
Abstract
Abstract
Background:
Although mounting evidence supports the use of palliative care (PC) to improve care experiences and quality of life for oncology patients, the frequency of and factors associated with PC use during oncology-related hospitalizations remain unknown.
Materials and Methods:
Using the National Inpatient Sample dataset, hospitalizations during 2012–2014 for a primary diagnosis of cancer with high risk of in-hospital mortality were identified. PC use was identified using the V66.7 ICD-9 code. Factors associated with the cost of hospitalization were identified using multivariable gamma regression.
Results:
During the study period, 124,186 hospitalizations were identified with a primary diagnosis of malignancy (melanoma, breast, colon, gynecologic, prostate, male genitourinary, head/neck, urinary tract, noncolon gastrointestinal, lung, brain, bone/soft tissue, endocrine, or nonlung thoracic). Most patients were treated at a teaching hospital (51–77% by cancer type), and use of PC ranged from 10% for patients with endocrine cancers to 31% for patients with melanoma. Patients utilizing PC had a lower frequency of operative procedures (4–33% vs. 34–79% by cancer type, all p ≤ 0.001), a higher rate of in-hospital death (30–45% vs. 4–10% by cancer type, all p < 0.001), and a lower total hospitalization cost (median: $5076–17,151 vs. $10,918–29,287 by cancer type, p ≤ 0.01 except male genitourinary). In an adjusted analysis, the cost of hospitalization was significantly associated (all p < 0.001) with patient gender, race, age, operative, in-hospital death, extended length of stay, and PC.
Conclusions:
In summary, inpatient PC utilization varied by cancer type. PC was associated with lower utilization of surgical procedures, shorter length of stay, and lower hospitalization cost. Lower hospitalization cost was also seen for patients who were older, female, or African American.
Introduction
P
Inpatient PC significantly improves patients' symptom control, anxiety, and readmission rates 11 and is associated with greater patient satisfaction compared to no PC in observational and randomized studies.12–14 Inpatient PC has been associated with lower costs and resource utilization.12–16 These findings suggest that PC is high-value care, in line with value-based care models being developed (e.g., MACRA). 17 However, prior studies of PC in the inpatient setting have had limited generalizability due to small, single-center study populations and analysis of patients with a variety of cancer diagnoses; large variations in prognosis and treatment by cancer type make it difficult to interpret these results for an individual patient. In addition, it is unknown what proportion of inpatients are receiving PC referrals in the United States and whether PC is being underutilized among patients most likely to benefit from goals of care discussions and palliative interventions. Finally, there is a persistent practice gap as it pertains to PC use. PC has shown benefit across the continuum of cancer care but is underutilized despite Level 1 evidence and multiple national and international guidelines.18–20 Identifying practice patterns, including groups in which PC is underutilized, might help clinicians and policy makers identify barriers to PC and address them to increase access to and quality of PC.
We hypothesized that PC utilization would vary by cancer type and that PC consultation would be associated with fewer operative procedures and a lower cost of care. Using data on hospitalizations across the United States from the National Inpatient Sample (NIS), we sought to characterize the population receiving inpatient PC and factors associated with the receipt of PC.
