
Abstract
Abstract
Background:
Research on the effectiveness of evidence-based practices in the treatment of depression and anxiety with palliative care populations is primarily limited to individuals having specific conditions such as cancer.
Objective:
This meta-analysis examined the effect of psychotherapy on depression and anxiety among individuals with any condition appropriate for palliative care.
Methods:
We searched PubMed, PsycINFO, Cochrane Library, and EMBASE databases until August 2017. Eligible studies were randomized controlled trials of psychotherapy that reported outcomes of depression and anxiety and included adults with serious illnesses.
Results:
The current meta-analysis included 32 randomized controlled trials with 36 samples including 1536 participants undergoing psychotherapy. Overall, findings suggest that psychotherapy in palliative care populations reduced depression (large effect) and anxiety (small effect) symptoms. Psychotherapy also improved quality of life (small effect). Significant moderators of intervention effects included type of intervention and provider, number and length of treatment sessions, and sample age. Cognitive-behaviorally based and other therapies (e.g., acceptance, mindfulness) showed significant effects, as did interventions delivered by mental health providers. More treatment sessions were associated with greater effect sizes; longer sessions were associated with decreased effect sizes. As the sample age increased, the study effect size decreased.
Conclusion:
Findings suggest that psychotherapy for individuals with serious illnesses appropriate for palliative care can mitigate symptoms of depression and anxiety and improve quality of life. Methodological reporting and quality of research designs in studies of psychotherapy for palliative patient populations could be improved. Future research is needed with a broader range of patient populations.
Introduction
T
While research on interventions for psychological distress in the context of palliative care has primarily focused on pharmacotherapy, a growing literature evaluating the efficacy of psychotherapy exists. 24 This meta-analysis provides an overview of existing randomized controlled trials of psychotherapy examining effects on depression and anxiety among adults with any condition appropriate for palliative care, without emphasis on a particular disease. Here, psychotherapy is defined as psychological interventions conducted by trained individuals and involve direct verbal and interactive communication to improve distress. Because palliative care seeks to improve quality of life (QoL), a secondary aim was to examine QoL outcomes (when available) in the studies found through our search. Few moderators of the effectiveness of psychotherapy targeting depression and anxiety in palliative care populations have been analyzed in the literature. Knowledge of the intervention characteristics most likely to be effective and of patients most likely to benefit is greatly needed. Therefore, we examined whether patient population, psychotherapy type, provider type, and treatment modality and context moderated the effect of psychotherapy on outcomes. Per PRISMA recommendations, 25 we also examined the moderating effect of study quality in the relation between treatment and outcomes. Finally, we examined the role of participant demographic and treatment factors.
Methods
Search methodology
Searches of PubMed, PsycINFO, Cochrane Library, and EMBASE databases for the terms “psychotherapy OR psychological intervention” combined with the terms “palliative OR palliative care” were conducted through August 17, 2017. No specific disease terms were included.
To be included, studies had to (a) be written in English, (b) include adults ages 18 and older, (c) examine the effectiveness of a psychotherapy that involved at least two sessions or a minimum of 60 minutes of intervention, (d) use a randomized controlled design, (e) assess depression or anxiety symptoms as continuous variables, (f) provide sufficient information for computing within group effect size for outcomes, and (g) be published in a peer-reviewed outlet. Psychotherapies focusing on marital functioning, physical symptom reduction (e.g., pain), or health behavior change, and those that involved only psychoeducation, single skill building (e.g., relaxation), or support were excluded. Reference lists of reviews and included articles were also searched.
Data abstraction
Data abstraction was performed by one reviewer and confirmed by another. Studies were coded for population condition (cancer, multiple sclerosis, HIV/AIDS, advanced/terminal illness, other/mixed), sample size, participants' mean age, percentage of female participants, percentage of married participants, and percentage of racial/ethnic minorities participants. Additionally, psychological intervention characteristics, including modality type (individual, group, family), context (face-to-face, telephone), number of sessions, length of sessions, and provider type (mental health providers including psychologists, psychiatrists, and clinical social workers; healthcare providers including physicians, nurses, and occupational therapists) were abstracted. Interventions were categorized based on descriptions provided in the article; intervention categories included (1) cognitive and behaviorally (CB) based therapies, including cognitive behavioral therapy (CBT), cognitive therapy, problem solving therapy, and interpersonal therapy, (2) existential therapies including dignity, legacy, life review, and meaning making, and (3) other (e.g., acceptance and commitment therapy [ACT], mindfulness based stress reduction [MBSR], and supportive expressive therapy). Finally, information was coded to permit computation of effect sizes.
Quality assessment
Methodological quality of studies was independently assessed by two authors using criteria based on the Jadad Scale 26 and the Cochrane Collaboration's tool for assessing risk of bias 27 (Table 1). For each criterion met, one point was assigned. Scores ranged from 0 to 7 (0–4 low, 5–6 medium, 7 high quality). Twenty-six authors were contacted for additional information on quality; 10 responded with supplementary information. If author(s) did not respond, unclear criteria were rated as unmet.
