
Abstract
Abstract
Background:
Many older adults live with serious illness for years before their death. Nurse-led primary palliative care could improve their quality of life and ability to stay in their community.
Objectives:
To assess feasibility and acceptability of a nurse-led Transitional Palliative Care (TPC) program for older adults with serious illness.
Methods:
The study was a pilot trial of the TPC program in which registered nurses assisted patients with symptom management, communication with care providers, and advance care planning. Forty-one older adults with chronic conditions were enrolled in TPC or standard care groups. Feasibility was assessed through enrollment and attrition rates and degree of intervention execution. Acceptability was assessed through surveys and exit interviews with participants and intervention nurses.
Results:
Enrollment rate for those approached was 68%, and completion rate for those enrolled was 71%. The TPC group found the intervention acceptable and helpful and was more satisfied with care received than the control group. However, one-third of participants perceived that TPC was more than they needed, despite the number of symptoms they experienced and the burdensomeness of their symptoms. More than half of the participants had little to no difficulty participating in daily activities.
Conclusion:
This study demonstrated that the nurse-led TPC program is feasible, acceptable, and perceived as helpful. However, further refinement is needed in selection criteria to identify the population who would most benefit from primary palliative care before future test of the efficacy of this intervention.
Introduction
O
A potential solution to these constraints is providing “primary” or generalist palliative care by nonpalliative care specialists.20,21 Registered nurses form the largest workforce in healthcare and are present at the point of care for many patients. Nurse-led care coordination programs have shown success assisting patients and their families to better manage their health in the community where they live.22–24 Primary palliative care competencies such as basic symptom management, patient-centered holistic care, and effective communication are fundamental competencies expected for all registered nurses. 25 Registered nurses may be ideal candidates to deliver primary palliative care to older adults with multiple chronic conditions. 26
We developed a nurse-led Transitional Palliative Care (TPC) program to provide primary palliative care to community-living older adults with multiple chronic conditions and conducted a pilot study to assess the feasibility and acceptability of the TPC program. In this article, we describe the findings from the study, as well as challenges and lessons learned.
Methods
Study design
We conducted a single-site, two-arm active-control pilot study to assess the feasibility and acceptability of the TPC program. Because the primary focus of this pilot study was to test feasibility, we did not use random group assignment.27,28
Participants and setting
The target population was older adults with serious illness as indicated by multiple chronic conditions. We identified the time of transition from hospital to home as a high-risk, high-needs entry point for nurses to intervene. Patients meeting the following criteria were identified and recruited from an academic healthcare center in Oregon: age ≥55; more than one qualifying diagnosis (e.g., congestive heart failure, coronary artery disease, ischemic heart disease, vascular-related diagnosis, chronic obstructive pulmonary disease, and chronic renal failure); expected to stay in the hospital for >72 hours; >1 hospital admission within last 12 months; expected to be discharged home; enrolled in Medicare Parts A and B; and lived within 30 miles of the hospital. We excluded patients who were not able to communicate in English, had cognitive impairment (Mini-Cog™: Word recall = 0 or abnormal clock drawing), enrolled in hospice or palliative care services, or were scheduled to receive home health nurse visits. A research assistant identified patients meeting inclusion criteria through daily chart review and approached them to screen and invite them to the study. The study was approved by the Institutional Review Board of Oregon Health and Science University.
Intervention
Standard transitional care (control group)
Usual treatment received by the control group was standard transitional care that included a home visit by a community-based Transition Coach within 7 days of discharge from the hospital and up to three telephone visits within 30 days of discharge. Transition Coaches were hired by local counties' Aging and Disability Services Offices. Transition Coaches were nonclinicians who were trained to provide transition care services outlined in Coleman's Care Transitions program (http://caretransitions.org) focusing on patient engagement in self-care. They identified Medicare patients scheduled for discharge from hospital to home and assisted them through transitions.
