
Abstract
Abstract
Background:
Delirium in patients with terminal cancer is irreversible and increases treatment resistance, which leads to a deterioration in quality of life.
Objective:
To investigate factors affecting the effectiveness and safety of intravenous chlorpromazine for irreversible delirium in patients with terminal cancer.
Design/Measurements:
Multiple regression analysis for factors affecting treatment effectiveness was carried out based on a retrospective comparison between responders and nonresponders to intravenous chlorpromazine.
Setting/Subjects:
Ninety-seven patients with terminal cancer who were treated with intravenous chlorpromazine for irreversible delirium were included.
Results:
The rate of patients with ≥50% improvement in mean Nursing Delirium Screening Scale score from pretreatment to day three of chlorpromazine treatment was 0.48 (95% confidence interval [CI]: 0.38–0.58). Factors affecting chlorpromazine treatment effectiveness were hyperactive delirium (odds ratio [OR]: 6.25, 95% CI: 1.14–34.5) and longer survival (OR: 1.096, 95% CI: 1.05–1.14). The mean chlorpromazine dose was low, at 17.9 mg/day. Adverse events were reported in 11 patients (11.3%) by day three of chlorpromazine treatment, and all were observed in patients who survived less than two weeks after chlorpromazine treatment. Patients who died, who had decreased blood pressure during chlorpromazine administration, and who showed acute akathisia all displayed shock index ≥1.
Conclusions:
Intravenous administration of low-dose chlorpromazine may be an effective and safe treatment option for delirium in patients with terminal cancer who have hyperactive delirium, longer predictive prognosis, and shock index <1.
Introduction
D
Drug therapy for delirium is an established treatment strategy.8,9 In a randomized, placebo-controlled trial in patients with terminal cancer, antipsychotic drugs for delirium showed no significant treatment effect. However, the subjects in the trial exhibited only mild-to-moderate levels of delirium, 10 and clinical guidelines recommend the use of antipsychotic drugs for the management of severe pain and erratic behavior. 3 Furthermore, patients unable to receive oral drug administration were excluded, despite the observation that individuals with terminal cancer are frequently unable to receive oral medication with disease progression. However, few nonoral antipsychotic drugs are available for administration to this patient population. Intravenous haloperidol, an established antipsychotic drug with low histamine-H1 receptor affinity, is recommended in most guidelines as first-line treatment for all types of delirium, 11 although there are reports that the relief of hyperactive delirium symptoms afforded by haloperidol is insufficient.7,12 Intravenous benzodiazepine is second-line treatment for delirium, although a recent study reported that the addition of benzodiazepine to haloperidol in patients with advanced cancer resulted in a significantly greater reduction in hyperactive delirium compared with haloperidol alone. 13 However, intravenous benzodiazepine is rarely associated with deterioration of delirium and respiratory suppression. 14
Intravenous chlorpromazine, which exerts a strong sedative effect through inhibition of histamine-H1 receptor and α-1 receptor bindings,15,16 has been used empirically to treat delirium in patients with cancer. 17 A previous study reported that ∼13% of off-label medication use was the intravenous administration of chlorpromazine in acute palliative care unit settings in the United States. 18 Although intravenous chlorpromazine was shown to be effective for treating delirium in a randomized controlled trial in patients with HIV, 19 to the best of our knowledge, similar studies have not been performed in patients with terminal cancer.
Given the lack of an optimal treatment strategy for delirium in patients with terminal cancer, it is recommended that drug selection and administration route are considered on an individual basis, according to each patient's disease status. In the present study, we retrospectively assessed the safety and effectiveness of intravenous chlorpromazine for irreversible delirium in patients with terminal cancer.
