
Abstract
Abstract
Background:
When attempting to share information about comfort-oriented care, many use “palliative,” “supportive,” and “hospice” care terminology interchangeably, but we lack evidence about the effects of using these different terms.
Objectives:
This study was designed to test whether the use of “palliative,” “supportive,” or “hospice” terminology can improve the dissemination of information among breast cancer patients—a large and growing oncology population.
Design, Setting, and Measurement:
This experimental study was conducted at a major U.S. hospital serving a diverse population. Patients visiting a cancer clinic encountered opportunities to learn more about cancer care. They were offered health materials that were described as reporting on “palliative,” “supportive,” or “hospice” care and the primary outcome was whether a patient decided to select or reject each. As a secondary outcome, the study measured the patient's level of interest in receiving each.
Results:
Compared with alternatives, materials labeled as “supportive” care were most likely to be selected and considered valuable (p value <0.01).
Conclusions:
In this study, the terminology used had a large effect and, compared with alternatives, the information labeled as being about “supportive” care was significantly more likely to be selected. If these effects are supported by additional research, there may be low-cost, highly feasible changes in language choice that increase the dissemination of relevant health information.
Introduction
I
When attempting to share information, the American medical community often uses “palliative” and “supportive” care terminology interchangeably. Sometimes, comfort-oriented care is also denoted by the term “hospice” care. Technically, these terms are not the same, despite considerable overlap in services. Because few patients are aware of technical distinctions, the effects of using these three different terms have been debated.17–20 Their actual effects on patients are not known.
This study was designed to test which term should be used when the goal is to increase the dissemination of information through mass media news coverage. Health reporting by the news media has the potential to reach millions on a daily basis, and the news media often use the terms synonymously, but these terms may have different effects on information dissemination. 13 Therefore, we tested whether the term used to label a news report had the same effects on patients.
The study was conducted among patients with cancer because the benefits of comfort-oriented care have been well documented for these populations. This type of care is particularly effective at improving their quality of life. 12 It also reduces medical costs among oncology patients, which generally incur the highest per-person cost for all diseases.21,22
Patients with breast cancer, specifically, were enrolled because this disease is commonly diagnosed and these patients have a wide range in their current health status, allowing recruitment of those who are early stage, as well as those who are late stage. This range is ideal for this study because the Institute of Medicine (IOM) and others stress the need to enroll patients from across the cancer continuum, with the goal of broadly improving communication about comfort-oriented care.12–16 Information about this care is potentially relevant across this spectrum, and it is recommended that attempts to communicate should not be limited to those with advanced cancer. 12
In addition, breast cancer receives more funding than other kinds of cancer, 23 meaning that the findings can inform interventions to improve communication with this large population. Compared with other cancers, breast cancer is also mostly commonly discussed by the news media,24–26 making it important to learn which terms should be used when attempting to disseminate information. It has been argued that the dissemination must be increased to meet this population's substantial informational needs.27–29
Methods
Study design, population, and setting
An experimental design tested whether the three terms used to label health materials influence the likelihood that patients will select or reject the material. Women with any stage of cancer, who were at least 21 years old, were recruited from a breast cancer clinic at a large, urban hospital serving a demographically diverse population. The clinic serves early stage and late-stage cancer patients, and, therefore, allowed the study to enroll patients across this spectrum. In keeping with the mentioned IOM recommendations for communication research that is broadly relevant across this spectrum, the study was designed to include patients at any stage, because they have the potential to benefit from the health information currently, and in the future. 12 For example, although hospice care enrollment is appropriate for those with advanced disease, the IOM has highlighted the importance of educating oncology patients early, regardless of their cancer stage, to increase their knowledge.
Study procedures
Study procedures were approved by the behavioral science committee of the University of Pennsylvania Institutional Review Boards, and also the Abramson Cancer Center. Eligible patients were identified by their Cancer Center clinic records and then approached consecutively at this clinic before their scheduled appointment to determine whether they were interested in study participation. When patients were approached for potential enrollment, the research objective was not revealed in case it could bias the patient's responses once enrolled, or even influence the patient's decision to enroll. To conceal the study's objective, the research assistant stated that the goal was to better understand patients' daily media habits for entertainment and news. (Patients were asked to share information about their media use. Because these data were actually not relevant to the analyses, they are not reported.)
