
Abstract
Abstract
Background:
In 2011–2013, >95% of the global opioid analgesics consumption occurred in three regions, accounting for 15% of the world population. Despite abundant literature on barriers to access, little is known on the correlation between actual access to opioid analgesics and barriers to access, including legal and regulatory barriers.
Objective:
This study aimed to evaluate the correlation between access to strong opioid analgesics and barriers to access in national legislation and regulations in 11 central and eastern European countries that participated in the Access to Opioid Medication in Europe (ATOME) project.
Design:
Two variables were contrasted to assess their correlation: the country level of access to strong opioid analgesics indicated by the Adequacy of Consumption Measure (ACM) and the number of potential legal and regulatory barriers identified by an external review of legislation and regulations.
Measurements:
A linear correlation was evaluated using a squared linear correlation coefficient.
Results:
Evaluation of the correlation between the ACM and the number of potential barriers produces an R2 value of 0.023 and a correlation plot trend line gradient of −0.075, indicating no correlation between access to strong opioid analgesics and the number of potential barriers in national legislation and regulations in the countries studied.
Conclusions:
No correlation was found, which indicates that other factors besides potential legal and regulatory barriers play a critical role in withholding prescribers and patients essential pain medication in the studied countries. More research is needed toward better understanding of the complex interplay of factors that determine access to strong opioid analgesics.
Introduction
I
These data—representing a high prevalence of inadequately treated pain—are in line with global consumption data of opioid analgesics.3–6 Recently published data from the International Narcotics Control Board (INCB) 6 show that a major part of the world population still lacks access to opioid analgesics, even though several international treatment guidelines recognize that these medicines are indispensable for the relief of moderate–to-severe (cancer) pain.7–10 In 2011–2013, 95.7% of the global consumption of opioid analgesics occurred in three regions, accounting for only 15% of the global population. 6 Even though progress in opioid analgesic use was seen, this growth was mainly accountable to high-income countries and minimal improvement was seen in low- and middle-income countries. 6
To improve access to opioid analgesics, it is paramount to identify factors that are associated with inadequate access. According to policy guidelines of the World Health Organization (WHO), these factors can be classified into four different categories: (1) economic or financial circumstances, (2) factors relating to societal attitudes, (3) knowledge and educational issues, and (4) policies or regulations. 11 Despite abundant literature on factors that are perceived to interfere with access to opioid medicines, little is known on the correlation between individual factors and access in clinical practice.
In the category of factors relating to economic circumstances, the human development index (HDI) and the gross domestic product (GDP) have been shown to be predictive variables for a country's opioid consumption level.6,12–14 But little evidence exists for other determinants of access to opioid analgesics, including issues relating to drug control systems that have frequently been reported to impede access to opioid medicines in a way that is disproportional to their benefit for the prevention of nonmedical use.10,15–21
This study, therefore, aimed to evaluate the correlation between access to strong opioid analgesics and potential legal and regulatory barriers in 11 central and eastern European countries that participated in the access to opioid medication in Europe (ATOME) project.
Materials and Methods
Data collection
In this study, the level of consumption of strong opioid analgesics was calculated using a modified version of the Adequacy of Consumption Measure (ACM). The ACM is based on consumption data of opioid analgesics that are mandatorily reported to the INCB. 12 It was first developed by Seya et al. using data from 2006 and recalculated by Duthey and Scholten for 2010.12,22 For this article, author W.K.S. calculated the modified ACM (hereinafter also referred to as ACM) excluding the morbidity correction and the opioid medicine pethidine, which is considered obsolete.
First, the per capita consumption of the four main opioid full-agonist analgesics (fentanyl, hydromorphone, morphine, and oxycodone) was calculated for each of the countries in this study: Bulgaria, Cyprus, Estonia, Greece, Hungary, Latvia, Lithuania, Serbia, Slovakia, Slovenia, and Turkey. Consumption data were used for 2013 for all countries with the exception of Greece: for Greece, data from 2010 were used, as data from 2013 were not available. As a second step, equipotent quantities were calculated using the WHO defined daily dose as a conversion factor, 23 expressed as “mg morphine equivalents.” As a third step, the average per capita consumption of the top 20 most developed countries worldwide (according to HDI) was calculated and set as a benchmark (defined as 100%), being considered an adequate level of consumption. As a final step, the ACM was calculated as a proportion of this benchmark, based on the per capita consumption of opioid analgesics and expressed as a fraction of the benchmark. For example, a country consuming 60% of the average of the 20 most developed countries has an ACM of 60%. Since this study focuses on European countries, for further comparison, the ACM was also calculated for the three European countries ranking highest in the HDI (Norway, Switzerland, and Denmark) (Table 1).