Methods
Study subjects
A total of 193 patients with terminal cancer and delirium as the main complication were treated by the Palliative Care Department of Kansai Medical University Hospital between June 2015 and September 2017. Figure 1 shows the selection of study subjects. Terminal cancer was defined as cancer with expected survival of not more than two months, based on a 50-day mortality rate of 91% from the onset of terminal delirium, as evaluated by the treating oncologist. 2 The presence or absence of delirium was evaluated using the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV); motoric subtype was determined using the Delirium Motor Subtype Scale and classified as hyperactive (heightened arousal, restlessness, agitation, hallucinations, and inappropriate behavior) or hypoactive (lethargy, reduced motor activity, incoherent speech, and lack of interest)20,21; and delirium was classified as reversible or irreversible by a psycho-oncology specialist. Irreversible delirium was defined as delirium that did not improve following treatment of the cause of delirium. 22 In this study, irreversible delirium was classified as a syndrome, not as a condition requiring continuous deep sedation, but one where the aim of treatment was to relieve symptoms.
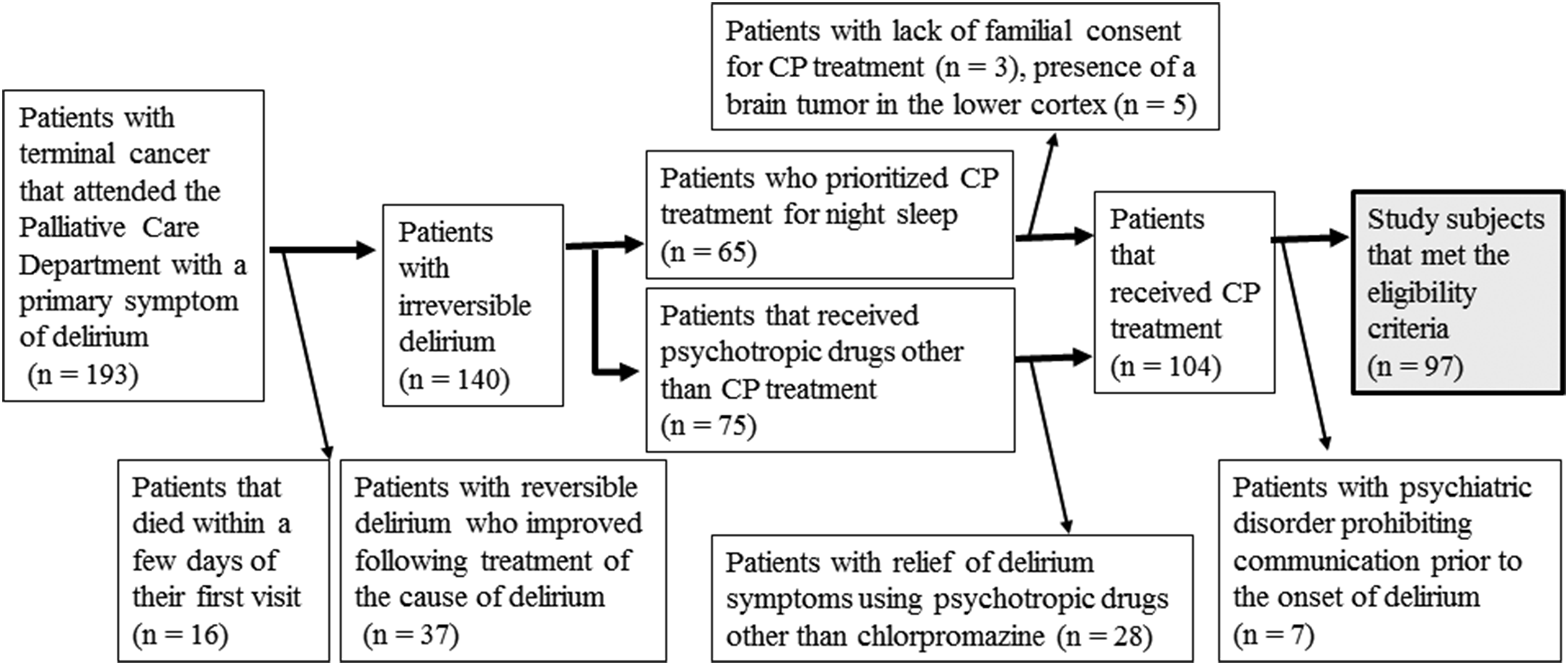
Selection of study subjects.