Study included two active intervention arms.
P, pilot; MF, multi-site full; SF, single-site full; U, unclear.
Meta-analytic procedures
The standardized mean gain score (i.e., standardized change in scores from pretreatment to post-treatment; [mean post-treatment score–mean pretreatment score]/pooled standard deviation) was computed as a measure of effect size. 28 Statistical analyses were conducted using macros designed for meta-analysis. 29 When studies used multiple measures per outcome variable, effect sizes were averaged so each sample was only included once in analyses. 30 MeanES macro 29 was used to compute mean effect sizes and conduct homogeneity analyses using random effects models. When the homogeneity analysis statistic is significant, the variance in effect sizes exceeds what would be expected due to sampling error alone. 30 Forest plots were created using Neyeloff and colleagues' Excel spreadsheet. 31
MetaF macro 29 was used to test the effects of categorical moderator variables. Both between-class (QB) and within-class (QW) variability are computed. When between-class effect is significant, the moderator explains a significant amount of variability in the effect sizes. When within-class variability is not statistically significant, the moderator fully explains the variability; when within-class variability is still statistically significant, the moderator only partially explains the variability. 28
The effects of continuous moderator variables were tested using MetaReg macro. 29 The significance of the set of predictors in explaining the variability of effect sizes is tested with the homogeneity test for the regression model (QR), and the homogeneity test of the residual (QE) evaluates whether there is a significant amount of variance remaining. 29 While multiple predictors can be entered simultaneously, each possible moderator was tested separately because not every study included information for every moderator, and we sought to maximize power by including as many studies as possible in each analysis. In MeanES analyses, the homogeneity analyses were significant for all three outcomes; therefore, mixed effects models were used for all moderator analyses.28,30
Publication bias
The possibility of publication bias (i.e., tendency for studies with statistically significant results to be published and the tendency for studies with nonstatistically significant results to not be published) in the studies included in this meta-analysis was examined by a regression test 32 and funnel plots.
Results
Study characteristics
The combined searches yielded 2949 references. After excluding duplicates, 2757 unique citations remained (Fig. 1). Thirty-two studies with 36 samples receiving psychotherapy published between 1984 and 2014 with a total of 1536 participants were included (Table 2); our search found no studies published between November 2014 and August 2017 that met criteria for inclusion in this meta-analysis. The mean baseline sample size per study was 42.67 (SD = 31.51, range = 5–154). Average age ranged from 36.20 to 84.45 (unweighted M = 53.69). Percentage of the sample that was female ranged from 0% to 100% (unweighted M = 61.37), that were minorities ranged from 5% to 65% (unweighted M = 23.95), and that were married ranged from 32% to 75% (unweighted M = 58.53). The average number of sessions across studies was 8.96 (range = 1.96–23.00), and the average session length across studies was 75.37 minutes (range = 8.40–208.80). Half of the interventions included participants with cancer (n = 18),33–50 six included participants with multiple sclerosis,51–54 four included participants with HIV,55–57 four included participants with “advanced” “life-limiting” or “terminal” illnesses,58–61 and four studies included participants with multiple diagnoses or some other diagnosis.62–65 Most interventions used individual psychotherapy (n = 23; 63.9%).34–36,40–42,44–48,51–55,59–61,63–64 Ten studies used group therapy33,37–39,43,56,62; three used family therapy.46,57,58 Most interventions involved psychotherapy conducted face-to-face (n = 31; 86.1%)33–51,54,56–63 rather than by phone52,53,55,64 (n = 5; 13.9%), and mental health providers administered the intervention in most studies (n = 29; 80.6%).33–40,42–57,62–64 Most interventions were CB-based psychotherapies (n = 21),36–40,43–46,48,50–54,62–64 10 interventions were existential psychotherapies,33–35,41,42,57–61 and 5 were other types of psychotherapy.47,49,51–52,56

Flowchart of study selection process.
When values for demographic variables (age, % female, % minority, % married) were not available for the active treatment sample, values for the entire sample were used.
Publication years followed by a or b indicate two publications from the same author in 1 year.
Study included two active intervention arms.