Per capita consumption expressed in millgram morphine equivalents. Data for 2013 (Greece: data for 2010).
Owing to rounding errors, the sum in this column may slightly deviate from total of the columns “Contribution to ACM, %.”
ACM, Adequacy of Consumption Measure; ATOME, access to opioid medication in Europe.
The number of potential barriers was identified in an external review of national legislation and regulations in each of the 11 countries that was conducted as part of the ATOME project. 24 This analysis used eight predefined categories to group the potential barriers that were identified: prescribing, dispensing, usage, affordability, manufacturing, trade and distribution, penalties, and other. 24 The total number of potential barriers for all eight categories was calculated for each country (Table 2).
Analysis
Both variables (ACM and number of potential barriers, see Tables 1 and 2) were contrasted to assess the correlation between the ACM and the number of potential barriers identified in national legislation and regulations. Closeness of fit was assessed by plotting the reported number of potential barriers of individual countries against the ACM in these countries. A squared linear correlation coefficient (R 2 ) was obtained, which provides an index of the degree to which the paired measures covary. As a secondary examination, we restricted the analysis to potential barriers in the categories prescribing and dispensing as it may be assumed that these types of barriers are more likely to influence access than others. Finally, we did an additional sensitivity analysis excluding potential barriers to access to opioid medicines that specifically focused on the treatment of opioid dependence.
Results