We have empirically administered intravenous chlorpromazine at bedtime for the relief of delirium symptoms in patients with difficulty receiving orally administered medication, are haloperidol refractory or intolerant, and experience heightened arousal, restlessness, agitation, hallucinations, and inappropriate behavior at night. We have administered chlorpromazine to relieve delirium symptoms, not as a transition from hyperactive to hypoactive. Furthermore, we have even used chlorpromazine to relieve delirium symptoms in patients with hypoactive delirium. In this study, the total haloperidol dose used before chlorpromazine treatment was as high as 4.3 mg/day, which was difficult to increase further. Increased extrapyramidal adverse effects associated with haloperidol above 4.5 mg/day have been reported. 23 We therefore did not add benzodiazepine to haloperidol before chlorpromazine treatment. The initial dose of intravenous chlorpromazine was in the range of 10–25 mg/day with an administration rate of 25 mg/hour and was administered at ∼9 pm and increased as appropriate.
Study analytical parameters
We retrospectively examined the medical records for each study subject. Analytical parameters included demographic factors, primary cancer site, Eastern Cooperative Oncology Group (ECOG) performance status, duration from chlorpromazine treatment until death, motoric subtype of delirium, dose of chlorpromazine, dose of opioids, psychotropic use before chlorpromazine, concomitant psychotropic drugs, Nursing Delirium Screening Scale (NuDESC) score, blood pressure, heart rate, presence or absence of death and extrapyramidal symptoms, and history of falls, convulsion, vasculitis, and subcutaneous callus.
Nursing Delirium Screening Scale
Widely used in oncology inpatient settings, the NuDESC is psychometrically valid and has a sensitivity and specificity of 85.7% and 86.8%, respectively. 24 The NuDESC is an observational five-item scale, measuring the following items with a range of 0–2: disorientation, inappropriate behavior, inappropriate communication, illusions/hallucinations, and psychomotor retardation. Higher scores indicate worse delirium. In a previous study on delirium in patients with terminal cancer, the NuDESC-derived total score for the items, inappropriate behavior, inappropriate communication, and illusions/hallucinations, was the best available primary outcome, with a 1-unit decrease between day zero (predose) and three (three days post-dose) deemed the minimum clinically significant difference. 10
In this study, patients were assessed for NuDESC by nursing staff on the morning of day zero and three. Our hospital routinely used NuDESC, meaning that it was also prospectively measured in this study.
Outcomes
The primary outcome of this study was the identification of factors associated with the effectiveness of intravenous chlorpromazine, based on the comparison between clinically relevant responders and nonresponders. The secondary outcomes of effectiveness included a comparison between predose and post-dose NuDESC scores and rate of chlorpromazine effectiveness on day three, which was determined as the percentage of patients with improvements in NuDESC score ≥50%.
Secondary safety outcomes included death, extrapyramidal symptoms, falls, convulsion, vasculitis, subcutaneous callus, and hemodynamic effects. The presence of extrapyramidal symptoms was evaluated using the Extrapyramidal Symptom Rating Scale (ESRS). 25 Hemodynamic effects were evaluated based on the comparison of blood pressure and heart rate, rate of shock index ≥1 between day zero (predose) and three (three days post-dose), and adverse episodes observed during intravenous drip administration. Adverse episodes were evaluated based on the appearance of subjective symptoms in the patient, systolic blood pressure of 90 mmHg or less, and a decrease of 30 mmHg or more in blood pressure.