At the end of the brief interview, patients were told that, to thank them for their study participation, they were being offered various news articles addressing health issues that may be of interest to them. They were told that copies would be available to take home and review at their leisure. In a randomly determined order, the trained research assistant mentioned the available selection. The research assistant described the three news articles as focusing on how “palliative care,” “supportive care,” or “hospice care” helps cancer patients.
Patients decided to reject or select each news article, which was the primary outcome. The research assistant did not inform them that their decision to select or reject each article was being investigated. As a secondary outcome, patients were asked to rate how much they wanted each article. These data were collected using a validated Likert scale ranging from 0 to 10, descriptively anchored with 0 = not at all, 3 = slightly want it, 6 = want it quite a bit, and 9 = extremely desired.30,31 At the conclusion of the interview, the patient received the requested articles. (Since the contents of each article were not visible to the patients earlier, it could not influence the study outcomes.)
This study tests the relative effects of each term within the same patients because, in many real-world settings, a patient can encounter information related to each of the three terms simultaneously, or in close succession. For example, when searching online for cancer care, links related to each term will appear among the search results, allowing the patient to choose some, none, or all. The search results typically do not highlight definitions, or the degree to which these terms differ. Similarly, in our study, the terms were not defined.
Analyses
The primary analysis compared the likelihood that each type of news article was selected. After computing the summary statistics for selection, McNemar tests were used to formally compare, within the same study subject, the selection of “supportive” versus “palliative” information and “hospice” versus “palliative” information.
The secondary analyses used nonparametric paired Wilcoxon signed rank tests to compare the difference in how much each patient reported wanting the information associated with each of the three terms, as measured by Likert scales. Owing to the lack of observed normality in the data distribution, which was confirmed using the Shapiro–Wilk test, this type of test was chosen over the traditional paired t-test. Box plots were also created to get a visual representation of the level of interest patients reported for each term. A Bonferroni correction-adjusted p value of 0.0125 was used to determine statistical significance.
Results
A total of 122 patients were approached and 89 women decided to participate in this study. (Two, who did not complete the study due to time constraints, were excluded from the final analyses.) The mean age at the time of interview was 56 years old, with most patients ranging in age from 54 to 59. Representing the study population's wide range in health status, the sample included patients who were relatively sick or healthy. About one-third of the patients included in this study had stage I cancer, and were undergoing treatment. Among all patients, another third had stage IV cancer, with the remaining third was characterized by stages in between. The sample was also diverse in other ways, reflecting a range of socioeconomic status and different races, as Table 1 summarizes.
Data based on clinic charts.
Among the sample of 87 patients, 29 (33.3%) selected all three articles, 32 (36.8%) selected two articles, 17 (19.5%) choose only one article, and 9 (10.3%) selected none at all. The vast majority of patients (71/87 or 81.6%) selected the information about “supportive” care, making it the most likely type of information to be chosen. In contrast, less than half of the patients (42/87 or 48.3%) selected the “hospice” care information and slightly more than half of the patients (55/87 or 63.2%) selected the “palliative” care information available.
As Table 2 summarizes, 4.7% of patients (4/87) selected “palliative” and not “supportive” information, 22.1% of patients (19/87) selected “supportive” and not “palliative” information, 59.3% of patients (51/87) selected both, and 13.9% of patients (12/87) selected neither. These differences in article selection generated a statistically significant p value of 0.002 (as shown in Table 3). In addition, the level of interest that patients reported in receiving the “supportive” care information was shown to be significantly greater than the interest they reported in receiving the “palliative” care information (Wilcoxon sign rank test, p value = 0.002). More specifically, 31% of patients (27/87) selected the same Likert value for both news stories, 43% of patients (37/87) wanted “supportive” care information more than “palliative,” and 25% of patients (22/87) wanted “palliative” care information more than “supportive.”
