
Abstract
Abstract
Background:
Although racial/ethnic minorities receive more intense, nonbeneficial healthcare at the end of life, the role of race/ethnicity independent of other social determinants of health is not well understood.
Objectives:
Examine the association between race/ethnicity, other key social determinants of health, and healthcare intensity in the last 30 days of life for those with chronic, life-limiting illness.
Subjects:
We identified 22,068 decedents with chronic illness cared for at a single healthcare system in Washington State who died between 2010 and 2015 and linked electronic health records to death certificate data.
Design:
Binomial regression models were used to test associations of healthcare intensity with race/ethnicity, insurance status, education, and median income by zip code. Path analyses tested direct and indirect effects of race/ethnicity with insurance, education, and median income by zip code used as mediators.
Measurements:
We examined three measures of healthcare intensity: (1) intensive care unit admission, (2) use of mechanical ventilation, and (3) receipt of cardiopulmonary resuscitation.
Results:
Minority race/ethnicity, lower income and educational attainment, and Medicaid and military insurance were associated with higher intensity care. Socioeconomic disadvantage accounted for some of the higher intensity in racial/ethnic minorities, but most of the effects were direct effects of race/ethnicity.
Conclusions:
The effects of minority race/ethnicity on healthcare intensity at the end of life are only partly mediated by other social determinants of health. Future interventions should address the factors driving both direct and indirect effects of race/ethnicity on healthcare intensity.
Introduction
D
In addition, socioeconomic status, such as low levels of income, education, health literacy, and poorer access to health insurance, which are often correlated with race, have also been associated with higher healthcare intensity at the end of life.6–11 Patients with lower levels of educational attainment, for example, are less knowledgeable about advance care planning and less likely to engage in advance care planning or to receive palliative care and hospice services than more educated patients.6,7 Low levels of health literacy are also associated with preferences for aggressive care at the end of life. 11 Furthermore, patients with lower levels of income and less financial stability are less likely to prefer palliative services and more likely to prefer life-prolonging therapies.7,9 Finally, uninsured patients are more likely to be admitted to an ICU and are more likely to die there than are patients with private insurance.6,8,10 As a result of this complex association between race/ethnicity and other markers of socioeconomic status, it is unclear whether prior data identifying higher healthcare intensity at the end of life among minority patients reflect differences by race/ethnicity alone or are confounded by socioeconomic status.
Unpacking this complex relationship is a key step in identifying targets for interventions that can decrease disparities in end-of-life care. Thus, our study objective was to understand the independent influence of key variables of socioeconomic status (education, median income by zip code, insurance) and race/ethnicity on acute care intensity in the last month of life. We hypothesized that racial/ethnic differences would have both direct and indirect effects on intensity of care and that the indirect effects would be mediated by income, insurance, and education.
Methods
Using death certificates and electronic health records, we identified all patients who died in Washington State between January 1, 2010, and December 31, 2015, and were affiliated with a single multihospital healthcare system in the Seattle area. For these patients, we examined healthcare intensity in the last 30 days of life, looking at both direct and indirect associations of race and socioeconomic status on several markers of high-intensity care.
Eligibility requirements
All patients were at least 18 years old at the time of death. We excluded patients whose death certificate indicated a cause of death due to “injury or poisoning emanating from an accident, suicide, homicide, or an undetermined source.” To be eligible, patients had to have at least one of nine chronic conditions listed in the Dartmouth Atlas identified from the electronic health record (EHR) via ICD-9 and International Classification of Diseases, Tenth (ICD-10) codes: cancers with poor prognoses, chronic pulmonary disease, coronary artery disease, heart failure, severe chronic liver disease, chronic renal failure, dementia, diabetes with end-organ damage, and peripheral vascular disease. A determination of affiliation with the healthcare system required that decedents had had at least one nonsurgical inpatient stay at one of the two largest hospitals in the healthcare system in the two years before death or at least two visits to the same outpatient facility in the healthcare system in the last 32 months of life, with at least one visit occurring during the last 24 months of life. These criteria for affiliation were adapted from the Dartmouth Atlas. 12 The university institutional review board assessed this study as not involving human subjects because all patients were deceased, and a waiver of Health Insurance Portability and Accountability Act (HIPAA) consent was approved, as required by Washington State law.
Measures
The outcomes of interest were three markers of high-intensity care at one of the two hospitals during the last 30 days of life: treatment in an ICU, mechanical ventilation, and CPR.