Statistical analysis
All data were reported as mean with 95% confidence interval (CI), ranges, average, or frequencies (%), as appropriate. Comparisons of each item of the NuDESC between predose and post-dose time points were performed using an unpaired t test. For discontinued patients, the worst value for each item of the NuDESC was used for the missing time points after discontinuation. An unpaired t test was used for the following dependent variables: age, sex, ECOG performance status, duration from chlorpromazine treatment until death, motoric subtype of delirium, NuDESC score before chlorpromazine treatment, dose of chlorpromazine, psychotropic use before chlorpromazine treatment, concomitant psychotropic drugs, opioid dose, blood pressure, heart rate, and shock index. Median survival was measured using the Kaplan–Meier method. In addition, multivariable logistic regression analysis was performed on the dependent variable of intravenous chlorpromazine effectiveness and eight independent variables: age, sex, prognosis longer than two weeks, hyperactive delirium, NuDESC score before chlorpromazine treatment, psychotropic use before chlorpromazine treatment, concomitant psychotropic drugs, and opioid use.
p-values <0.05 were regarded as statistically significant. Statistical analysis was performed using SPSS software version 18.0J for Macintosh (SPSS, Inc. IBM, Chicago, IL).
Results
The demographic and clinical characteristics of study subjects are shown in Table 1. The median age of the study subjects was 70.0 years (range 35–88 years). Mean performance status score was 3.7 ± 0.5, and mean survival period after chlorpromazine treatment was 18.8 ± 15.8 days. Mean intravenous chlorpromazine dose was 17.9 mg/day (range 10–60 mg/day).
Dose of opioids is expressed as oral dose level of morphine (mg/dL). For conversion: parenteral morphine:oral morphine = 1:2; parenteral oxycodone:oral morphine = 1:2; oral oxycodone:oral morphine = 2:3; fentanyl:morphine = 1:100; oral methadone:oral morphine = 1:8.
CP, chlorpromazine; I.V., intravenous; po, per os; PS, performance status.
NuDESC score was significantly improved on day three after initiation of intravenous chlorpromazine (Fig. 2). NuDESC-derived total score for the items inappropriate behavior, inappropriate communication, and illusions/hallucinations was decreased by more than 1 unit, from 3.2 to 2.0. The chlorpromazine effectiveness rate on day three was 0.48 (95% CI: 0.38–0.58). Based on the criteria of clinically relevant effectiveness, study subjects were classified as 47 responders and 50 nonresponders. The responders demonstrated a significantly higher rate of hyperactive delirium rate (p = 0.005) and a higher rate of longer expected survival (p < 0.001) compared with nonresponders (Table 2). Median survival for all participants who were responders was 21 days, compared with 9 days for nonresponders (Fig. 3). Multivariable logistic regression analysis identified two factors associated with intravenous chlorpromazine effectiveness: hyperactive delirium (odds ratio [OR]: 6.25, CI: 1.14–34.5) and longer expected survival (OR: 1.096, 95% CI: 1.05–1.14) (Table 3).