The ACM for each country, the benchmark (an ACM of 100%), and European consumption levels (top three HDI and European average) are presented in Figure 1 and more in detail in Table 1. The results show a wide variation between study countries in their ACM, ranging from 4% of the global benchmark (Cyprus) to 57% of the global benchmark (Slovenia), indicating an opioid analgesic consumption level that is very low to moderate. In addition, for each country the total number of potential barriers in national legislation and regulations is presented in Table 2. When contrasting the ACM and the total number of barriers, a wide spread between individual countries was observed (Fig. 2).
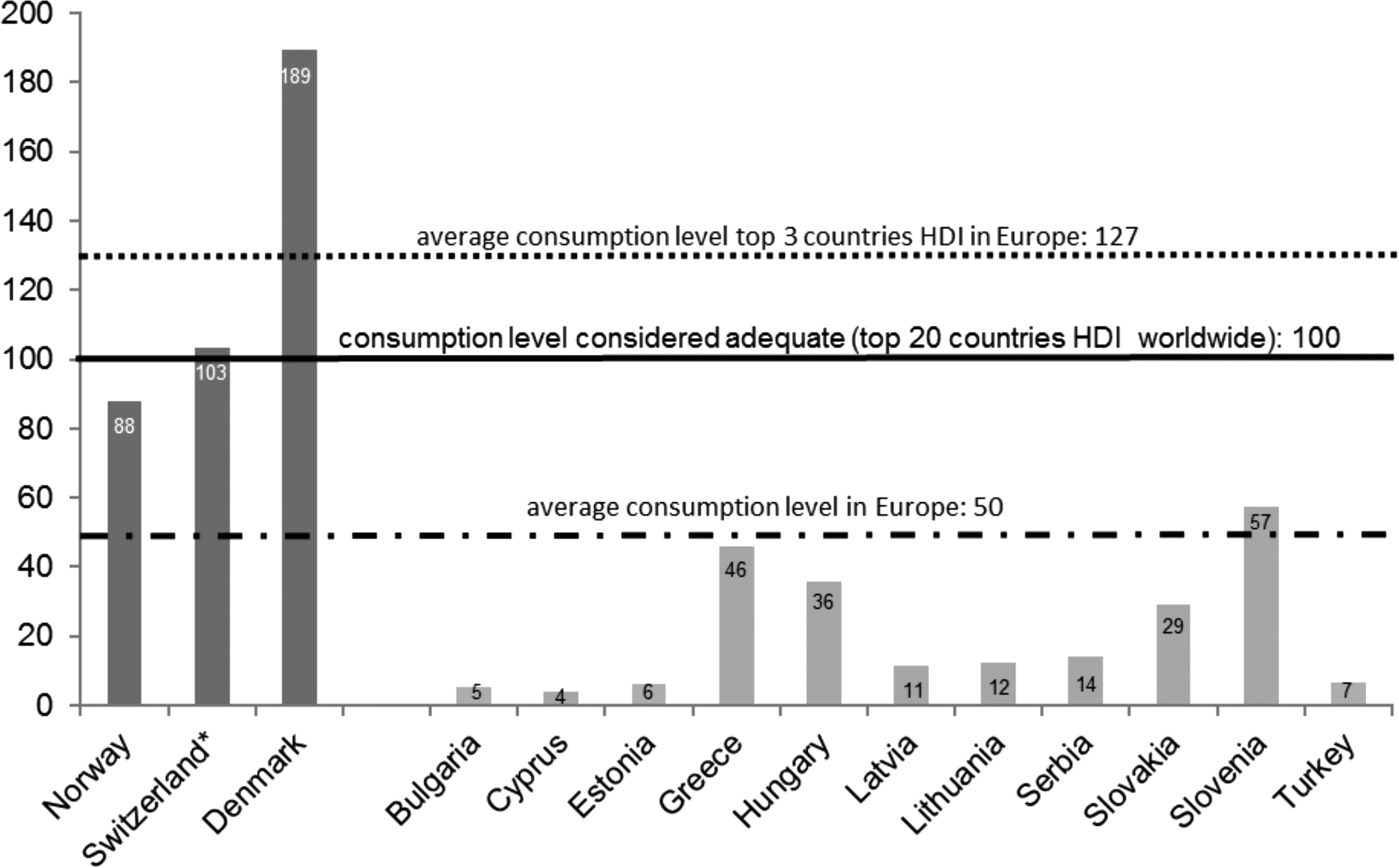
The ACM calculated based on the per capita consumption of the four main opioid analgesics in 2013 (Greece: data for 2010). Per capita consumption expressed in milligram morphine equivalents for the 11 central and eastern European countries in this study and the top 3 countries in the HDI. *including Liechtenstein. ACM, Adequacy of Consumption Measure; HDI, human development index.
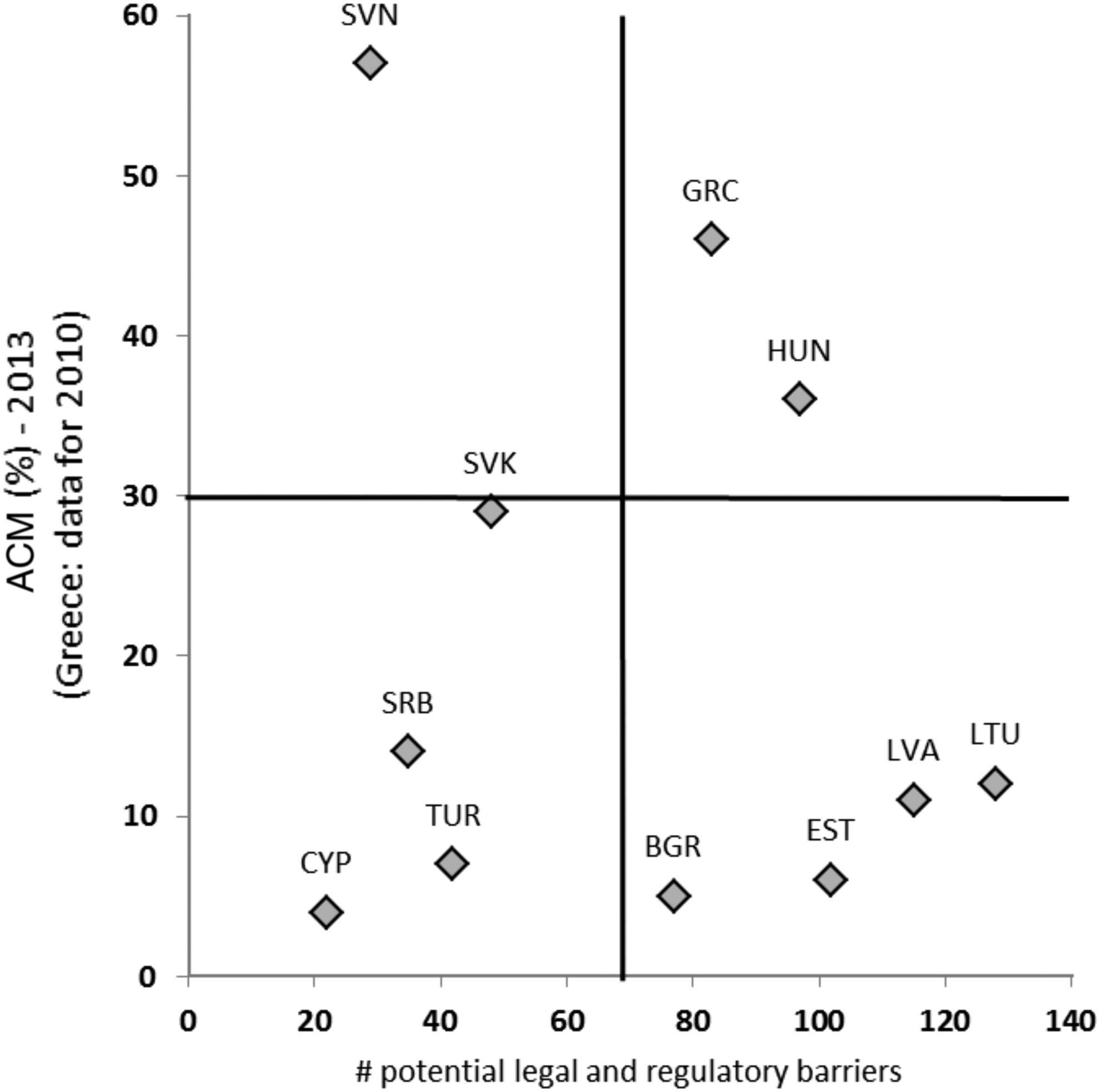
Noncorrelation between access to opioid analgesics (ACM) and the number of potential legal and regulatory barriers in 11 central and eastern European countries: Bulgaria (BGR), Cyprus (CYP), Estonia (EST), Greece (GRC), Hungary (HUN), Latvia (LVA), Lithuania (LTU), Serbia (SRB), Slovakia (SVK), Slovenia (SVN), and Turkey (TUR).
Looking at the results in Figure 2, we can identify three distinct clusters of countries based on distance from the center and positioning on both axes. In the upper right quadrant, there is a cluster of two countries (Greece and Hungary) with a relatively high level of access to strong opioid analgesics, despite a relatively high number of potential barriers. The cluster of countries in the lower left quadrant (Cyprus, Serbia and Turkey) shows the contrary: access to strong opioid analgesics is (very) low despite a relatively low number of potential