BAI, beck anxiety inventory; BDI, beck depression inventory; BDI-II, beck depression inventory-II; CES-D, Center for Epidemiological Studies Depression Scale; COPD, chronic obstructive airway disease; CBT, Cognitive Behavioral Therapy; EOL, end of life; EORTC-QoL, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; EQ- 5D, EuroQol 5 Dimensions; FACT-G, Functional Assessment of Cancer Therapy-General Measure; GDS, Geriatric Depression Scale; HADS-A, Hospital Anxiety and Depression Scale-Anxiety Subscale; HADS-D, Hospital Anxiety and Depression Scale-Depression Subscale; HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale; HIV, Human Immunodeficiency Virus; HRSD, Hamilton Rating Scale for Depression; MACS, Mental Adjustment to Cancer Scale -Anxious preoccupation subscale; MQoL, McGill Quality-of-Life Scale; MADRS, Montogomery Asberg Depression Rating Scale; POMS-A, Profile of Mood States-Anxiety Subscale; POMS-D, Profile of Mood States-Depression Subscale; QoL, quality of life; QUAL-E, quality of life at the end of life; SCL-90-R, Symptom Checklist-90 Revised; SISC, Structured Interview for Symptoms and Concerns; SOSI-A, Symptoms of Stress Inventory-Anxiety; SOSI-D, Symptoms of Stress Inventory-Depression; STAI-S, State Form of the State-Trait Anxiety Inventory; U, Unknown.
Quality assessment
Quality assessment ratings ranged from 3 to 7 (Table 1). Most studies (n = 24) were of medium quality. All studies met Criterion 7 (diagnostic assessment of the primary outcome conducted by a professional or no diagnostic assessment necessary for recruitment). Conducting a power analysis (i.e., to estimate a sufficient sample size to achieve adequate power) and basing the study sample size on this power analysis (Criterion 5) was the criterion met most infrequently (n = 12).
Mean effect sizes and homogeneity analyses
Effect sizes are interpreted based on Cohen's d effect size criteria 65 (i.e., 0.2 = small, 0.5 = medium, and 0.8 = large). Mean effect sizes and results of the homogeneity analyses are presented in Table 3; Forest plots are presented in Figures 2–4. The mean effect sizes for depression and anxiety were significant and negative, indicating that, overall, psychotherapy in palliative care populations reduced depression and anxiety symptoms. Psychotherapy had a large effect on depression symptoms and a small effect on anxiety symptoms. The mean effect size for measures of QoL was significant, small, and positive, indicating that these interventions improved QoL. The homogeneity analyses for all effect sizes were significant, indicating that the variability in effect sizes was greater than would be expected by sampling error alone, 28 which suggests that there are possible moderators contributing to study effect sizes.
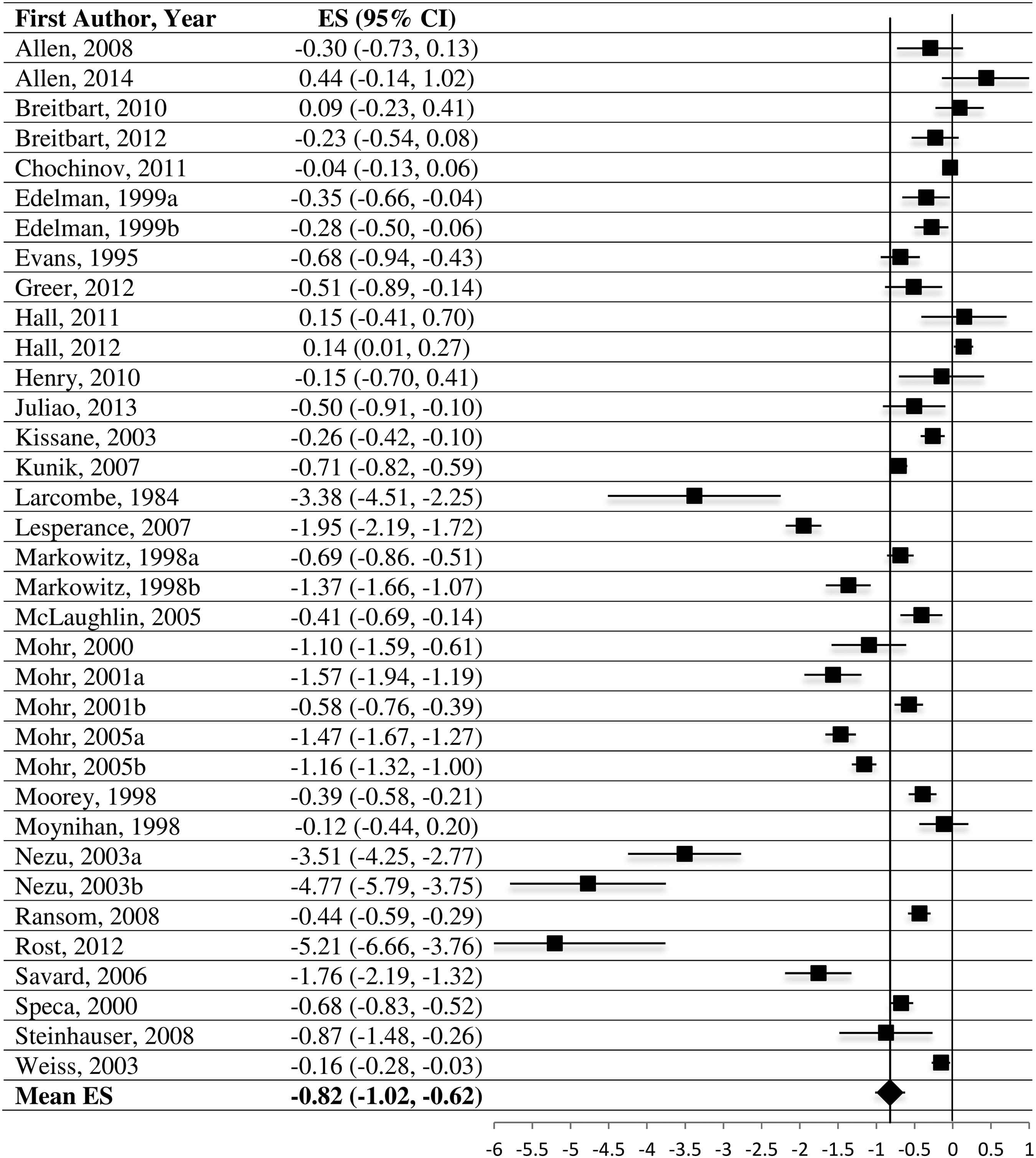
Forest plot of depression effect sizes.