We examined four predictors of interest: race/ethnicity, level of education, estimated income (all obtained from the death certificate), and insurance coverage (obtained from the EHR). Race/ethnicity was a categorical variable, with white race as the reference category; if race was unavailable from the death certificate, we obtained it from the EHR. Educational attainment was modeled as an ordinal variable. Estimated income was an ecological variable, measured as the median income (in thousands of dollars) of the patient's zip code of residence at the time of death and modeled as a linear variable. Insurance status had six categories (private insurance, Medicare, Medicaid, military insurance, other types of insurance, uninsured) with private insurance as the reference category. In addition to the socioeconomic variables, we tested one additional variable as a potential mediator in path analyses: the number of Dartmouth Atlas conditions with which the patient had been diagnosed. This variable, obtained from the EHR, served as a proxy for multimorbidity. Because of a strong floor effect, it was modeled as a continuous variable, censored from below. Finally, we examined patient's gender, age at death, and marital status, obtained from the death certificate, as potential confounding variables.
Statistical analysis
All models were based on probit regression, estimated with weighted mean- and variance-adjusted least squares (WLSMV). Separate regression models tested the association between each predictor (i.e., race/ethnicity, level of education, estimated income, insurance coverage) and outcome of interest (i.e., treatment in an ICU, receipt of mechanical ventilation, and receipt of CPR). Each model included covariate adjustment for any of the three potential confounders whose addition to the unadjusted model changed the coefficient for the predictor by at least 10%. 13
We then built and tested a conceptually derived path model for each outcome. In path models, racial/ethnic minority status was treated as an exogenous predictor, with the remaining predictors of interest (i.e., level of education, median income by zip code, insurance coverage, number of comorbidities) serving as mediators between race/ethnicity and the outcome. Temporal sequence was assumed to flow from race to education to median income by zip code to insurance status to the number of chronic illnesses.14,15 The coding of two variables was simplified for the path analyses. Race was recoded as a dichotomized variable (0 = white non-Hispanic, 1 = Hispanic, minority race, or mixed race). This recoding was justified by analyses showing that patients who were members of each of the racial/ethnic minority groups had similar trends in healthcare intensity, when compared with the white non-Hispanic group. Health insurance was recoded as a dichotomized variable (military or Medicaid insurance compared with other types of insurance or no insurance). This coding scheme was based on prior studies and on analyses from this database showing that military- and Medicaid-insured patients typically received significantly higher intensity end-of-life care than was the case for patients with other types of insurance or no insurance. 6 Patients with no insurance represented a very small group (n = 670) and, as a group, had a relatively high income by zip code. Beginning with saturated models, we removed paths in order of descending p value until all paths had p < 0.05. Diagrams for all path models show the regression coefficients for each in large typeface, with p values shown as superscripts.
Although we examined additional path models that included age and gender as exogenous predictors, to adjust for these potential confounders, the models tested did not change the direction or significance of paths to and from the variables of interest and thus are not presented.
Results
We identified 22,058 decedents who met the eligibility requirements for the study (Table 1). Decedents were predominantly white (82%) and male (57%). Approximately 27% had earned a four-year college degree or higher. The median income for the decedents' zip code was almost $60,000. About one-third had private insurance, another third had Medicare, 23% had Medicaid, and 3% were uninsured. Median age at death was 66 years. Almost half of the decedents were married at the time of death. Over half had been diagnosed with cancer, and about one-fourth with chronic pulmonary disease and/or coronary artery disease.
Except where otherwise noted, the statistics shown is the number and (percentage) of cases.
The statistics shown for this line is the median (interquartile range).
Ecological variable: estimated as the median income of the zip code of the patient's residence at the time of death.
CPR, cardiopulmonary resuscitation.
Regression models
We found significant associations between race/ethnicity, socioeconomic status (SES), and healthcare intensity at the end of life after adjustment for confounders (Table 2). Decedents with lower levels of income were more likely to receive all three types of high-intensity care in the last 30 days of life. Those with lower levels of education and those having Medicaid and military insurance were more likely than their counterparts to receive mechanical ventilation and ICU care. Racial/ethnic minority groups were more likely to be admitted to an ICU and to receive mechanical ventilation than were white non-Hispanics, and black and mixed-race patients were more likely to receive CPR.
For each outcome, a separate probit regression model was run for each predictor (or set of dummy indicators), using weighted least-squares estimation with mean and variance adjustment (WLSMV).
Income was an ecological variable (the median income of the patient's zip code of residence at the time of death), measured in thousands of dollars and modeled as a continuous predictor.