barriers. A third cluster of countries in the lower right quadrant shows a pattern that is more in line with expectations: four countries with low (10%≤ ACM <30%: Latvia and Lithuania) to very low (3%≤ ACM <10%: Bulgaria and Estonia) access to strong opioid analgesics and a relatively high number of potential barriers in national legislation and regulations.
Evaluation of the correlation between the ACM and the number of potential barriers produces an R 2 value of 0.023 and a correlation plot trend line gradient of −0.075, indicating no correlation (formula: y = −0.0745x + 25.903). Similar results were obtained in case the analysis was restricted to two separate categories of potential barriers (prescribing and dispensing), R 2 value of 0.007 (formula: y = −0.062x + 23.162), and when excluding potential barriers to access to opioid medicines for the treatment of opioid dependence, R 2 value of 0.002 (formula: y = −0.029x + 22.306).
Discussion
In this study, we aimed to evaluate the correlation between the level of access to strong opioid analgesics, indicated by the ACM and the number of potential barriers in national legislation and regulations in 11 central and eastern European countries. The low R 2 value (2% variance explained) indicates that there is no correlation between ACM and the number of potential barriers in legislation and regulations in the countries studied. Our findings suggest that other factors play a role in explaining variation in access to strong opioid analgesics. For example, one of the findings of the ATOME project was that pain treatment education in the medical curriculum falls short in many countries. 25 Later, similar conclusions were drawn from the Advancing the Provision of Pain Education and Learning study. 26 Unfortunately, there are no studies examining a possible correlation between the ACM and the level of treatment education.
