
Abstract
Abstract
Background:
The optimal treatment of malignant ascites (MA) and feasibility of the management with free drainage remain unclear.
Objective:
To study the success of drainage, complications, and survival after paracentesis or insertion of an indwelling tunneled catheter (TC) for the MA performed on a day-case basis.
Design and Setting:
We evaluated 118 paracenteses and 48 insertions of TCs performed in 104 patients with MA at the Palliative Care Outpatient Unit of Tampere University Hospital.
Results:
Drainage of ascites fluid (median 3700 mL; range 300–13,200 mL) was successful in all cases. The complication rates were 7% and 25% for paracenteses and TCs, respectively. Most of the complications were minor. Repeated procedures were needed in 64% and 10% of the paracenteses and insertions of TCs, respectively, (p < 0.001). Median survival after the first procedure was 40 days (interquartile range, IQR: 17–115). Patients with pancreatic cancer had shorter median survival (19 days; IQR: 9–35) compared with other patients (47 days; IQR: 23–143) (age-adjusted HR 2.73; 95% CI: 1.65–4.52), whereas patients receiving chemotherapy had longer median survival (112 days; IQR: 43–205) compared with patients without chemotherapy (25 days; IQR: 14–52) (age-adjusted HR 2.48; 95% CI: 1.58–3.89). The volume of removed ascites fluid was not associated with survival.
Conclusions:
Free drainage of MA seems feasible in an outpatient clinic. Early insertion of TC should be considered to avoid repeated paracenteses. However, in patients with pancreatic cancer, paracentesis might be an accepted alternative due to their short life expectancy.
Introduction
M
There are no clear guidelines for the optimal treatment of MA. In palliative care settings, repeated large-volume paracenteses or insertions of a permanent tunneled catheter (TC) are shown to be effective in relieving the symptoms of MA, whereas diuretics or dietary restrictions are rarely beneficial.1,8 The choice between paracentesis and TC is mainly done according to physician's judgment about the benefits and risks of the procedure along with the wishes of the patient. As a single procedure, paracentesis is easy to perform, has a low risk of complications, and is less costly than TC. However, repeated paracenteses are often needed as the ascites fluid accumulates again. 9 If paracentesis has to be repeated several times, insertion of a TC becomes less costly and more convenient for the patient, whereas paracentesis would be a reasonable choice for patients with a very short life expectancy.10,11 Therefore, defining factors associated with shortly approaching death after a therapeutic procedure for MA are important for appropriate decision-making.
Paracenteses or insertions of TCs are frequently performed in inpatients, although these procedures might be done at outpatient clinics as well. 4 However, these procedures are mainly performed by radiologists or surgeons, while the successes or complications of TC insertions or paracenteses in palliative care units are infrequently reported.12,13 Concerns about rapid large-volume removal of ascites fluid still exist, although there seems to be no increase in complication rates. 14 In addition, the need for intravenous albumin or other fluids remains unclear.15,16
We evaluated the success, complications, and survival after paracenteses and insertions of TCs in an outpatient palliative care clinic on a day-case basis for the management of MA.
Methods
The paracenteses and insertions of TCs due to MA at the Palliative Care Unit of Tampere University Hospital between January 2013 and December 2015 were evaluated. Procedures performed in the outpatient clinic and those identified by the procedure codes marked in the electronic patient records were included into the analysis. However, all procedures performed in each patient were manually searched from the medical records, including those performed before and after the study period and those performed without the procedure code (e.g., procedures performed in other units), to describe the need for a repeated procedure and the number of procedures needed before insertion of a TC.
This study was approved by the Regional Ethics Committee of Tampere University Hospital, Finland (approval code R16071).
Procedures
All the procedures were performed on a day-case basis by a physician working in the palliative care outpatient clinic. None of the physicians were radiologists or surgeons, but they had experience in palliative care. The decision to perform a procedure and the choice between paracentesis and TC were made by the attending physician complying with the preferences of the patient. The largest locule of ascites fluid and the optimal site for the procedure were identified by using ultrasound. Subcutaneously injected 1% lidocaine was used for local anesthesia at the sites of incisions and for the subcutaneous tunnel area of the TC.
Paracentesis was performed with an 8.5F drainage catheter (Non-Locking Drainage Catheter, ReSolve; Merit Medical Systems, Inc., South Jordan, UT). After inserting the catheter into the peritoneal cavity, the inner needle was removed and the catheter was connected to a collecting bag. Free drainage of the ascites fluid was allowed without clamping of the catheter. The catheter was removed upon discharge of the patient.