TPC (intervention group)
Patients assigned to the intervention group received TPC in addition to the standard transitional care described above. The draft of protocol for the TPC program was developed based on literature from palliative care, gerontological nursing, and transitional care. We conducted four focus groups and 14 individual interviews with local palliative care providers (n = 11), geriatricians (n = 4), and transitional care nurses (n = 11) to evaluate and refine the protocol. Essential components of the TPC program were registered nurses who would visit participants at least once in the hospital, at home within three days after hospital discharge, and initiate three weekly and two monthly telephone visits during the three-month postdischarge intervention period. The primary purposes of the hospital visits were TPC nurses getting to know patients and establishing rapport and assessing and working with patients to prepare for discharge. The postdischarge visits were to (1) assess and address patients' needs to manage their health at home, (2) assist patients to manage symptoms, (3) assist patients to navigate and communicate with healthcare providers, and (4) facilitate advance care planning conversations with patients and their family.
Interventionist training
Two registered nurses were hired as interventionists and trained to provide primary palliative care using the TPC intervention protocol that was developed through expert reviews described above. Basic symptom management and communication skills are core competencies required in prelicensure nursing education. 29 Both TPC nurses had baccalaureate degrees in nursing and 2–3 years of experience working as a registered nurse in primary care settings. Neither had prior training in palliative or hospice care specialties. The principal investigator (S.I.) provided four two-hour training sessions (total of eight hours) about the TPC intervention. Training included best practices in transitional care (Coleman's Care Transition Program, 30 Naylor's Transitional Care Program, 31 BOOST 32 ), complex medication management,33–36 and palliative care principles,10,37 particularly symptom management in the geriatric population. 37 In addition, the nurses received Respecting Choices® First Step Advance Care Planning Facilitator Training from a certified trainer that includes four online modules and an eight-hour face-to-face training. 38 TPC nurses' competency to facilitate advance care planning conversation was evaluated using role-play criteria that was part of the Respecting Choices training program.
Assessment of feasibility and acceptability
Feasibility of recruitment and retention was assessed through recruitment, enrollment, and completion rates, as well as reasons for nonenrollment or attrition. Feasibility and acceptability of TPC were assessed by monitoring intervention fidelity of TPC visits. All visits were audio-recorded with permission from the participants, and the principal investigator (PI) reviewed 25% of the recordings for content and quality. 39 In addition, we conducted exit telephone interviews and asked participants in both groups about their satisfaction using an Experience with Care Survey and what worked well and challenges using a semistructured interview guide. We conducted group interviews with TPC nurses and 10 Transition Coaches who were involved with the study participants to assess their experience with and acceptability of the TPC intervention. Patient outcome data were collected to assess feasibility of data collection methods. Patient outcomes included health service utilization; number of symptoms and symptom burden using Memorial Symptom Assessment Scale Global Distress Index (MSAS-GDI)40,41; physical function and ability to participate in social function using Patient-Reported Outcomes Measurement Information System (PROMIS) Short Form at one-, two-, and three months after discharge from the index hospitalization; and advance care planning conversations with their families.
Data analysis
We used descriptive statistics to summarize quantitative data using SAS version 9.2 (Cary, NC). We used Wilcoxon rank-sum tests to compare participant care satisfaction and evaluation. p-values less than 0.05 were considered statistically significant. Responses to the open-ended questions from the exit interviews and field notes from the group interviews with TPC nurses and Transition Coaches were reviewed by two investigators (S.I., B.B.) to extract descriptions of what did or did not work well and what was most and least helpful from patients' and interventionists' perspectives using qualitative description approach. 42
Results
Recruitment, enrollment, and retention
A total of 179 potential participants meeting inclusion criteria were identified between January 12 and June 30, 2015 (Fig. 1). Sixty-six patients were discharged before researchers approached them, and 53 met exclusion criteria. Among the 60 patients approached by researchers, 41 agreed to enroll (enrolled-to-approached rate 68%). Because early enrollment rate was low, and the primary purpose of the study was to test the feasibility of the TPC intervention, initially we assigned all participants to the TPC group until we had enough to evaluate the intervention. After 15 patients were assigned to the intervention group, we randomly assigned all remaining participants to control or intervention group in a 4:1 ratio. Twenty patients were enrolled in the intervention group and 21 in the control group.