IQR, interquartile range
As Table 2 documents, 27.9% of patients (24/87) selected “palliative” and not “hospice” information, 12.8% (11/87) selected “hospice” and not “palliative” information, 36.1% (31/87) selected both, and 23.2% (20/87) selected neither. These differences produced a McNemar p value of 0.028, which indicates a lack of statistical significant difference at the adjusted 0.0125 level. Among those who did request each type of information, the level of interest that patients reported for the “palliative” care information was also not significantly different from the levels of interest that they reported for the “hospice” care information (Wilcoxon sign rank test, p value = 0.059). In addition, we observed that there were 36/87 subjects who selected the same Likert value for both sets of information, 32/87 subjects who wanted “palliative” information more than “hospice,” and 18/87 subjects who wanted information about “hospice” more than “palliative” care.
Figure 1 summarizes how patients reported different levels of interest in receiving each article, which was the secondary outcome. Compared with the information labeled “palliative” or “hospice care,” patients reported substantially more interest in “supportive” care information, as indicated by higher mean and median values. The “supportive” care information also generated a narrower and more concentrated interquartile range (IQR). Ratings of interest in “supportive” care information produced a mean score of 5.8 (95% CI [5.1–6.5]), with a median score of 7 on the 0–10 scale. When reporting their level of interest in information about “palliative” care, patients reported a mean score of 4.4 (95% CI [3.6–5.3]), with a median score of 5. When patients were offered information about “hospice” care, their levels of interest generated a mean score of 3.4 (95% CI [2.6–4.3]), with a median score of 0.
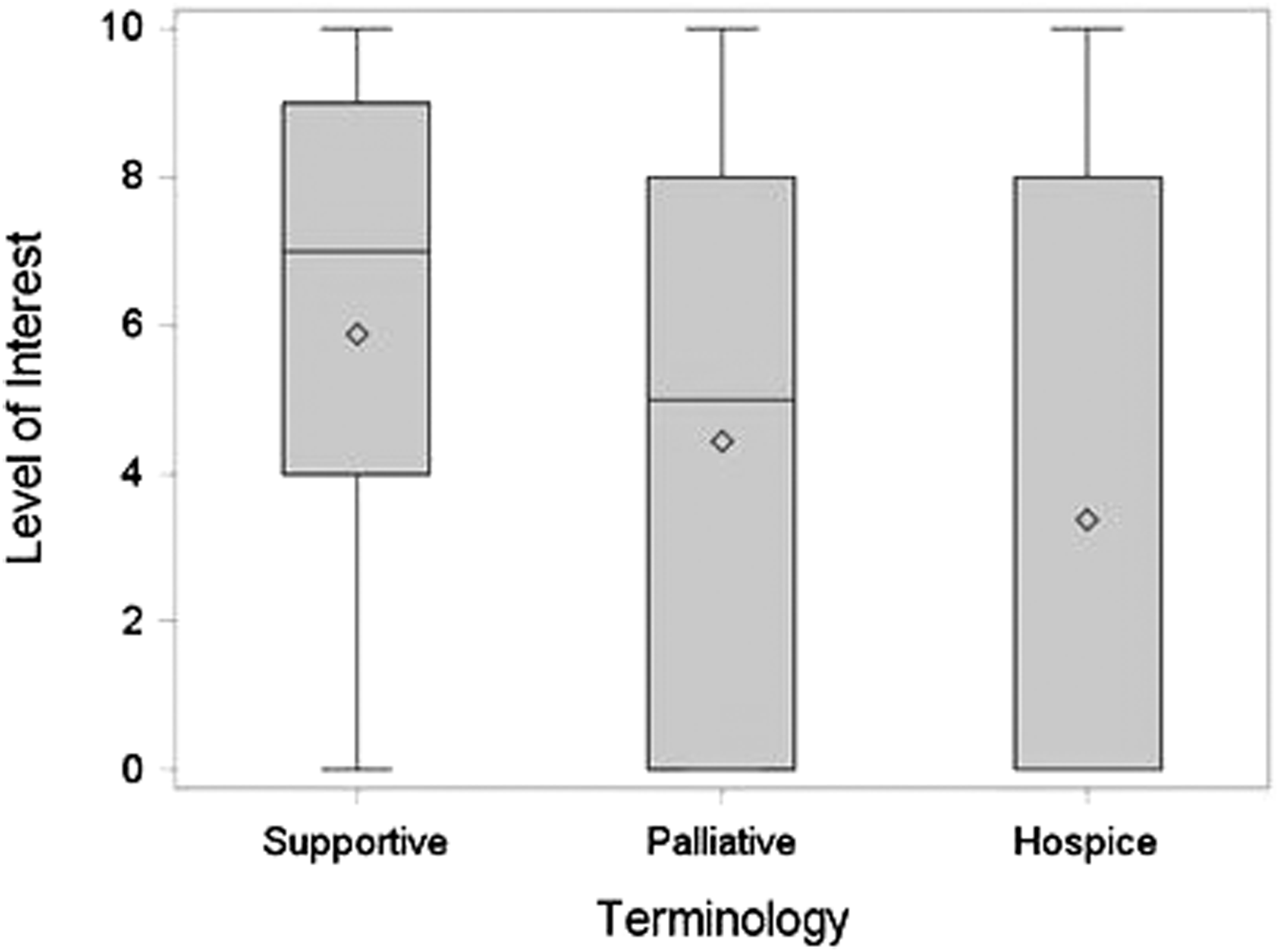
Patients' level of interest for each term. The diamonds represent the mean values. Horizontal bars represent median values. The bar for the “hospice” median value is visually undetectable because it occurs at zero. (Mean, median, and interquartile range (IQR) ratings are on a 0–10 scale.)
Conclusions
This study was designed to test whether health information was more likely to disseminate when labeled with “palliative,” “supportive,” or “hospice” care terminology. Although these terms are commonly used interchangeably, the study findings suggest that they have different effects. By a wide margin, information about “supportive” care was most likely to be selected by patients.