Materials and Methods
Study population
This retrospective study was completed using data from the NIS from 2012 to 2014. The NIS is the largest all-payer inpatient care database in the United States and includes data on more than seven million hospital stays. 21 The NIS, maintained by the Agency for Healthcare Research and Quality (AHRQ), collects data on demographic characteristics (e.g., age, sex, race, and insurance status) and up to 25 diagnostic and procedural codes, coded using the International Classification of Disease, Ninth Revision (ICD-9) Clinical Modification lexicon. 22 In addition, hospital-level characteristics, including hospital region, location (urban vs. rural), bed size, and teaching status, are recorded for each hospitalization. 22
All patients with a primary diagnosis code indicating solid organ malignancies (gastrointestinal, thoracic, melanoma, breast, male and female genitourinary, head and neck, brain, endocrine, and bone/soft tissue) were identified. Only primary diagnosis was used as per the ICD-9-CM Official Guidelines for Coding and Reporting. 23 Malignancy-related hospitalizations were identified by a primary ICD-9 code between 140 and 239; data were then grouped by cancer type as per the American Medical Informatics Association system. 24 Patients younger than 18 years of age, admitted emergently, having a primary cancer location that was nonspecific or lymph node or a secondary cancer classification or who were transferred between hospitals were excluded. Patients undergoing a major operative procedure were identified using previously defined criteria from the AHRQ. 22 We then identified all inpatient visits with an All-Patient Refined Diagnosis-Related Group (APR-DRG) Risk of Mortality rating of 3 or 4, indicating a high risk of in-hospital mortality. In prior studies, a one unit increase in Risk of Mortality rating was associated with a threefold increase in mortality. 25
Use of PC was determined using the ICD-9 code “V66.7.”26–28 The V66.7 code was originally developed to identify patients with a high risk of mortality who were receiving comfort care and expected to die. 26 As PC has evolved, the V66.7 ICD-9 code began to represent a spectrum of PC services provided to patients. Therefore, mention of receipt of PC in this article indicates that patients received elements of PC sufficient to warrant the use of the PC ICD-9 code. The inability to identify which elements of PC were provided to each patient makes the V66.7 code a blunt instrument for determining PC utilization, but one that still provides basic information about PC utilization.
Primary study outcomes
The primary study outcomes of the current analysis included the frequency of PC among hospitalizations for patients with cancer and a high risk of in-hospital mortality. Secondary outcomes included the frequency of palliative or operative procedures for these patients, the cost of hospitalization, the length of stay in the hospital, and the outcome of the hospitalization (e.g., in-hospital mortality location of discharge); these outcomes were compared among patients who received versus did not receive PC during their hospitalization.
Statistical analysis
Hospitalization costs were adjusted for inflation based on the month and year of the admission using the U.S. Department of Labor Bureau of Labor Statistics CPI Inflation Calculator (https://www.bls.gov/data/inflation_calculator.htm). Comparisons of patient characteristics across malignancy types were performed using the chi-squared test for categorical variables and the rank-sum test for continuous variables. Length of stay was dichotomized at the 75th percentile (12 days); hospitalizations of at least 12 days were considered an extended length of stay. To evaluate factors significantly associated with increased cost of hospitalization, we used multivariable gamma regression, as it provided the best fit for the right-skewed cost data. Characteristics of patients (age, sex, and race) and hospitalizations (treatments received, in-hospital death, and extended length of stay) that were significant in univariate regression were included as covariates in the final multivariable model. All analyses were performed using Stata 14.1/MP for Windows (College Station, TX), and a two-sided p-value of <0.05 was used to define statistical significance.
Results
Patient and hospital characteristics
We identified 124,186 hospitalizations during the study period with a primary diagnosis of malignancy and a high risk of in-hospital mortality. The median (interquartile range [IQR]) patient age was 71 (61–80) years, 46.8% were female, 13.4% were African American, 63.7% were treated at a teaching hospital, and 11.9% died during their hospitalization. Overall, 16.6% of these patients received PC, including 15.4% of patients in 2012 and 18.1% of patients in 2014. Compared to patients who did not receive PC, those who received PC were of similar age [median (IQR) 71 (61–80) vs. 71 (62–80) years] and race (13.8% vs. 13.3% African American) and were as likely to be treated in a teaching hospital (64.2% vs. 63.6%, p = 0.2). Patients who received PC were more likely to be female (48.3% vs. 46.5%, p < 0.001) and die during the hospitalization (36.1% vs. 7.1%, p < 0.001).