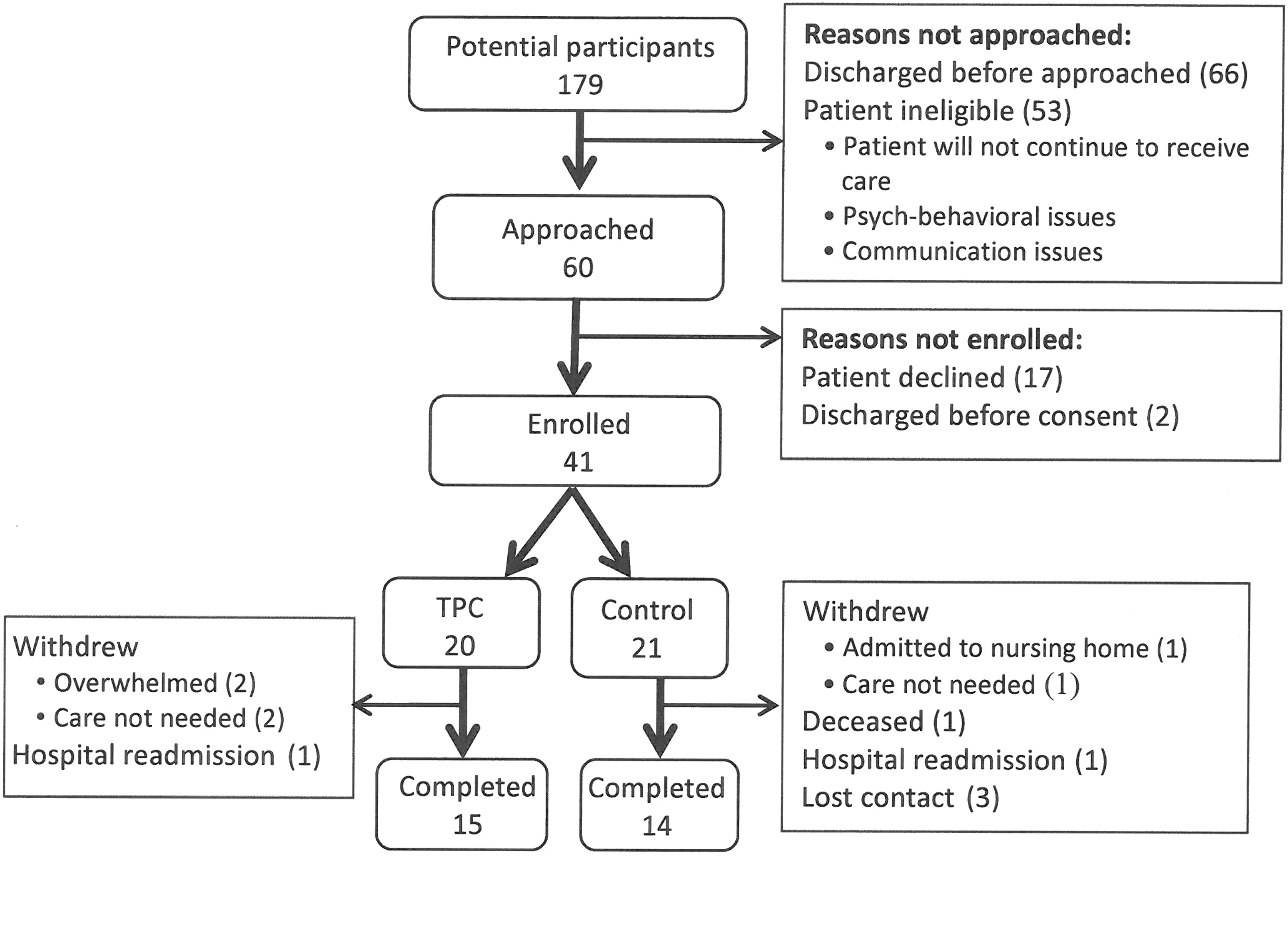
Enrollment diagram.
In the intervention group, four participants withdrew before receiving a home visit by a TPC nurse. Two stated that they were overwhelmed after hospital discharge, and having a TPC nurse visit was felt to be a burden. The other two withdrew because they were doing well and believed that a home visit by a TPC nurse was not needed. One participant in the intervention group was readmitted to a hospital six weeks after hospital discharge. In the control group, two participants withdrew because one was admitted to a skilled nursing facility the first week after discharge and another declined a home visit by a Transition Coach as not needed. One participant died eight weeks after discharge, and one participant was readmitted to hospital. We lost contact with three participants in the first month; our retention rate was 70.7%.
Participant characteristics
Demographic information and characteristics of all participants are presented in Table 1. The typical participants were ∼70 years and white with variety of diagnosis for the hospitalization.
Some participants had more than one primary diagnosis at admission.