Forest plot of anxiety effect sizes.
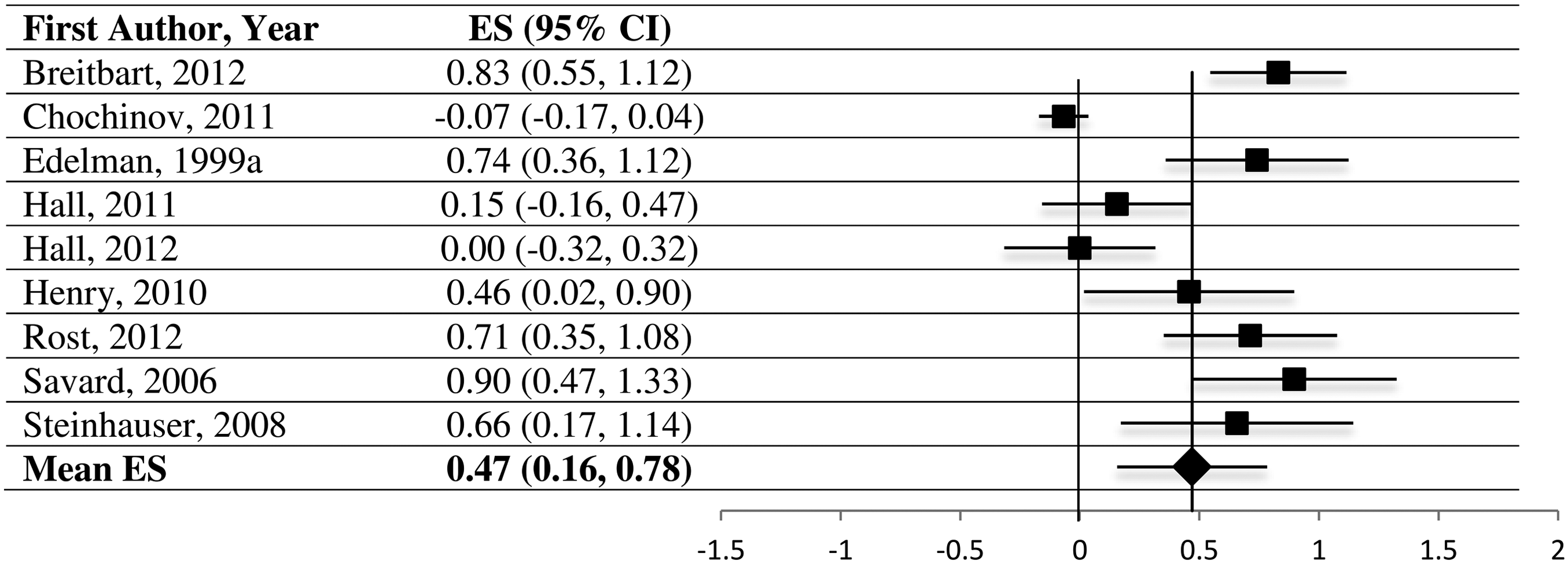
Forest plot of quality of life effect sizes.
p < 0.01, **p < 0.001.
CI, confidence interval; ES, effective size; SE, standard error.
Analyses of categorical moderators
Categorical moderators could only be tested when there were at least three studies per category for a given effect size. Thus, population condition was dichotomized (i.e., cancer vs. other) when examining studies that included anxiety as an outcome. For treatment modality, only individual versus group was examined as no studies that included anxiety as an outcome used family therapy. Additionally, the effects of population condition, psychotherapy type, provider type, treatment modality, treatment context, and study quality could not be examined for QoL effect sizes. Results of MetaF tests for categorical moderators are presented in Table 4.
p < 0.05, **p < 0.01, ***p < 0.001.