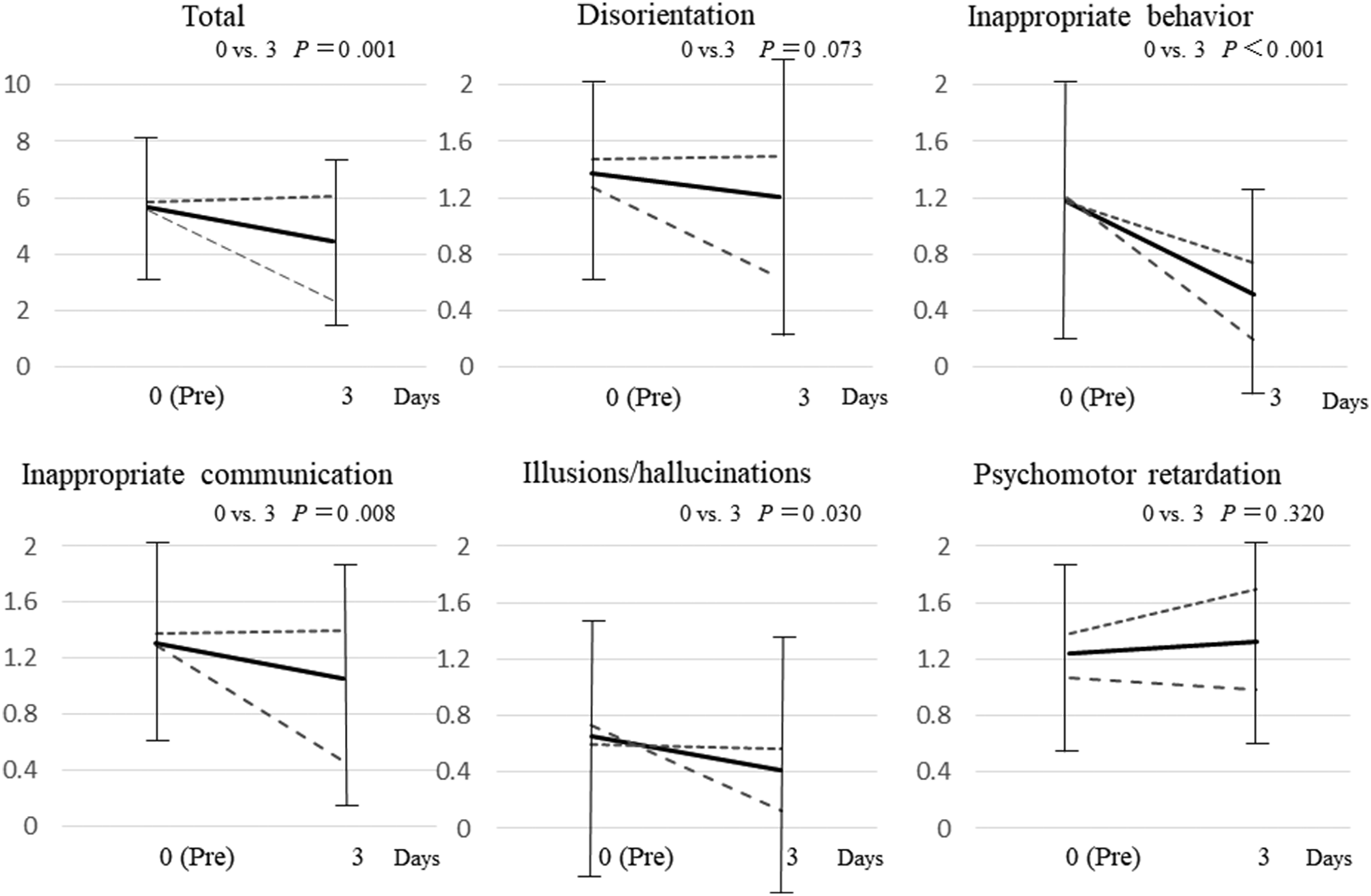
Mean score based on the Nursing Delirium Screening Scale before and after intravenous drip chlorpromazine administration. ART total study subjects (day 0: n = 97, day 3: n = 85); ART responders (day 0: n = 47, day 3: n = 47); ART nonresponders (day 0: n = 51, day 3: n = 39).