We would expect to find a decrease in the ACM as the number of potential barriers in national legislation and regulation increases and vice versa. However, looking at the results shown in Figure 2, there are two clusters of countries that show a pattern that is not in line with these expectations. Two countries in the upper right quadrant (Greece and Hungary) have a relatively high level of access to strong opioid analgesics compared with the other countries in this study, despite a relatively high number of potential barriers.
A possible explanation could be that some of the overly strict rules that are set out in law (de jure) in these countries are not always followed in practice (de facto). For example, a workaround has been found to bypass certain barriers, or violation of rules may be tolerated to a certain level. A prime example can be found within the field of harm reduction wherein a country may choose not to prosecute drugs possession for personal use based on discretionary powers although it remains an act against the law. 27 In the same manner, potential barriers that were identified in national legislation and regulations in these countries may not constitute actual barriers in practice.
The cluster of countries in the lower left quadrant shows the contrary: access to strong opioid analgesics is low (Serbia) to very low (Cyprus and Turkey), despite a relatively low number of potential barriers. In these countries, other factors may play a more significant role in impeding access to opioid analgesics, such as issues concerning the affordability of opioid analgesics or fear for opioid analgesic use. For Cyprus, the relatively low number of potential barriers may possibly be related to the fact that Cyprus is a former British colony. 28 It is not unlikely that influences from British colonial times are still visible in legislation. However, there are no (scientific) data available to support this theory. Serbia underwent a legislation review process as a part of an international pain policy fellowship to improve the availability and accessibility of opioids for cancer pain. As a result, a new law on psychoactive controlled substances was enacted in 2011, which is likely to have contributed to the relatively low number of potential barriers. 29 The impact of this revision may not yet have resulted in a (substantially) higher level of opioid consumption.
A similar initiative in Vietnam that started earlier appeared to have supported the reduction of barriers to access, with a year-on-year increase in morphine consumption per capita since the start of the project in 2005 until 2010. 30 However, as this project comprised a broad set of actions and no research has been conducted to examine the correlation between the different interventions and morphine consumption, it remains difficult to highlight indicators for success. In a study that evaluated the effectiveness of a series of workshops aimed at improving access to opioids in 13 Latin American countries, no significant differences were seen between countries that had one, two, or no workshops, and the outcome measures being (changes in) opioid consumption and formulations available. 14 The authors discussed that it may take several years before results can be observed. 14
For Cyprus, Serbia, and Turkey, key challenges to access to opioids were identified in aspects concerning education and training, societal attitudes, and financial issues in addition to legal and regulatory issues. 25 In all three countries, fear of opioid medicines and misconceptions around their medical use (for example, the misconception that prescribing of opioid medicines automatically results in opioid dependence or hastened death) were considered a major barrier to access.25,29 More (financial support for) education and training in pain management and palliative care were considered a necessity to improve the current situation. In addition, more financial resources are needed to support the treatment of pain, palliative care, or harm reduction. In Cyprus, for example, due to lack of governmental funding, the provision of palliative care mostly relies on charity funds. 25
We also see countries showing a pattern that is more in line with expectations. In the lower right quadrant, there is a cluster of countries (n = 4) with low (Latvia and Lithuania) to very low (Bulgaria and Estonia) access to strong opioid analgesics and a relatively high number of potential barriers in national legislation and regulation. In the upper left corner, we see one country (Slovenia) with moderate access to strong opioid analgesics and a relatively low number of potential barriers. Although we describe countries that have a relatively high level of opioid analgesic consumption, it should be noted that the level of opioid analgesic consumption is considered inadequate in all 11 countries studied and even below the European average in 10 of the 11 countries.