HIV, Human Immunodeficiency Virus; AIDS, Acquired Immune Deficiency Syndrome; CT, Cognitive Therapy; CET, Cognitive-Existential Therapy; PST, Problem Solving Therapy; DT, Dignity Therapy; LR, Life Review; MM, Meaning Making; Ex, Existential therapy; IPT, interpersonal therapy.
Psychotherapy type had a significant effect on depression and anxiety outcomes. For studies examining effects on depression, CB-based therapies and other therapies resulted in large, statistically significant effect sizes; however, studies that used existential therapies did not have an overall significant effect size. Similarly, among studies examining anxiety as an outcome, CB-based therapies and other therapies resulted in statistically significant effects (small and medium, respectively); existential therapies did not result in a significant effect.
Provider type was a significant moderator of depression and QoL effect sizes. Specifically, studies in which mental health providers administered the treatment had statistically significant average effects on depression (large effect) and QoL (medium effect), but studies in which other types of providers (e.g., healthcare providers) administered the treatment did not have a significant average effect size for depression or QoL.
Analyses of continuous moderators
Analyses of continuous moderators were possible for most moderators on each outcome; however, too few studies examining QoL as an outcome reported the mean session length and the percentage of minority participants in the sample, so these moderators were not tested for studies that examined QoL outcomes. Results of analyses for continuous moderators are presented in Table 5.