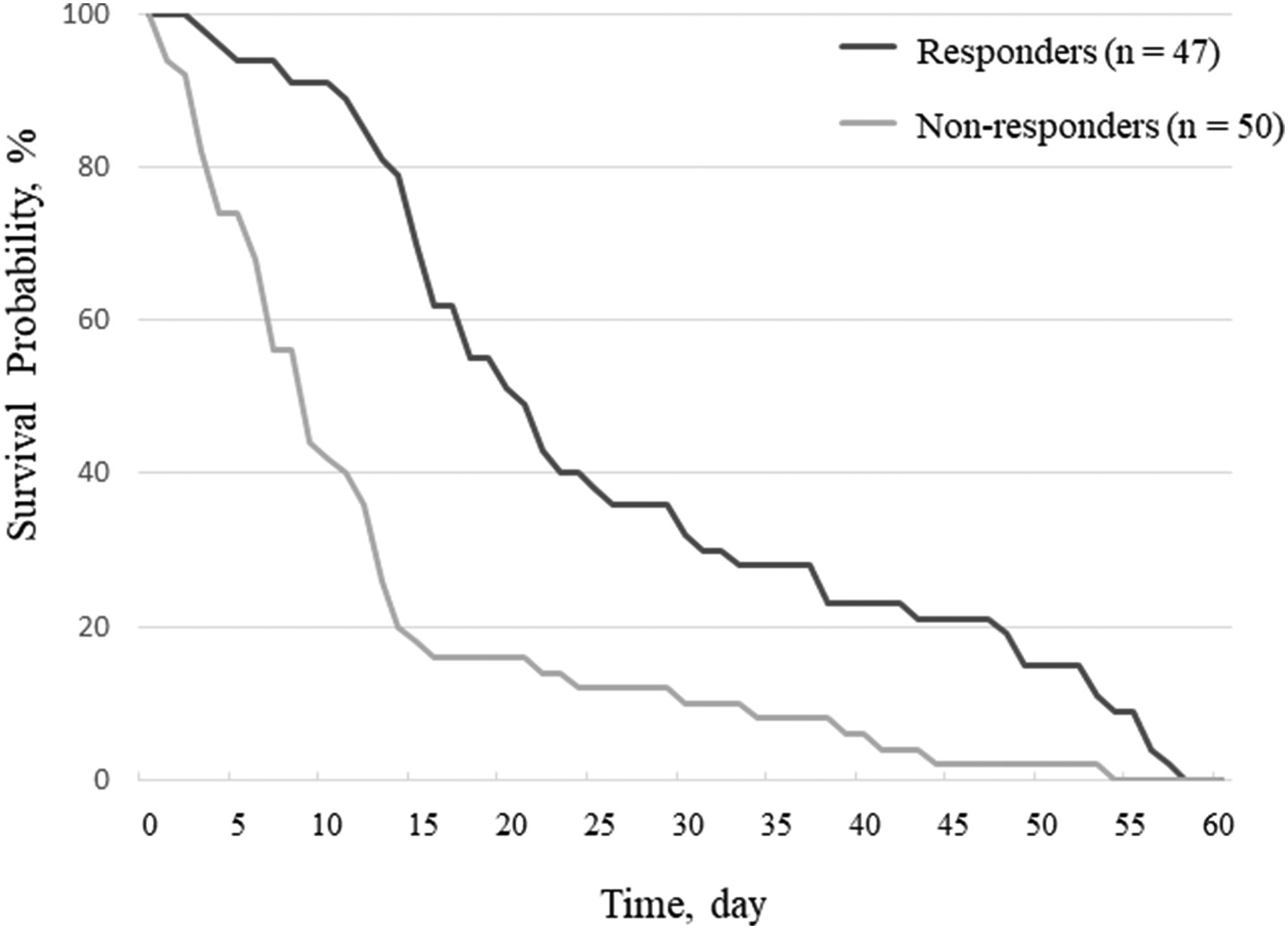
Kaplan–Meier survival of study subjects.
Dose of opioids is expressed as oral dose level of morphine (mg/dL). For conversion: parenteral morphine:oral morphine = 1:2; parenteral oxycodone:oral morphine = 1:2; oral oxycodone:oral morphine = 2:3; fentanyl:morphine = 1:100; oral methadone:oral morphine = 1:8.
CP, chlorpromazine; ECOG, Eastern Cooperative Oncology Group; NuDESC, Nursing Delirium Screening Scale; PS, ECOG performance status; SD, standard deviation.
CI, confidence interval; CP, chlorpromazine; OR, odds ratio; SE, standard error.