An intraperitoneal TC was inserted with the PleurX catheter system (PleurX; Becton, Dickinson and Company, NJ). The manufacturer's instructions were followed, and a standard technique was used for insertion. 17 In brief, the 15.5F fenestrated catheter was tunneled subcutaneously and then inserted into the peritoneal cavity using a 16F introducer passed over the guidewire, which was first inserted with the Seldinger technique. Initial large-volume drainage was performed in the outpatient clinic and management instructions of the TC were given to the patients or their caregivers. Drainage was first advised for each day and then as required for symptom relief. Prophylactic antibiotics (oral cephalexin) were prescribed for five to seven days.
All patients were followed for one to eight hours depending on the symptoms and time needed for drainage. The outpatient clinic is supplied with beds to allow patients to rest in the supine position. Albumin or other intravenous fluids were not routinely administered, but could be used at the decision of the physician.
Data collection
A retrospective review of all the patient charts, including the notes of nurses, was performed. Data were collected regarding the patients' demographic characteristics, diagnoses, symptoms, oncologic therapies, and date of death. The indications, technical success (ascites fluid received), complications, symptoms or signs related to the procedure, supportive therapies (e.g., intravenous fluids), and volume of the ascites fluid drained were recorded for each procedure. Patients were followed until death or to the end of December 2016.
Statistical analyses
Descriptive statistics, such as percentages, medians, and interquartile ranges (IQRs), were used for the data of the demographic and procedure characteristics. Comparisons of categorical variables between the different groups were performed by the chi-square test. Cox proportional hazard regression analyses were used to evaluate the influence of procedure type, volume of removed ascites fluid, cancer type, and ongoing chemotherapy or not on age-adjusted survival time after the procedure. Two-sided p-values of less than 0.05 were accepted as statistically significant. Data analyses were performed by SPSS Statistics, version 23.0.
Results
Patients and procedures
A total of 166 procedures (118 paracenteses and 48 TCs) performed in 104 patients were analyzed. The patient and procedure characteristics are presented in Table 1. Two patients (2%) were alive at the end of December 2016, and all the other patients were followed up until death. The patients came to the outpatient clinic from home and from hospital wards in 148 (89%) and 14 (13%) of the cases, respectively. Three patients came from a nursing home and one came from hospice.
Head and neck, renal, duodenal, and esophageal.
Data missing in one patient.
TC, tunneled catheter.
All the procedures were technically successful in terms of removing ascites fluid. The median volume of removed ascites fluid was 3700 mL (range 300–13,200 mL), and over 5000 mL and 10,000 mL were removed in 42(25%) and 5 (3%) of the procedures, respectively. In one procedure, information regarding the final volume of removed fluid was missing. Three (2%) patients received intravenous fluids (two albumin and one sodium chloride solution).
Symptoms related to MA and necessitating the procedure are given in Table 2. The majority of patients (94%) felt unspecified discomfort, whereas about one-third suffered from pain. In seven cases (4%), the symptoms were not recorded.
Repeated procedures
A repeat procedure for ascites was needed after paracentesis in 64% and after insertion of a TC in 10% of the cases (p < 0.001). The median time to the next procedure after paracentesis was 14 days (IQR: 8–22). Paracentesis before insertion of a TC was performed in 39 (81%) of the patients with TCs, and more than one paracentesis was required in 22 (46%) cases.
Complications
Complications of the procedures are presented in Table 3. Complications occurred in 8 (7%) and 12 (25%) of paracenteses and insertions of TCs, respectively. Two complications were reported after one and three after another insertion of TCs. Two patients suffered from hypotension (removed ascites fluid 3550 mL and 9400 mL), which subsided with intravenous fluids without renal impairment. One patient was discharged on the same day and the other patient stayed at the hospital for two days. Two patients had peritonitis due to the TC. One patient stayed at the hospital for six days, recovering with antibiotics and removal of the TC. The other patient was already admitted to the hospital for end-of-life care. The catheter was left in place, but her symptoms improved with antibiotics. One patient with fulminant liver metastases died five days after paracentesis (removed ascites fluid 4100 mL) due to liver failure and unspecified infection, but bacterial cultures from ascites fluid were negative. The cause of death was reported to be progression of the metastatic cancer. One patient had minor bleeding from the paracentesis wound. The patient was observed over one night at the hospital, but no transfusions were needed. Six patients reported prolonged leakage of ascites fluid, which ended spontaneously. None of the complications were clearly associated with patients' death.
Dislodgment of the guiding wire.
Bleeding.
Survival after the procedure
The median survival after the first procedure of the patient was 40 days (IQR: 17–115) and after all the procedures was 43 days (IQR: 18–139). The age-adjusted survival according to different factors is presented in Figure 1. Pancreatic cancer was associated with shorter median survival (19 days; IQR: 9–35) after the first procedure compared with colorectal (51 days; IQR: 24–133), breast (43 days; IQR: 19–129), and other (48 days; IQR: 21–186) cancers. Patients who received chemotherapy had better median survival (112 days; IQR: 43–205) than patients without ongoing chemotherapy (25 days; IQR: 14–52). The procedure type or volume of removed ascites fluid did not have any influence on survival after the procedures (Fig. 1A, B).