p < 0.05, **p < 0.01, ***p < 0.001.
For studies examining depression symptoms as an outcome, mean number of treatment sessions, mean length of sessions, and mean age of the sample were significant predictors of the study effect size. Because the mean effect size for depression was negative, a negative beta indicates an increase in effect size and a positive beta indicates a decrease in effect size. Therefore, as the mean number of treatment sessions increased, the effect size increased, but as the mean length of sessions and the mean age of the sample increased, the study effect size decreased.
For studies examining anxiety symptoms as an outcome, no continuous moderator analyses were significant. Among studies examining QoL, mean age of the sample was a significant predictor of effect size. Specifically, as mean age of the sample increased, study effect size decreased.
Investigation of publication bias
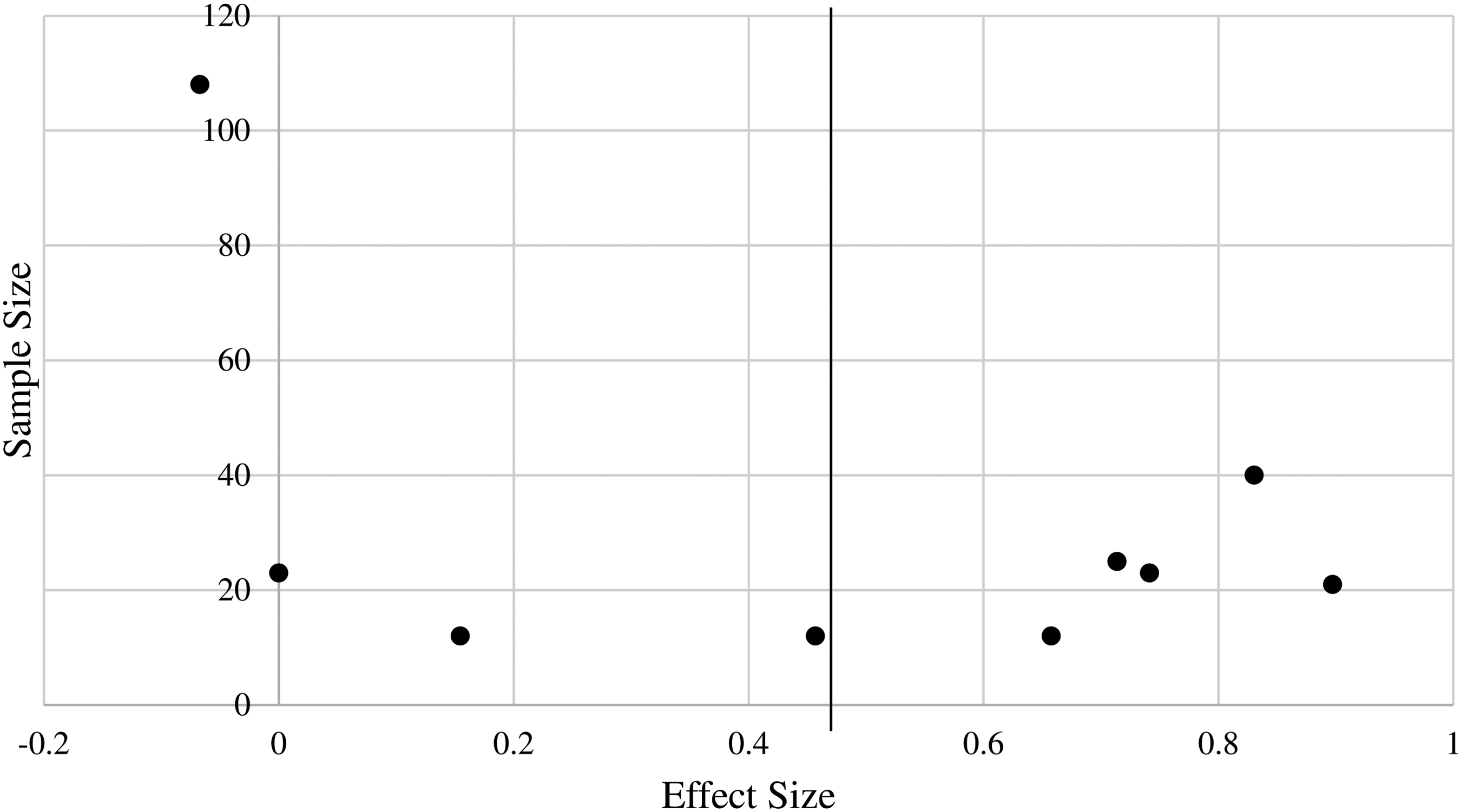
Funnel plots for studies that provided effect sizes for each outcome are presented in Figures 5–7. The results of the regression tests demonstrated funnel plot asymmetry for depression [b = −4.33, t(33) = −2.83, p = 0.008] and QoL [b = 4.45, t(7) = 3.80, p = 0.007] but not anxiety [b = −2.10, t(19) = −1.59, p = 0.128], suggesting publication bias in studies examining depression and QoL as outcomes (i.e., depression and QoL effect sizes may be overestimated).
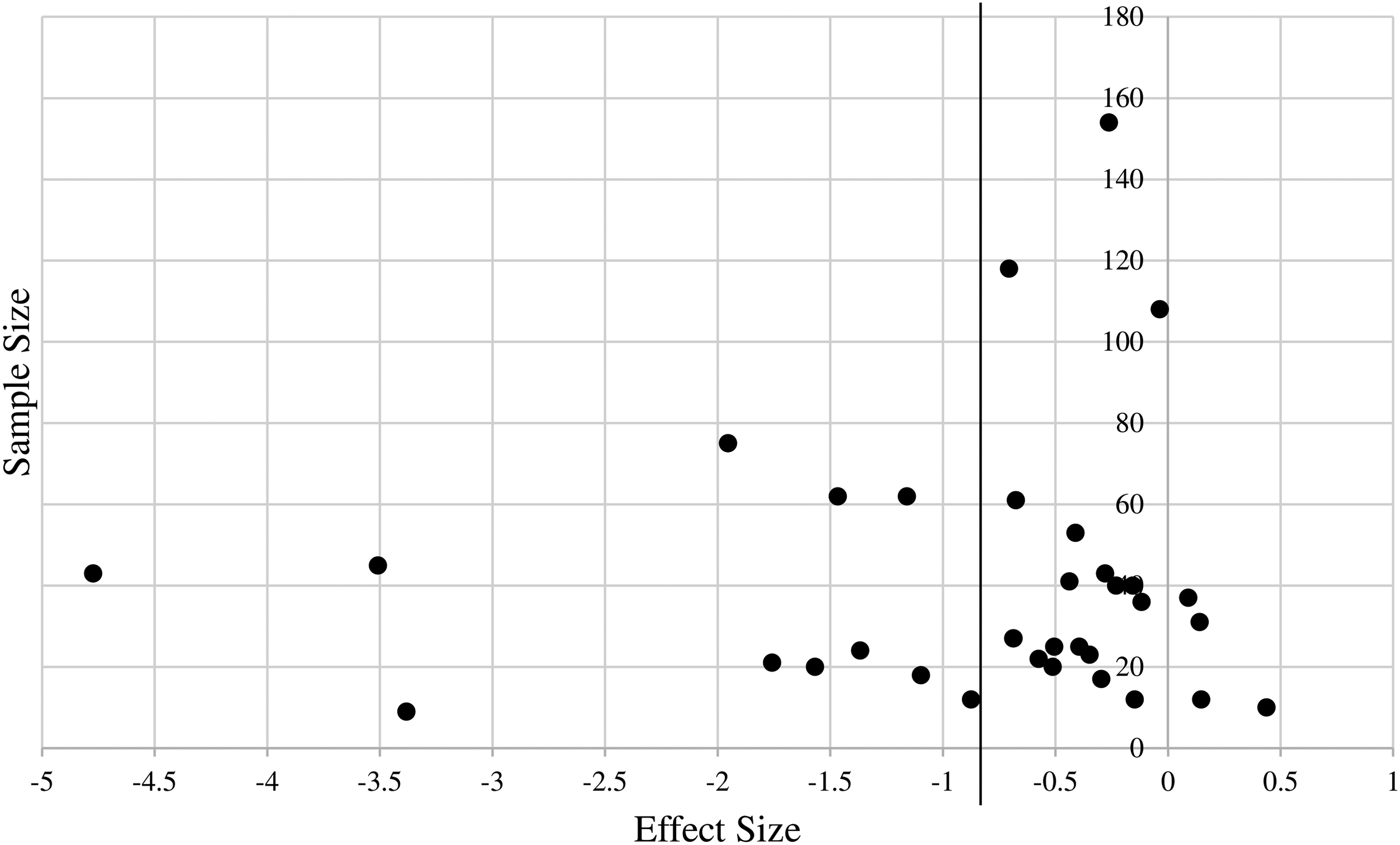
Funnel plot for studies reporting outcomes for depression.