By day three after initiation of chlorpromazine administration, 12 patients (12.4%) had discontinued treatment because of death (2 patients), decreased blood pressure during administration (3 patients), addition of intravenous administration of benzodiazepine for delirium progression (5 patients), acute akathisia (1 patient), and medication refusal (1 patient). Eleven patients (11.3%), excluding the patient who had refused medication, were diagnosed as having adverse events associated with intravenous chlorpromazine treatment. Adverse events were all observed in patients within two weeks of starting chlorpromazine treatment. The two patients who discontinued because of death had hyperactive delirium and expected survival less than one week as judged by the treating oncologist, and a rapid decrease in blood pressure from 11 and 14 hours, respectively, after initiating intravenous chlorpromazine. The three patients who discontinued because of decreased blood pressure were identified following routine blood pressure measurement during drip intravenous administration of chlorpromazine and showed a decrease in systolic blood pressure of 30 mmHg or more. None of the three patients showed subjective symptoms, and systolic blood pressure naturally resolved after chlorpromazine discontinuation. One patient who discontinued because of acute akathisia developed this condition following the initial administration of intravenous chlorpromazine (20 mg). The acute akathisia had improved by the following day, but the patient died on day eight following the initiation of chlorpromazine.
No falls, convulsion, vasculitis, or subcutaneous callus were associated with chlorpromazine treatment. Systolic blood pressure was significantly decreased on day three following initiation of intravenous chlorpromazine (Table 2). Among 13 patients (13.4%) with shock index ≥1 before the initiation of intravenous chlorpromazine adverse events included death (2 patients), decreased blood pressure decreasing during administration (3 patients), and acute akathisia (1 patient).
Discussion
The present study is the first report of the assessment of factors affecting the effectiveness of intravenous chlorpromazine, in addition to its safety, for the treatment of delirium in patients with terminal cancer. With a median age of 70 years, patients in this study were relatively elderly, the majority was male, and many had been diagnosed with cancers of the digestive system, neck, and cervix.
Our study reports two important findings. The first is that hyperactive delirium was a factor affecting the effectiveness of intravenous chlorpromazine. Hyperactive delirium is more likely to be associated with inappropriate behavior, optical illusion, and/or hallucination compared with hypoactive delirium. 26 In the present study, the incidence of hyperactive delirium was high, and intravenous chlorpromazine administration was highly effective. Clinical guidelines recommend the use of antipsychotic agents to treat inappropriate behavior associated with delirium. 3 Hyperactive delirium is frequently observed in patients with terminal cancers, with one study reporting that 42% of patients with terminal cancer who died in a university hospital exhibited hyperactive delirium. 27 Hyperactive delirium increases stress among the patient's family members, and its management is clinically important. 28
Intravenously administered chlorpromazine rapidly exerts a sedative effect through inhibition of the histamine-1 receptor and α-1 receptor.15,16 This sedative action appears to be related to the effectiveness of chlorpromazine for the treatment of delirium with inappropriate behavior. Behavioral disturbances associated with delirium appear to worsen at night time. The mean residence time of intravenous chlorpromazine, irrespective of the administered dose, is 8.9 hours, which can cover the average sleeping time. 15
In the present study, optical illusion, hallucination, and inappropriate behavior were improved following chlorpromazine treatment, indicating that intravenous chlorpromazine reduces inappropriate behavior by intermittent sedation as well as improving sensory and attentional disturbance caused by delirium. However, given the retrospective and observational design of our study, full evaluation of the effectiveness of intravenous chlorpromazine was not possible.