Cancer diagnoses included lung (27.0%), noncolon gastrointestinal (22.9%), colon (18.2%), urinary tract (8.5%), gynecologic (6.8%), brain (5.0%), head and neck (3.5%), breast (2.8%), prostate (2.1%), bone/soft tissue (1.2%), endocrine (0.8%), nonlung thoracic (pleural or mediastinal) (0.6%), melanoma (0.4%), and testicular/male genitourinary (0.1%) (Table 1). Frequency of PC varied by malignancy type from 10.0% for patients with urinary tract cancers to 30.7% for patients with melanoma (Table 1). For all cancer types, use of PC was associated with a significantly higher median number of secondary diagnoses (Fig. 1).
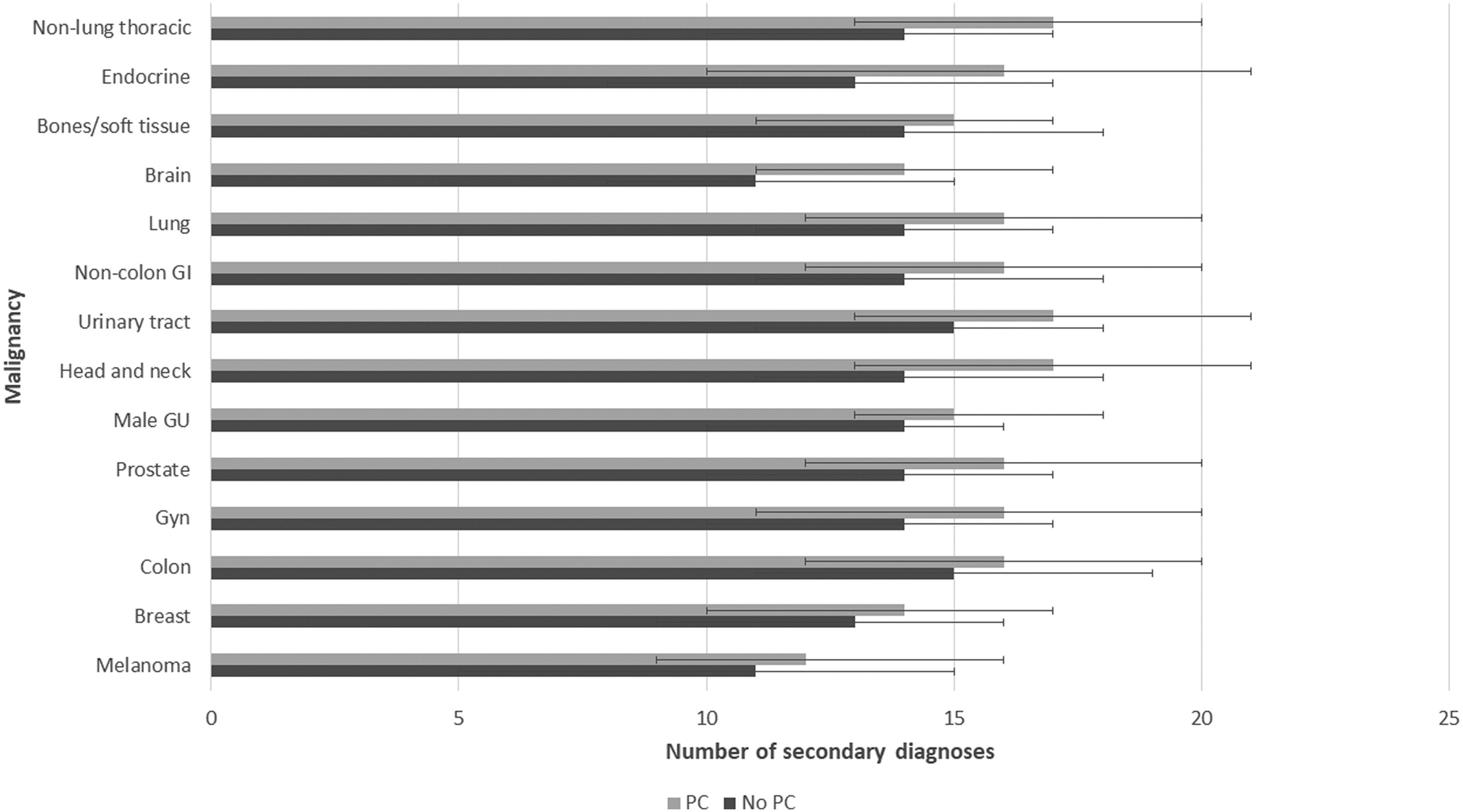
Median (IQR) number of secondary diagnoses by palliative care referral and cancer type.