Adjusted for age, gender, and marital status.
Education was modeled as an ordinal predictor.
Adjusted for age.
Unadjusted model (there were no confounders).
Adjusted for age and marital status.
ICU, intensive care unit.
Path models
Path models for all three outcomes fit the observed data well, with p values for χ2 tests of model fit showing nonsignificant misfit (0.76 for CPR, 0.31 for mechanical ventilation, and 0.59 for ICU care). All showed important effects (direct and/or indirect) of racial/ethnic minority status, low estimated income, low education, coverage by Medicaid and military insurance, and high levels of comorbidity with higher intensity of care at the end of life.
Receipt of CPR
The path model for likelihood of received CPR showed a direct effect of racial/ethnic minority status (minorities more likely than white non-Hispanics to receive CPR) and smaller indirect effects through the mediators (Fig. 1; Table 3). The effect of income was primarily direct (lower estimated income associated with greater use of CPR), with effects of education entirely indirect, through the subsequent mediators (lower education associated with greater use of CPR). Medicaid and military insurance holders were more likely to receive CPR than were others, but this effect was indirect—through the association of these types of insurance with higher levels of comorbidity.
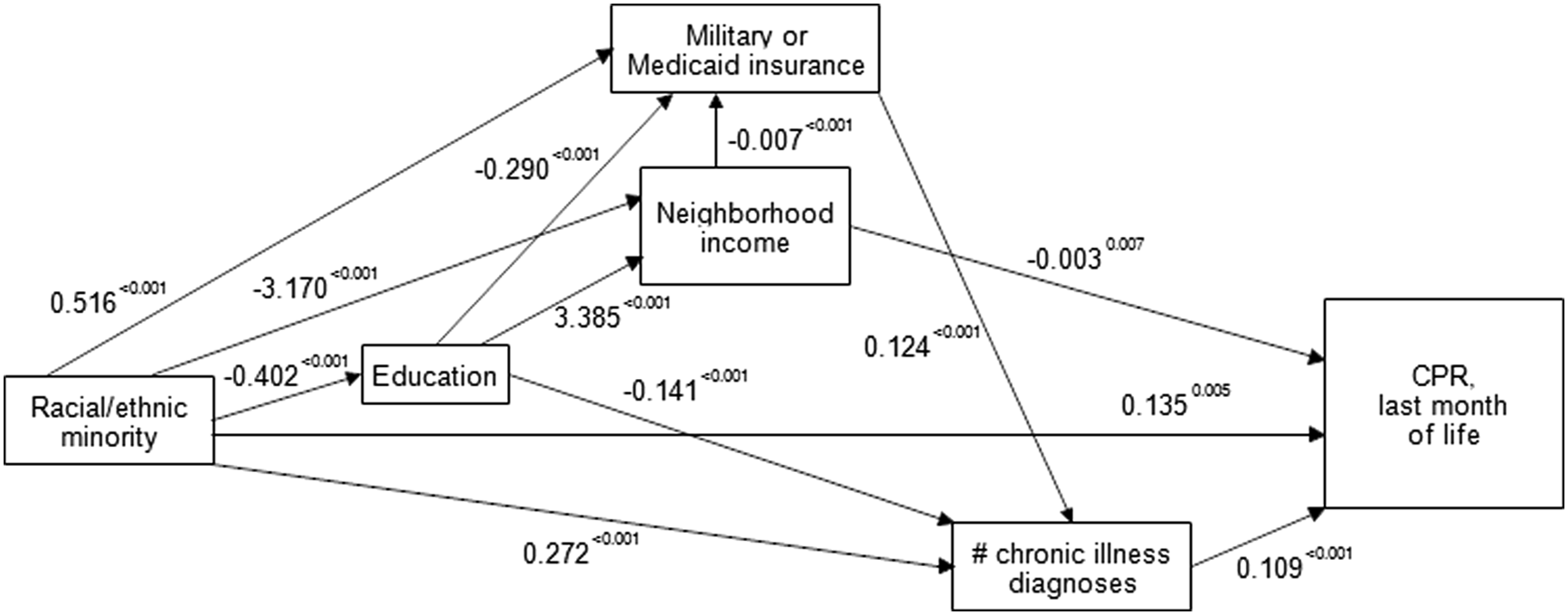
Path model of the influence of race/ethnicity and socioeconomic status on whether any cardiopulmonary resuscitation occurred in the last month of life, with mediation by insurance coverage and the number of chronic comorbidities.