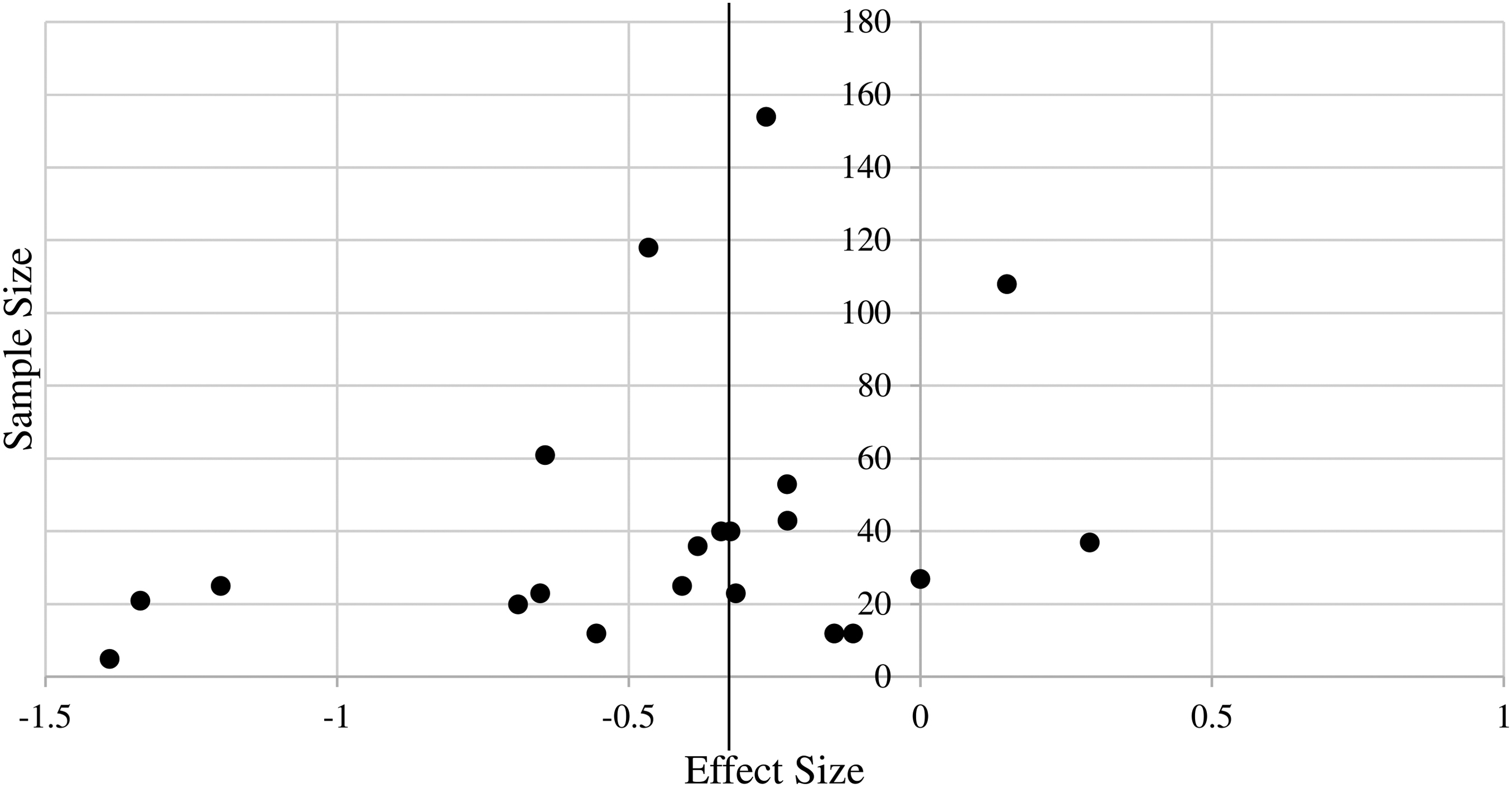
Funnel plot for studies reporting outcomes for anxiety.