Receipt of PC was defined as use of the V66.7 ICD-9 code during the inpatient admission.
AA, African American; GI, gastrointestinal; GU, genitourinary; IQR, interquartile range; PC, palliative care.
Frequency of in-hospital interventions by use of PC
During the inpatient admission, 19.9% of patients received at least one palliative procedure (i.e., pleural catheter, percutaneous endoscopic gastrostomy [PEG] tube, or prolonged intubation >96 hours). PC was associated with a significantly higher likelihood of receiving a palliative procedure for half of the cancer types (5–45% vs. 5–41% by cancer type, Table 2). For all cancer types, patients who received inpatient PC were significantly less likely than other patients to undergo an operation during their hospitalization (4–32% vs. 34–79% by cancer type, Table 2). Use of inpatient chemotherapy and radiation varied by cancer type but was overall low (<15%), except for the use of inpatient chemotherapy in patients with male genitourinary cancers (Table 2).
Receipt of PC was defined as use of the V66.7 ICD-9 code during the inpatient admission.
P-values significant at a level of p < 0.05 are bold.
Palliative procedures: pleural catheter, percutaneous endoscopic gastrostomy tube, or intubation >96 hours.
OR, operating room procedure; GU, genitourinary; GI, gastrointestinal.
Frequency of hospitalization outcomes by use of PC
Overall, 49.8% of patients who died during their inpatient admission received PC, versus 13.3% of patients alive at discharge (p < 0.001). For all cancer types, inpatient PC was associated with significantly higher in-hospital mortality, particularly deaths in the first days of the hospitalization. In-hospital mortality rates for patients who received inpatient PC were 30–45%, depending on the malignancy type, versus 4–10% among patients who did not receive inpatient PC. Both overall and when restricted to patients who were alive at discharge, use of inpatient PC was associated with a lower likelihood of being discharged home for all cancer types (Table 3). In the overall study population, receipt of PC was associated with 6.44-times higher odds (95% CI 6.26–6.62, p < 0.001) of in-hospital death compared to no PC.
Receipt of PC was defined as use of the V66.7 ICD-9 code during the inpatient admission.
P-values significant at a level of p < 0.05 are bold.
Among the 109,347 patients who were alive at the time of discharge, 37.0% were discharged home, 30.0% received home healthcare, 32.4% were discharged to a short-term hospital or skilled nursing facility, and 0.6% (N = 1141) left against medical advice or did not have a discharge location listed. Patients who received PC were significantly less likely to be discharged home (8.8% vs. 37.3%, p < 0.001), even among patients who were alive at discharge (13.7% vs. 40.2%, p < 0.001). The overall median (IQR) length of stay in the hospital was 7 (4–12) days. The median length of stay was either shorter or similar for patients receiving PC (Table 4). This pattern remained unchanged after restricting the population to patients who were alive at discharge (Table 4).
Receipt of PC was defined as use of the V66.7 ICD-9 code during the inpatient admission.
P-values significant at a level of p < 0.05 are bold.
GU, genitourinary; GI, gastrointestinal.