Mechanical ventilation
The path model for mechanical ventilation suggested that the effects of racial/ethnic minority status on receipt of mechanical ventilation (racial/ethnic minorities more likely to receive mechanical ventilation than white non-Hispanics) were about equally attributable to effects mediated by the SES variables and effects that were independent of these mediators (Fig. 2, Table 4). Estimated income had both direct and smaller indirect effects on this outcome (lower income associated with higher use), with education having only indirect effects (lower education associated with higher use). Medicaid and military insurance had both a direct effect on greater likelihood of mechanical ventilation and a smaller indirect effect, through the association of these types of insurance with higher levels of comorbidity.
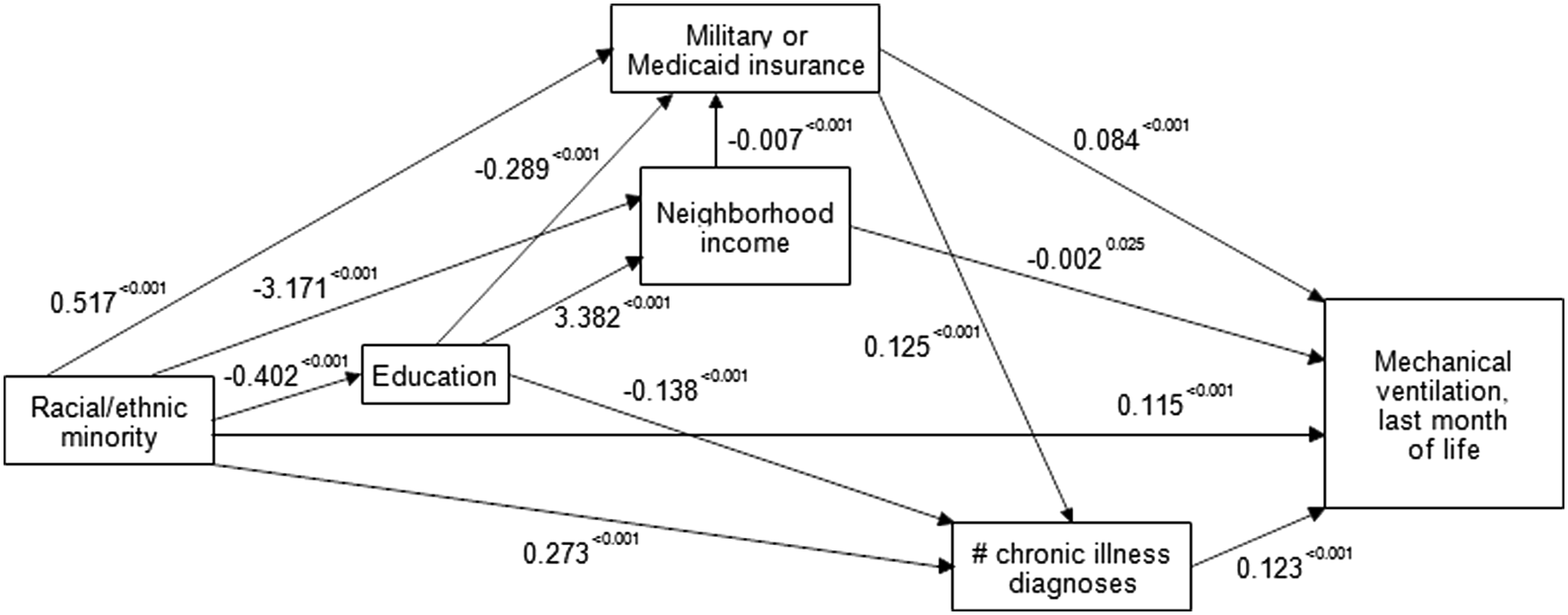
Path model of the influence of race/ethnicity and socioeconomic status on whether any mechanical ventilation occurred in the last month of life, with mediation by insurance coverage and the number of chronic comorbidities.
ICU care
Finally, the path model for ICU care at the end of life showed racial/ethnic minorities more likely to receive ICU care than white non-Hispanics, both because of a direct effect of race/ethnicity and smaller indirect effects through the mediators (Fig. 3, Table 5). The effects of estimated income and education on ICU admission were all indirect. Insurance status had both a direct effect and a smaller indirect effect through its association with higher levels of comorbidity.