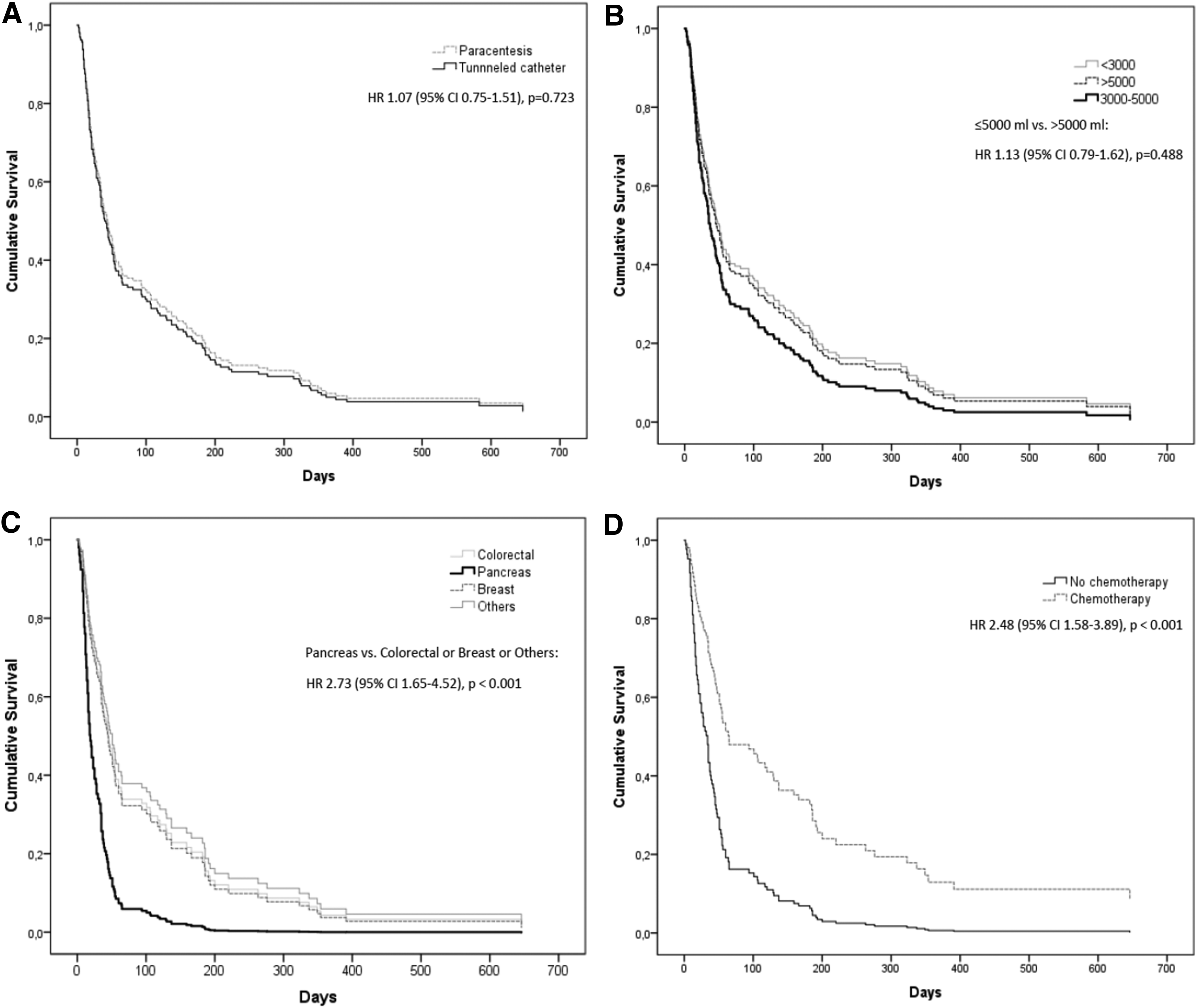
Age-adjusted survival after all the procedures according to the procedure type
Discussion
Our study shows that paracentesis and the insertion of a TC for MA can be safely performed in an outpatient clinic by palliative care physicians. Paracentesis had to be repeated in approximately two-thirds of the patients, whereas additional procedures after the insertion of a TC were relatively uncommon. The volume of the removed ascites fluid was not associated with increased mortality, but patients with pancreatic cancer and those without ongoing chemotherapy had a poor survival rate.