Cost of hospitalization by use of PC
The median (IQR) cost of hospital stay was $60,069 ($30,009–$115,116). The median (IQR) cost was $36,857 ($15,879–$79,051) for patients who received PC, versus $65,127 ($33,988–$121,382) for those who did not (p < 0.001). For all cancer types except male genitourinary, the cost of hospitalization was significantly lower for patients who received inpatient PC versus those who did not (Table 5A). After excluding patients who died during the hospitalization, the cost of admission remained significantly lower for all cancers except for male genitourinary, bone/soft tissue, endocrine, and nonlung thoracic (Table 5B).
Receipt of PC was defined as use of the V66.7 ICD-9 code during the inpatient admission.
P-values significant at a level of p < 0.05 are bold.
GU, genitourinary; GI, gastrointestinal.
In a multivariable gamma regression, factors associated with a lower cost of hospitalization included older age [−$220 (95% CI −$229 to −$212) per year], female sex [−$995 (−$1,220 to −$770)], African American race [−$958 (−$1,291 to −$625)], and use of inpatient PC [−$5,122 (−$5,651 to −$4,592), all p < 0.001; Table 6]. Factors associated with a higher cost of hospitalization included an operative procedure [$18,484 ($18,204 to $18,765)], in-hospital death [$2,477 ($2,114 to $2,841)], and extended length of stay [≥12 days vs. <12 days: $27,018 ($26,667 to $27,368) higher cost, all p < 0.001; Table 6]. Statistically significant effect modification on the cost of hospitalization was seen between PC and age (≥65 vs. <65 years old); among patients who received PC, patients who were at least 65 years old had hospitalization costs that were $1,516 ($898 to $2,134) higher than those of patients who were less than 65 years old (p < 0.001, Table 6).
Length of stay was dichotomized at the 75th percentile (12 days).
P-values significant at a level of p < 0.05 are bold.
Discussion
PC has been lauded for its effectiveness in improving patients' quality of life and, with early utilization, quantity of life, but its utilization among inpatients with a high risk of in-hospital mortality was previously unknown. In this national database study of inpatient PC utilization by cancer patients, we found that inpatient PC was associated with a higher median number of secondary diagnoses, lower likelihood of operative procedures, higher likelihood of in-hospital mortality, and a lower likelihood of discharge home versus to another facility for all 14 cancer types studied. For most cancer types, the use of inpatient PC (by V66.7 ICD-9 code) was also associated with a higher rate of palliative procedures (pleural catheters, PEG tubes, and prolonged intubation) and a lower cost for the hospitalization. These findings suggest that patients receiving inpatient PC services may be receiving goal concordant care.
A significant concern is whether the use of the V66.7 code confers a PC consultation or just application of the code. Of note, the V66.7 code is often applied when components of PC, including comfort care, end-of-life care, or hospice care, are discussed in the patient's medical record; its use does not necessarily indicate that a PC specialist was consulted. 28 Only one study addresses whether the V66.7 code correlates with actual PC consultation. 26 At a single U.S. academic center, the V66.7 code had a sensitivity of 49.9% and specificity of 99.1%; in other words, when the V66.7 code is applied, it is highly likely that those patients actually received a PC consult. However, approximately half of the PC consults actually delivered correctly applied the V66.7 code to indicate that such a consultation occurred. 26 Applied to our data, assuming all hospitals had an active PC consultation service, the rates of PC use would be doubled, making this a lower bound for the penetration of PC. Since the V66.7 code identifies comfort care and DNR patients, the association with death would be lessened. In contrast, use of the V66.7 code likely overestimates the use of PC in the inpatient setting, suggesting that PC is more underutilized than our findings would suggest. Underutilization of PC might be due to the persistent association of PC with end-of-life care, rather than as a beneficial component of medical care coordination and goals of care-concordant treatment for patients with severe, complex, and/or chronic conditions. 29
Our finding that PC was associated with a higher likelihood of in-hospital mortality is consistent with prior literature within both U.S. and international cancer patient populations.27,30 In contrast, outpatient PC referral has been associated with a lower risk of in-hospital death. 31 This difference is likely attributable to the timing of the referral, as the majority of outpatient referrals are at least three months before death, while the majority of inpatient PC referrals occur in the last three months of life. 32 This is consistent with findings from surveys of cancer providers, 65% of whom favored initiating end-of-life discussions when patients were symptomatic or had no further treatment options. 33 Our findings suggest that a more holistic approach to referral is needed as the higher number of secondary diagnoses/severity of illness in the PC group suggests that, regardless of mortality risk, these patients have multiple factors that might benefit from PC intervention.