Path model of the influence of race/ethnicity and socioeconomic status on ICU care was provided in the last month of life, with mediation by insurance coverage and the number of chronic comorbidities. This model, again, showed nonsignificant misfit to the observed data (p = 0.5893 for the χ2 test of fit). The regression coefficients are shown in larger typeface on each path (with p values shown as superscripts). The model was very similar to the model for mechanical ventilation. Patients from racial/ethnic minorities, those with lower education, those living in neighborhoods with lower median income, those covered by military or Medicaid insurance, and those with more chronic diseases were significantly more likely than their counterparts to receive ICU care in the last month of life.
Discussion
In this study of decedents from a large urban and rural catchment area, we found that racial/ethnic minorities were more likely to receive higher intensity care at the end of life, and that the association between race/ethnicity and aggressiveness of end-of-life care was only partly mediated by other modifiable variables of socioeconomic status. The important associations between race/ethnicity and socioeconomic status are often used to explain the existence of racial/ethnic differences in healthcare intensity at the end of life. We demonstrate, however, that disproportionate socioeconomic disadvantage accounts for some, but not all, of the differences in healthcare intensity at the end of life, and that race/ethnicity itself plays a large and significant role.
Several possible explanations may underlie the higher intensity of care experienced by racial/ethnic minorities in our study. First, prior studies have found that black patients, in particular, receive less intensive medical interventions (e.g., primary care, elective procedures) compared with whites over their life span, and this lack of access to beneficial interventions may result in lower levels of trust in the medical system.16–18 This lack of trust and increased concern about receiving appropriate medical care may lead patients to view advance directives as a means of further excluding them from healthcare rather than as a way to increase their control over future medical care and decision making.17,19 Patients from racial/ethnic minorities may thus be less likely to decide to forgo life-sustaining measures and instead may opt for more aggressive therapies. 20
Second, prior studies have documented differences in the quality of communication between providers and patients from racial/ethnic minorities.21,22 Compared with white patients, patients from racial/ethnic minority groups are more likely to report poorer overall communication. 23 In the outpatient setting, black patients experience more verbal dominance and less patient centeredness than white patients 24 and, in the inpatient setting, patients from racial/ethnic minorities experience more discord with their providers. 6 These documented disparities in communication quality may explain differences in healthcare intensity. 20 For example, inadequate communication about treatment preferences and their implementation into care may explain why black patients receive more life-prolonging care than white patients even when DNR orders are present. 25 Although prior research suggests that patients from racial/ethnic minorities are more likely to prefer high-intensity care and less likely to participate in advance care planning, a patient's individual preferences may not be adequately ascertained or implemented if assumptions and preconceptions are made about the care a patient may prefer without communicating explicitly and thoroughly about his/her preferences.17,18,20
Interventions to improve patient/provider communication for patients from racial/ethnic minority groups may help to better ascertain informed patient preferences for end-of-life care. For example, high-quality communication around prognosis and end-of-life preferences has been found to result in less intense care and lower costs at the end of life across groups defined by race/ethnicity or SES. 26 In addition, integration of palliative care may provide an opportunity to improve communication, increase quality of life, decrease aggressive care, and lower costs and may attenuate some of the racial/ethnic differences in healthcare intensity at the end of life. 1
Our study has several limitations. First, this study was limited to a single healthcare system in Washington State and may not generalize to other regions or healthcare systems, although our results are consistent with prior studies. Second, we focused on patients who had one or more of nine chronic, life-limiting conditions, and these findings may not generalize to other chronic conditions or to acute critical illness without an underlying chronic illness. Third, our study examined decedents and may not accurately reflect care delivered to all patients earlier in their course of chronic illness. 27 However, our focus was on intensity of care in the last month of life for conditions that are generally present for much more than a few months, making this less of a concern for our study. Finally, we used death certificate data and medical records, which may result in some misclassification for race, ethnicity, or socioeconomic status.
In conclusion, we show that racial and socioeconomic differences continue to exist in healthcare intensity at the end of life. Our study suggests that racial/ethnic differences in end-of-life care are due, in part, to the association of race with socioeconomic status, but patient race/ethnicity plays a persistent role in accounting for these differences. Racial/ethnic differences in trust and preferences, in addition to disparities in patient/provider communication, may explain why differences in end-of-life care persist. These findings suggest that interventions designed to eliminate disparities in end-of-life care must address the reasons for disparities in care by race/ethnicity and by socioeconomic status.
Footnotes
Acknowledgment
The research reported in this article was supported by the Cambia Health Foundation and the National Institutes of Health under award number T32HL12595.
Author Disclosure Statement
No competing financial interests exist.