The second important finding of our study is that intravenous chlorpromazine exerted a positive effect on delirium in patients with longer expected survival, but negatively affected safety in patients who survived for two weeks or less after treatment initiation. In general, delirium worsens and becomes irreversible and resistant to treatment as the patient approaches death.1,4 It is reported that among terminal cancer patients with expected survival less than one week, 73% of patients exhibited drowsiness, resulting in increased scoring on a psychomotor retardation scale. 29 In the present study, patients who survived for less than two weeks displayed severe psychomotor retardation, and intravenous chlorpromazine further worsened this symptom. Among patients with longer expected survival, intravenous chlorpromazine did not worse psychomotor retardation. Our results suggest that while intravenous chlorpromazine may represent a treatment option for delirium, it may worsen the symptoms of delirium in certain cases because of anticholinergic effects and oversedation. 30
Adverse events were reported in all patients who survived for less than two weeks following intravenous chlorpromazine administration. Intravenous chlorpromazine can decrease blood pressure through inhibition of the α-1 receptor and is therefore contraindicated in patients with circulatory failure. Furthermore, 97% of terminal cancer patients were shown to have hypoalbuminemia three days before death, indicating that intravascular dehydration worsens in the terminal stage of cancer. 31 In the present study, reduced blood pressure was detected in three patients by blood pressure monitoring during intravenous chlorpromazine administration, although no patients became symptomatic. Although in this instance, the reduced blood pressure in all three patients spontaneously resolved, this symptom could potentially induce circulatory shock with continuous chlorpromazine administration. For the two cases of death, it was unclear whether the causality of death was related to circulatory adverse events associated with intravenous chlorpromazine. However, all five patients (three patients with reduced blood pressure and two patients who died) displayed a shock index ≥1 before chlorpromazine administration. Therefore, chlorpromazine administration should be avoided in patients at risk of circulatory failure. The prognosis of cancer patients with decreased consciousness levels and shock index ≥1 has been reported as less than one week. 32 In the present study, the incidence of akathisia associated with chlorpromazine administration was 1.0%, which was lower than that previously reported for haloperidol treatment (11%–13.9% in cancer patients receiving 2 mg oral haloperidol, and 10% in patients without cancer who received 5 mg intramuscular haloperidol). 33
No adverse events associated with chlorpromazine administration were reported in terminal cancer patients who survived for more than two weeks, which may have been attributable to the low dose of chlorpromazine (17.9 mg/day). Studies have reported intravenous chlorpromazine doses of 40 mg/day for the treatment of delirium in patients with advanced cancer and 36–50 mg/day in hospitalized patients with AIDS.17,18 Oral risperidone at a dose of 1.4 mg/day (equivalent to 28 mg intravenous chlorpromazine) or oral olanzapine at a dose of 6.3 mg/day (equivalent to 63 mg intravenous chlorpromazine) have been used for the treatment of delirium in patients with terminal cancer.8,9,34 In contrast, the dose of intravenous chlorpromazine in patients who survived for less than two weeks was 17.4 mg/day. Thus, low-dose intravenous chlorpromazine may represent a safe treatment option for delirium in patients with terminal cancer expected to survive for more than two weeks.
The present study had several limitations. First, this was a retrospective observational study without a control group, meaning that confounding factors for the effectiveness of intravenous chlorpromazine could not be fully excluded. Second, NuDESC was evaluated only twice, once before administration and again on day three, which may have been inadequate for detecting clinically relevant changes in the NuDESC score. Third, a long-term assessment of chlorpromazine administration was not performed, so the safety evaluation remains incomplete. Fourth, we included patients with treatment-resistant delirium for whom the palliative care team requested intravenous chlorpromazine treatment, which may have introduced bias. Fifth, we did not add benzodiazepine to haloperidol before chlorpromazine treatment. This combination therapy has been shown to be beneficial in a recent study reported after our study. 13 If we had implemented this standard regimen, fewer subjects would have been eligible for inclusion. Sixth, since the data analysis was performed by the principal investigator of the study, the analysis was not blinded. Finally, as the study was carried out at a single site, the findings may not be generalizable, and larger, multisite studies are therefore required. Thus, the present study may be considered a pilot study.
Conclusions
Intravenous administration of chlorpromazine is a potentially effective treatment for hyperactive delirium in patients with terminal cancer and expected survival of two weeks or more. The safety of this treatment option was confirmed at a low dose in patients who survived for more than two weeks and with a shock index value <1.