COPD, chronic obstructive pulmonary disease; IQR, interquartile range; TPC, Transitional Palliative Care.
Intervention fidelity
The TPC intervention was delivered following the intervention protocol. The mean length of a TPC visit in the hospital was 39 (SD = ± 29) minutes. The mean length of TPC home visits was 87.8 (SD = ± 27.5) minutes, not including travel time. The home visit was followed by five telephone visits (three weekly, then two monthly) by the same TPC nurse. The mean total telephone visit time per participant was 103 (SD = ± 51) minutes. Length of each telephone visit was 5–58 minutes depending on participant's needs and availability.
The TPC intervention was delivered 99% of the time; one participant missed the last telephone visit due to her travel schedule. The majority (91%) of telephone visits was conducted within 2 days of the scheduled date; eight telephone visits were delayed by 3–15 days due to participant availability. The TPC nurses could conduct additional home or telephone visits if they judged it was appropriate, but none was made. A TPC nurse had planned to make an extra home visit for a participant who had an exacerbation of shortness of breath with difficulty communicating on the telephone. However, the participant went to an emergency department (ED) and was readmitted to the hospital the night before the additional visit was scheduled.
Fidelity of intervention was rated on 25% of audio recordings of the visits. TPC nurses were compliant with the protocol 94% of time. Symptom management and communication components of the intervention were delivered 100% of time. Advance care planning was not discussed when patients expressed discomfort or refused.
Participant satisfaction, perception, and needs for palliative care
Compared to the control group, participants in the intervention group rated the care they received significantly higher in availability of TPC nurses and managing their illness. There were no statistically significant differences between the two groups in other aspects of care (Table 2).
p < 0.05.
TPN, transitional palliative care nurse.
In exit interviews, both groups stated that receiving additional information about medications, treatment, available community resources, and how to navigate the healthcare system was helpful. The intervention group appreciated that the TPC nurse tailored care to fit their individual needs and interests (Table 3). In contrast, some participants in the control group thought that a Transition Coach providing standardized procedures was not helpful. Participants in the intervention group liked to have someone to call to answer their questions. A few participants stated that they liked having “a nurse” to call because nurses could answer medical or medication questions. Although only two participants actually called TPC nurses, a participant stated, “I like just having a number to call if I had any questions … peace of mind,” and more than half of the intervention group made similar comments. Several participants in the control group stated that not having a number to call or not receiving regular follow-up visits were not helpful.
Not marked: Intervention group Not marked: TPC nurses.
Both intervention and control group coaches.
Control group.
Both TPC nurses and transition.
Committing time for visits was a challenge for both groups. Engaging in up to one-hour interactions with a nurse or a coach, especially when participants were still recovering from illness, was tiring for some. Another challenge raised by both groups was limited information about availability of community resources. Two participants said that they were uncomfortable talking about advance care planning because they thought it would scare their family or they did “not need it now.” Although two control group participants thought up to 30 days follow-up was not enough, about one-third of participants from both groups indicated that they were doing well and did not need services like the TPC or Transition Coach.
This input from participants led us to report the overall symptom burden and functional status as a marker of palliative care needs. The median number of symptoms the participants experienced was 6 (IQR = 3: Table 4), and ∼60% had more than five symptoms. The most common and burdensome symptoms were lack of energy, pain, and dry mouth. Not all symptoms were burdensome, but 40–60% of participants had at least one symptom that was quite a bit to very much burdensome (Fig. 2). However, more than half of participants never to rarely had trouble participating in social activities (Fig. 3), and more than 60% had no to little difficulty carrying out everyday chores (Fig. 4).