To our knowledge, this is the first study testing whether these terms effect the dissemination of information. Dissemination is an important study outcome because it limits the degree to which information can inform knowledge and beliefs, and influence decision making. This dissemination test used news articles because the news industry serves millions, and even small mass media effects can have profound public health consequences. 32 The news commonly uses each of the three terms synonymously when reporting on cancer care, but based on the current findings, there may be immediate opportunities to improve communication by modifying the term used.
Despite the ways in which this study is novel, the current findings are generally consistent with others. Maciasz et al. telephoned patients who listened to educational text that described “palliative care” or “supportive care.” They found that the latter term is associated with more favorable impressions of the services involved. 33 Oncologists may also respond more favorably to “supportive” care terminology than to “palliative” care terminology.18,34,35 The evidence collectively suggests that the name matters.
Study limitations
This study has several important limitations. This study was designed to test effects for the sample overall. Since the news media do not currently tailor the language used in their health reporting according to audience characteristics such as age or cancer stage, we did not design the study to test the effects of potential tailoring for subgroups. However, in exploratory tests, there were no significant differences by subgroups. If the goal is to learn how communication should be tailored for various subgroups, future studies should be powered specifically for the comparison of interest.
For reasons discussed earlier, this study was designed to enroll cancer patients, and the results may not be generalizable to other patients. It was designed to specifically study women with breast cancer, for reasons that were also discussed, and future research should enroll other cancer populations. In addition, given that this study was conducted in a single clinic, future tests should include other clinics, as well as nonclinic settings. The effects may be moderated by different settings. Different study designs are also welcome.
In conclusion, it is important to help patients gain information about evidence-based care.1–4 Prior studies have documented myths and gaps in knowledge, and called for improved cancer communication.12–14,36 In this study, the term “supportive care” increased the chance that health information would disseminate, suggesting that a simple change in language may be a low-cost way to improve communication.
Footnotes
Acknowledgment
This study was supported by American Cancer Society grant MRSGT-08-013-01-CPPB.
Author Disclosure Statement
No competing financial interests exist.