Funnel plot for studies reporting outcomes for quality of life.
Discussion
Although palliative care guidelines recommend psychological treatment of distress 1 among palliative care populations, an evaluation of the evidence for psychotherapy being used with this population has not been conducted. The primary aim of this meta-analysis was to examine whether psychotherapy among individuals with conditions that could warrant palliative care resulted in reductions in depression and anxiety symptoms between pre- and post-treatment. In a meta-analytic review of 32 studies with 36 samples, psychotherapy was found to be effective for reducing depression and anxiety symptoms and improving QoL among patients appropriate for palliative care. While there was significant variability in effect sizes across studies, on average, the reduction in depression symptoms between pre- and post-treatment was large. Although the results also revealed that psychotherapy reduced anxiety symptoms, the mean effect size was small. The secondary aim was to examine whether these interventions resulted in improvements in QoL. In general, psychotherapy resulted in a significant increase in QoL, but the effect size was small.
Multiple moderators of study effect sizes were examined. Psychotherapy type was significantly associated with depression and anxiety effect sizes. Specifically, the mean effect size for studies that used therapies typically designed to target existential distress (e.g., dignity therapy, life review) was not significant, indicating that these therapies did not improve depression or anxiety symptoms. In contrast, both CB-based therapies and other types of psychotherapy (e.g., ACT, MBSR) did result in reductions in depression and anxiety symptoms. Interestingly, while interventions with a greater number of treatment sessions resulted in greater reduction in depression symptoms, longer treatment sessions resulted in less reduction in depression symptoms. This finding may reflect the inability of patients with serious illness to tolerate lengthy sessions (i.e., on average 75 minutes long), suggesting that more shorter sessions is preferable to fewer longer sessions.
In addition, studies in which mental health providers administered the treatment had significant effects on both depression and QoL, but studies that used other types of providers did not have significant effects on depression or QoL. When the mean age of the sample was older, the effect size for depression and QoL was smaller (i.e., treatment was less effective). This finding possibly reflects the fact that older patients generally report lower levels of distress 66 and therefore may be less likely to benefit from intervention. Alternatively, older adults compared to younger adults may not fully benefit from interventions like CBT without treatment modifications (e.g., adjusting pacing of treatment, providing written material) that account for age and health-related factors.67–69
Taken together, these findings suggest that CB-based and other (e.g., acceptance, mindfulness) therapies delivered by mental health providers are effective methods of mitigating depression and anxiety among adults appropriate for palliative care. The large effect size on depression is notable in comparison to effect sizes reported in meta-analyses of psychotherapy for cancer patients that are generally in the small range. 70 This finding may reflect the higher symptom burden among patients whose conditions warrant palliative care. It may also reflect the relatively high dose of the interventions tested. While existential therapies did not have a significant effect on anxiety, depression, or overall QoL, it is likely that they impact other important outcomes such as spiritual well-being that may not be reflected in measures of psychological distress. 71
Overall, these findings suggest that the clinical care of palliative care patients with anxiety and depression could be improved by the provision of cognitive-behavioral and other (acceptance, mindfulness) therapies by mental healthcare providers. This may require greater integration of psychologists, who have doctoral-level training in the provision of such therapies, into palliative care teams. 1 While psychological and psychiatric care is a recommended part of palliative care practice, it is not currently required, and mental health providers are likely not included in most palliative care programs. 72 Future studies should also evaluate the effects of including psychotherapy for psychological distress as part of palliative care services.
The results of this meta-analysis should be interpreted in light of limitations. First, results indicate likely publication bias in studies examining depression and QoL. Second, most studies identified focused on patients with cancer. Given the limited number of studies examining interventions with other conditions (e.g., HIV), these studies had to be combined into a single group to examine condition as a moderator. In addition, due to limited information on treatment settings (e.g., inpatient, outpatient), setting could not be examined as a moderator. Thus, the degree to which these findings generalize to specific medical conditions and palliative care settings remains unknown. Third, there was a confound between psychotherapy and treatment provider variables, as only one of the seven studies that used nonmental health providers implemented CBT and the others examined existential therapies.
This meta-analysis also revealed limitations of the current literature on this topic. First, the methodological quality of research designs and reporting could be improved. On average, the quality rating was medium, and we noted a possibility of publication bias in studies examining depression and QoL as outcomes. Methods of improving quality of studies could include tracking reasons for participant attrition, using intention-to-treat analysis to address missing data, and using a priori power analysis to determine adequate sample sizes. Future research should also focus on a wider range of patients appropriate for palliative care and those most at risk for poor outcomes without intervention. Finally, future studies should include greater detail about population and study characteristics (e.g., race/ethnicity, disease stage, concurrent psychopharmacological treatment, treatment setting) and the specialty care being received in addition to disease-specific treatment/care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.