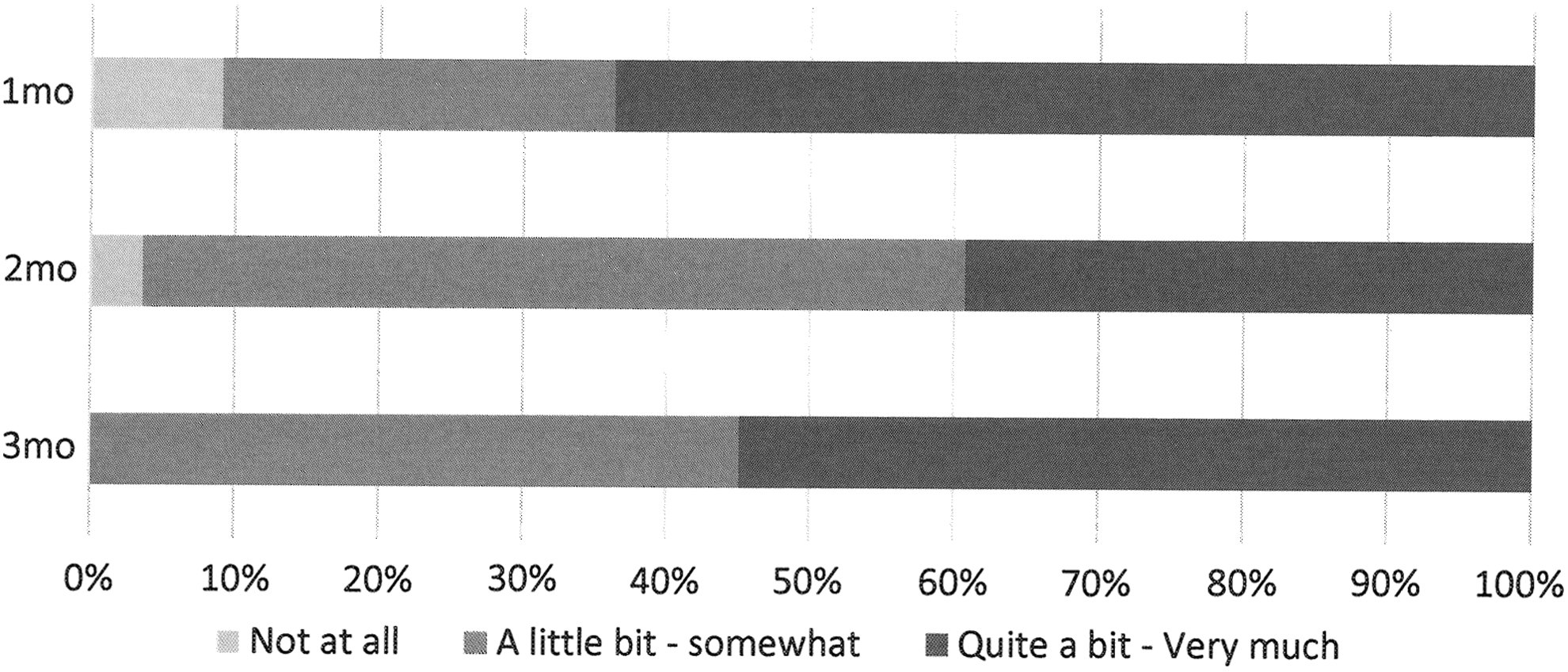
Percent of participants who experienced symptom burden (MSAS-DGI). MSAS-DGI is a patient-report instrument rating symptom distress (0–not at all; 4–very much) associated with 13 physical and psychologic symptoms during the past 7 days.40,41 MSAS-DGI, Memorial Symptom Assessment Scale Global Distress Index.

Percent of participants who had trouble participating in social roles and activities (PROMIS Ability to participate in social roles and activities Short Form 4a). PROMIS Ability to Participate in Social Roles and Activities Short Form 4a. PROMIS Ability to participate 4a asks how often (1–Always; 5–Never) they have trouble participating in social roles and activities (leisure activities with others, family activities, usual work, and activities with friends). PROMIS, Patient-Reported Outcomes Measurement Information System.

Percent of participants who had difficulty with everyday chores (PROMIS Physical Function Short Form 4a). PROMIS Physical Function Short Form 4a. PROMIS Physical Function 4a asks how difficult (1–Without any difficulty; 5–Unable to do) to do every day chore (vacuuming or yard work, use stairs, 15 minute walk, run errands, and shop).
MSAS-GDI is a patient-report instrument rating symptom distress (0–not at all: 4–very much) associated with six physical symptoms (lack of energy, pain, lack of appetite, feeling drowsy, constipation, and dry mouth) and frequency (0–never; 4–almost constantly) of four psychologic symptoms (sad, worry, irritable, and nervous) during the past 7 days.40,41 Because the MSAS-GDI was developed for patients with cancer, three additional physical symptoms (shortness of breath, difficulty sleeping, and swelling of arms or legs) that are common among older adults with noncancer chronic condition were added. Higher scores of MSAS-GDI indicate higher symptom burden.