Although many of the associations between PC and specific interventions or outcomes (e.g., discharge home) were consistent across all malignancy types, there were notable exceptions. For example, among patients with lung cancer, PC referral was associated with a significantly lower likelihood of receiving at least one palliative procedure (PC vs. no PC: 24% vs. 28%, p < 0.001). In this case, the association of PC with fewer palliative procedures was likely driven by our definition of palliative procedures, which included insertion of a pleural catheter, insertion of a PEG tube, or intubation for greater than 96 hours; the lower likelihood of palliative procedures was driven by a lower utilization of pleural catheters in patients receiving PC. Additional differences by malignancy included a higher frequency of radiation associated with PC compared to no PC for patients with urinary tract cancer (3% vs. 1%, p < 0.001) or bone/soft tissue cancer (7% vs. 3%, p = 0.008). Similarly, a lower frequency of chemotherapy use was associated with PC for patients with noncolon gastrointestinal cancer (3% vs. 4%, p < 0.001) and lung cancer (4% vs. 7%, p < 0.001). These findings highlight the need to focus on disease specific metrics outside of standard survival and patient reported outcome measures. Any further interventions aimed at improving implementation or sustainability of PC in practice will have to be adaptive and establish relevant metrics to overcome stakeholder barriers.
Our analysis identified older age, female sex, and African American race as variables significantly associated with lower in-hospital costs. In addition, the effect of older age was significantly modified by PC referral; that is, older age was associated with higher costs among the subpopulation who received an inpatient PC consultation. The cost difference is understandable, as previous literature would suggest that older patients are less likely to undergo aggressive therapy for malignancies. It is however interesting to consider the gender and racial differences in cost after adjusting for PC. This could suggest that these groups regardless of PC use are utilizing fewer healthcare resources.
Limitations of this study include the inability to determine causation given the retrospective nature of national database analysis. Our assertion that patients did or did not receive inpatient PC relies on the use of the V66.7 ICD-9 code. This is an imperfect method of ascertaining PC use but has previously been utilized in national database studies.10,28 Furthermore, our study is limited to PC in the inpatient setting. However, it is estimated that the majority of PC occurs in the inpatient setting. 10 Finally, we were unable to determine a patient's stage of cancer from the NIS database. However, by limiting our study population to hospitalizations with a high risk of inpatient mortality by APR-DRG Risk of Mortality, we believe that we eliminated some of the effect of varying cancer stage among cancer patients receiving versus not receiving PC.
In conclusion, we found that inpatient PC in the United States was associated with less aggressive end-of-life care for patients of multiple cancer types and was associated with significant lower hospitalization costs. However, inpatient PC appears to be utilized late in a patient's disease course, as it remains associated with a substantially higher rate of in-hospital mortality. In addition, there is disease-specific variability in utilization of PC. Future research should focus on interventions to increase earlier referrals to PC and strategies to overcome barriers to utilization for patients with symptom management issues or a terminal diagnosis. A disease-based focus may assist with a policy emphasis to target a commensurate increase in PC resources and personnel to ensure timely access to palliative services for those most at need.
Footnotes
Acknowledgments
The first author (J.M.R.) is supported by a grant from the Doris Duke Charitable Foundation. The senior author (F.M.J.) is funded by a grant from the Agency for Healthcare Research and Quality (1K08HS024736-01).
Author Disclosure Statement
No competing financial interests exist.