The treatment of MA is mostly reported from radiological and surgical units especially concerning the insertion of a TC.18–20 In this study, both paracenteses and insertions of TCs performed in an outpatient palliative care unit were technically successful, and major complications were rare. The complication rate in previous studies ranged from 0% to 8% for paracentesis and from 8% to 56% for insertion of a PleurX TC. 12 These numbers are in line with our results showing overall complication rates of 7% and 25% for paracentesis and TC, respectively. However, the majority of complications reported in our and in other studies are minor, and some of them (e.g., leakage of the ascites fluid for couple of days) could be considered normal consequences of the procedure. Some of our patients were in a poor clinical condition and died shortly after the procedures. However, none of the complications were clearly associated with patient's death. In our institution, the insertion of a TC was associated with somewhat more inconvenience and minor complications than paracentesis, but patients had similar survival after both procedures. Therefore, the choice between these two procedures should be mainly driven by the preferences of the patient, the need for additional procedures, and the expected survival.
Although paracentesis is a simple procedure offering a rapid and good symptom relief for MA, repeated paracenteses are frequently needed within approximately two weeks. 9 Our study is in line with the previous studies as we showed that paracentesis had to be repeated in 64% of the cases in a median of 14 days, whereas the insertion of a TC offered a permanent solution for MA in 90% of the cases. If paracentesis needs to be repeated several times, insertion of a TC is shown to be more cost-effective, especially if the paracenteses are performed in an inpatient setting.10,11 In addition, repeated paracenteses pose a risk for uncommon, but potential, complications and repeated hospitalizations, lowering the quality of the patient's life. Therefore, early insertion of a TC is probably the most convenient therapeutic option for majority of patients with MA, excluding those with very short life expectancy. This fact is especially true for patients living in rural areas, which is the case in many parts of Finland.
The median survival of a patient with refractory MA is reported to be about one to three months, although ovarian cancer is associated with longer life expectancy.2,4,5,21 These survival times are similar to those found in our study, which included only two patients with gynecological malignancies. In previous studies, impaired prognosis among patients with MA is associated with a low serum albumin level, transudative ascites fluid, liver metastases, no ongoing chemotherapy, presence of edema, and nonovarian malignancy.1,21,22 When considering whether to perform simple paracentesis or to insert a TC, it would be valuable to define patients with a very short survival time (e.g., < one month). The median survival of patients with pancreatic cancer was only 19 days in our study, which was significantly lower than the median survival in other cancer groups. In some previous studies, pancreatic cancer was included in the group of GI cancers, avoiding description of the prognosis of these patients separately. 13 According to our results, MA in a patient with pancreatic cancer could be treated with simple paracentesis at least if the patient is in a poor clinical condition and if repeated paracenteses are easily available when needed. Patients with ongoing chemotherapy had longer survival times compared with patients without it in our study, which is consistent with findings of the study by Ayantunde and Parsons. 1 However, it is very likely that the patients on chemotherapy had also better performance status, which could partially explain the longer survival. The need for therapeutic procedures for MA is nevertheless a trigger that should lead to end-of-life care planning especially in patients with pancreatic cancer and patients without chemotherapy.
Concerns regarding hemodynamic disturbances due to rapid large-volume removal of ascites fluid still exist, although free drainage has been safe in some studies.12,16,23 In our study, over 5 L of ascites was removed in 25% of the patients with no clear association with complications or survival. In addition, intravenous albumin was given to only two patients in our study, whereas in a recent study by Gu et al., all the patients received albumin substitution during removal of MA. 13 Although there are some differences between the present study and the study by Gu et al., the complications and survival (43 vs. 36 days) after the procedure were similar. Safe removal of MA without the use of albumin has been reported also in some other studies.12,15,16 We suggest that in contrast to the removal of ascites due to cirrhosis, free drainage without the routine use of intravenous albumin seems to be a feasible therapeutic procedure for patients with MA and no liver insufficiency, although no randomized trials exist on this issue.12,15,16,24
Our retrospective analysis is limited to symptoms and background factors of the patients as well as the complications of procedures reported in patient records. We suggest that all of the significant complications were found because the procedures and their outcomes were carefully marked. In contrast, some valuable background factors such as performance status of the patient were not reported. The improvement in symptoms after removal of ascites was not uniformly reported, which prevented us from describing the success of procedures used to relieve symptoms. The decision of whether to use paracentesis or a TC was made by the physician in our study. Therefore, randomized studies with prospective evaluations of benefits and harms of each procedure are needed to fully describe the optimal treatment for MA.
Conclusions
Drainage of MA without upper limits of the removed volume seems feasible in an outpatient clinic. For majority of patients with MA, early insertion of a TC is reasonable to avoid the inconvenience and costs of repeated paracenteses. However, in patients with very poor survival, such as those with pancreatic cancer, the use of simple paracentesis might be an alternative to a TC, at least if repeated paracenteses are easily arranged.
Footnotes
Author Disclosure Statement
V.V.S. has received lecture fees from Grex Medical. Other authors have no competing financial interests.