MSAS-GDI, Memorial Symptom Assessment Scale Global Distress Index.
Interventionist perceptions
In interviews, the TPC nurses and Transition Coaches were asked what went well and the challenges (Table 3). The TPC nurses perceived that the hospital visit, seeing the same nurse, and having a telephone number to reach the nurse during transition were helpful for them to know the patient better and for patients to feel connected. They thought visit timing was generally adequate, yet more flexibility in timing of visits based on individual needs might improve efficiency of care. TPC nurses also identified challenges in communicating with patients' healthcare providers (e.g., “the team does not know me” and TPC nurses could not document in the patient health record) because TPC was not integrated in the patients' care team.
Discussion
This study demonstrated the feasibility and acceptability of the nurse-led intervention providing primary palliative care to older adults with multiple chronic conditions. However, some challenges were identified that could inform clinical trials to test the efficacy of this type of intervention.
Although identification of the appropriate target population is critical to evaluate the value of the intervention, it was challenging in this study. Despite the diagnosis of serious illness with multiple chronic conditions and more than one recent hospital admission, one-third of participants perceived that the intervention was more than they needed. Despite burdensome symptoms, the majority had little to no difficulties in their daily activities and did not perceive that they needed palliative care. Existing early palliative care trials have mostly targeted patients with cancer diagnosis with clear needs for palliative care.43–46 In contrast, illness trajectory and symptom presentations of older adults with multiple chronic conditions are complex and unpredictable, and their palliative care needs are not well defined. 44 Studies show that adding functional limitations to diagnosis of advanced stage illness increases sensitivity to identify population in need of palliative care.11,47 In our study, about half of the participants experienced burdensome symptoms, and ∼40% had some difficulties in their daily activities. Adding both functional limitation and existence of burdensome symptoms to eligibility criteria should be considered in future studies to identify patients most likely to benefit from primary palliative care.
Another challenge we faced was reaching potential subjects before they left the hospital. Even when we could reach patients before discharge, they were receiving discharge instructions and too overwhelmed to consider participating in the study. Development of a mechanism to identify and reach out to high-risk, high-needs patients sooner is needed to assure feasibility of similar interventions.
Although participants found that TPC was acceptable, the best intervention dose and contents remain uncertain. Authors of systematic reviews of transitional care models have concluded that effective interventions vary by target patients' needs.23,48 Given that some participants said they did not need 3 months while 30 days was not enough for others, 6–8 weeks of visits with flexibility might be appropriate for this population. The TPC group reported that the visits were helpful because they were tailored to their conditions and needs. However, nurses' ability to tailor their care to patient's needs is variable. TPC nurses expressed that management of diverse illness and symptom presentations was challenging. Further identification of specific primary palliative care nursing competencies and development of a training program to foster adequate competencies to standardize the intervention dose are needed.
Finally, TPC nurses in this study were hired for the research and externally added to existing patients' healthcare teams. Because close communication and care coordination across providers and settings are key for consistent and continuous care, 49 TPC nurses need to be recognized and integrated into existing patient care team.
This study has several important limitations. First, this was a small pilot study with limited statistical power. Second, the assignment of patients to intervention or control was not strictly randomized. In addition, ability to select specific target population, thus accurate descriptions of group characteristics, was limited due to the inaccuracy or incompletion of clinical health record we used. Finally, this study took place in one city and one healthcare institution, which may limit generalizability. Geographical location of the study site also resulted in lack of a racial and ethnic diversity of the participants. However, we were successful in piloting this intervention and addressing feasibility and acceptability.28,50
In summary, we describe feasibility and acceptability of a nurse-led primary palliative care intervention for community-living older adults with multiple chronic conditions. Rigorous testing of efficacy of this intervention is warranted for next step. The most critical challenge for a future efficacy study is the identification of specific target population that would most benefit from primary palliative care. Establishing the criteria to identify this population is urgent to advance evidence-based palliative care for the growing population of older adults with serious illness.
Footnotes
Acknowledgments
This study was funded by National Palliative Care Research Center Career Development Award (2013–2015). This study utilized OHSU REDCap which is supported by NIH (1UL1RR024140 01) for data collection and management. The authors thank the patients, family members, and clinicians for their participation in this study.
Author Disclosure Statement
No competing financial interests exist.