Besides GDP and HDI, there is little evidence for determinants of access to opioid analgesics. A recent study by Berterame et al. assessed the correlation between actual consumption data of opioid analgesics and impediments to access to opioid analgesics. 6 Information on the number of impediments was collected by sending a survey on various impediments to 214 national authorities, which included the impediment “onerous regulations.” The authors found that the frequency of the reported impediment “onerous regulations” decreased substantially since 1995. Moreover, they found that after adjustment for GDP and country-level development, the total number of reported impediments (including onerous regulations) was no longer associated with use of opioid analgesics. Governments of countries with a low GDP and/or HDI may have difficulties in ensuring the availability and affordability of opioid medicines due to limited resources and infrastructure, as indicated by the significant relationship between GDP, HDI, and use. 6
A potential limitation of the study by Berterame et al. is that other important stakeholders such as healthcare professionals and patient representatives involved in pain management were not included in the surveys. As different stakeholders may perceive different types of barriers, limiting the group of respondents to national authorities may have caused underreporting of the number and nature of impediments. 31 A strength of our study is that we used data on potential barriers that were identified by an external review of legislation and were disseminated to the ATOME country teams for validation. 32 These ATOME country teams included various stakeholders, among whom are healthcare professionals, patient representatives, and national authorities. An additional study has been undertaken by the ATOME working group to assess differences in the perception of barriers to access to opioid medicines among key stakeholders; a publication is currently in preparation.
Several limitations of this study should be considered when interpreting the results. First, the limited sample size may have caused the study to be underpowered to identify significant differences between countries. Second, as data from 2013 were not available for Greece, we used data from 2010. Changes in opioid analgesic consumption may have taken place in the period between 2010 and 2013, resulting in underestimation or overestimation of the ACM for Greece. However, in the 10 other countries, only small changes were seen between 2010 and 2013 (average change −1%; range −7% to +3%). Third, this study evaluated potential barriers to access to opioid medicines in relation to opioid analgesic consumption data. These opioid analgesic consumption data did not include opioid agonists such as methadone. However, similar results were found when excluding potential barriers to access to opioid medicines used for the treatment of opioid dependence. Possible future steps may include validation of this updated method to calculate the level of opioid consumption on a wider scale.
Conclusions
In conclusion, our hypothesis that countries with a heavier burden of legal and regulatory barriers to control strong opioid analgesics would have even less access to these essential medicines for patients in medical need could not be confirmed. This is an important result in the context of finding solutions for improving access to opioid analgesics for patients in need for effective and safe pain medication. Obviously, there are other factors that play a critical role in withholding prescribers and patients essential pain medication. More research is needed toward better understanding of the complex interplay of factors that determine access to opioid analgesics.
Footnotes
Acknowledgments
The data on the legal and regulatory barriers were previously obtained as a part of the Access To Opioid Medication in Europe (ATOME) project. The research leading to these results has received funding from the European Community's Seventh Framework Programme [FP7/2007-2013] under grant agreement no. 222994 with the overall aim to improve the access to opioid medication in Europe. The authors thank the International Narcotics Control Board for providing opioid consumption data.
Author Disclosure Statement
The authors declare no potential conflicts of interest that are directly relevant to the content of this article. H.G.M.L. and A.K.M.T. have received unrestricted research funding from The Netherlands Organisation for Health Research and Development (ZonMw), the private–public funded Top Institute Pharma (![]() , includes cofunding from universities, government, and industry) and Innovative Medicines Initiative (IMI, Leufkens only), the EU 7th Framework Program (FP7), the Dutch Medicines Evaluation Board, the Dutch National Health Care Institute (H.G.M.L. only) and the Dutch Ministry of Health.
, includes cofunding from universities, government, and industry) and Innovative Medicines Initiative (IMI, Leufkens only), the EU 7th Framework Program (FP7), the Dutch Medicines Evaluation Board, the Dutch National Health Care Institute (H.G.M.L. only) and the Dutch Ministry of Health.
W.K.S. provides consulting services as an independent consultant on regulation of and policies related to psychoactive substances. Examples of these include conducting workshops on availability of pain management, providing an overview of importation and exportation rules, providing information on controlled substance policies, the review of cannabis, and the application of the International Nonpropietary Name. This has included work for the World Health Organization, Pinney Associates, Jazz Pharmaceuticals, Grünenthal, Mundipharma, and DrugScience. He is a member of the board of International Doctors for Healthier Drug Policies.