPS, palliative performance status; PCU, palliative care unit.
N = 218, time of first diagnosis unknown for one patient.
Feasibility
A total of 219 patients had to be screened to recruit 60 patients, of whom 28 participated at least twice. This corresponds to an estimated recruiting probability of 27.4% (95% CI [21.6–33.5]) and an estimated probability for repeating the assessment of 46.7% (95% CI [33.7–60.0]).
Patient reported outcome measurements (PROs)
Descriptive data for PROs at the first two points of measurement are shown in Table 3. For HHI, FACT-G, FACIT-Sp, and single item EORTC QLQ C-30, higher scores indicate better outcome, that is, better expression of hope, functional capability, spiritual well-being, and QoL. Higher scores for STADI trait depression/anxiety indicate higher manifestations of these constructs. Results of dependent samples t-tests for T1 and T2 are shown in Table 4. The correlation for QoL and physical well-being at T1 (Person's r): r(54) = 0.31 reached a significant level (p = 0.02). No significant correlation was found for T2.
Strain caused by assessment
The mean duration of the assessment at T1 was 23 minutes (10–50 minutes). The mean strain caused by assessment (Table 5) was 1.44 (SD = 1.99) at T1 and 2.3 (SD = 2.49) at T2 without significant difference (t[22] = −1.75; p = 0.09). Nine patients showed strain ≥5 at T1. Three of them participated at T2, four died before T2, one declined because of high physical strain and one did not want to be strained by the survey.
One point: Organizational loss (Perceived strain caused by assessment t1: 0).
Ten-point Likert scale (0 = no strain at all; 10 = maximal strain imaginable).
Further details about strain over time are shown in Table 5. Patients reported four main categories of burden: concentration and understanding of the questions (cognitive), thinking about the topics (emotional), physical uncomfortableness, and the desire to fulfill the study task correctly.
Discussion
Repeated measurements using psychometric self-reports with inpatient palliative care patients seem to be feasible. In accordance with former studies, poor health status (life expectancy of less than one week and cognitive impairments) was the main limiting factor to recruit patients for research at a PCU.11,12 However, 65% of the eligible patients and 27.5% of the admitted patients, respectively, were willing to be enrolled in the assessment. This should be encouraging to schedule future intervention studies, in particular because the self-perceived strain was rather low in most patients. Furthermore, participants agreed that the assessment might also have been personally helpful for them. This finding is in accordance with previous results9,10 and with the psychological approach that every assessment might itself be an intervention.
Four of the 58 participants (7%) of the first assessment had to be excluded because they either discontinued the assessment or it remained ambiguous, whether the patient had fully understood the items. This sort of attrition has to be taken into account when calculating the number of cases for a study at the PCU.
Limitations of the study are the monocentricity, the small sample size, and the predominantly oncological sample, however, including hematological patients. Furthermore, the scale assessing strain has not yet been psychometrically tested and may not have captured fully the strain caused by the interview.
Generalizability of the reported feasibility may be hampered by the impact of limited health insurance in other countries, leading to shorter PCU stays.
Remarkably, the mean score for hope at both points of measurement was in the upper third of possible maximum scoring. The scores for the EORTC QLQ C-30 single item varied from 1 to 7 with mean 3.11, which was not as good as the observed scores for hope would have suggested. The FACT-G scores were in the upper third with high standard derivations. We found a significant increase for the physical subscale over time, which is most likely due to improved symptom control. The mean scores for FACIT-Sp were at the upper third of the maximum total score. Interestingly, most missing data were associated with the subscale “faith.”
Most of the palliative patients reported only average anxiety and depression, actually 14% and 18% low or very low scores (Fig. 2).
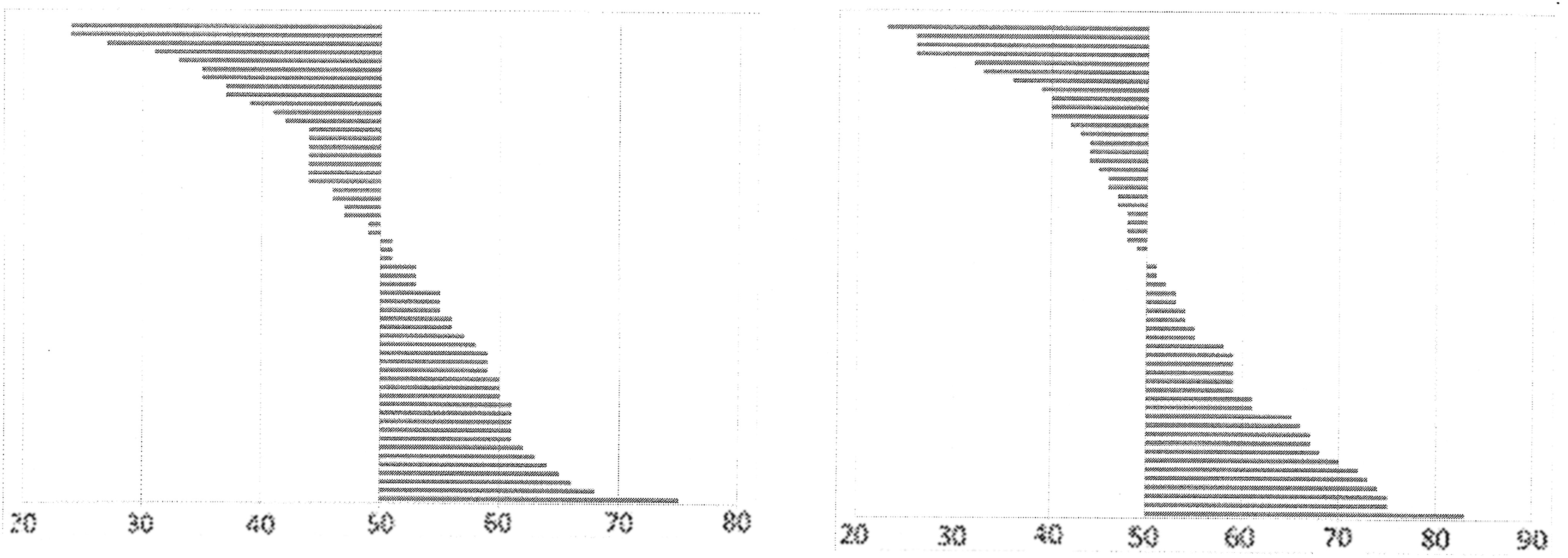
T-standardized anxiety scores (M = 50; SD = 10; one bar = one patient) and depression scores (M = 50; SD = 10; one bar = one patient) of the 56 palliative patients at hospitalization.
Further research questions are: What are the therapeutic effects of self-assessing psychological symptoms? Which correlations between specific psychometric data should we explore? What is determining inner peace?
Footnotes
Acknowledgment
We thank Facit.org (![]() ) for the permission to use the FACIT-Sp. Data used in this study will be published in an MD thesis (Viola Zeller, University Hospital Mainz, Germany).
) for the permission to use the FACIT-Sp. Data used in this study will be published in an MD thesis (Viola Zeller, University Hospital Mainz, Germany).
Author Disclosure Statement
No competing financial interests exist.