
Abstract
Abstract
Introduction:
Palliative care uses a team approach, including physicians, nurses, social workers, chaplains, and pharmacists. The pharmacist's role within palliative care teams is increasing and initial favorable outcomes have been reported.
Methods:
This retrospective study evaluated adult hospitalized patients seen by a part-time palliative care specialist pharmacist as part of the palliative care consultation team at an academic health system during a 15-month period between September 1, 2015, and March 30, 2017. Our study's objective is to identify patterns of an inpatient palliative care pharmacist's interventions and outcomes and evaluate the impact of pharmacist involvement on patient hospital length of stay (LOS), length from admission to palliative care consult (LTC), and time from consult to discharge or death (CTD).
Results:
The palliative care pharmacist was on service 35% of the time and saw 26.4% of the patient seen by the palliative care team (n = 341 out of 1293). Each patient received an average of 3.5 interventions with an average of 4.1 documented outcomes. The most common interventions were optimizing palliative medication regimen and providing education; most common outcomes were implementation of a change in palliative medication regimen and education of healthcare professionals. Overall, patients seen by the palliative care pharmacist were younger (p < 0.05), more likely to be female (p < 0.05), and more likely to have a primary palliative consultation reason listed as “pain” (p < 0.005). LOS, LTC, and CTD were significantly longer for patients seen by palliative care pharmacist.
Conclusion:
Pharmacist interventions and outcomes were predominantly related to optimizing symptoms by changes in medication regimen and education of healthcare professionals. A subanalysis of patients with known date of first pharmacist visit found significantly improved LOS, LTC, and CTD for patients with early access to palliative pharmacy (in addition to the other members of the palliative team) compared to those without early access.
Introduction
Quality palliative care is a team effort and requires collaboration among many disciplines, 1 most notably physicians, pharmacists, nurse practitioners, social workers, and chaplains. 2 This team approach in palliative care has been coined “transdisciplinary” (in which members create a shared team mission, benefit from role overlap, and have integrated responsibilities, training and leadership).1,3 The overlap in roles is vital in the comprehensive approach to palliative care as all disciplines work together to optimize care for the patient and families. 1
The important role of a palliative care pharmacist has been extensively described in ambulatory care, inpatient, community, long-term facilities, and home-based care.4–25 American Society of Health-System Pharmacists (ASHP) guidelines on the pharmacist's role in palliative and hospice care were updated in 2016 26 to reflect the expansion of pharmacist within the specialties of palliative care and hospice. The ASHP guidelines delineated and described pharmacists' roles and highlighted essential clinical, administrative, practice development, advocacy, and advancement. Walker et al. 27 summarized the roles and responsibilities of palliative care pharmacists into five categories: provision of pharmaceuticals, optimizing medication regimen, educating and providing drug information, monitoring and ensuring patient safety, and participating in administrative and formulary management. In the transdisciplinary palliative care setting, pharmacists' assessment includes both physical and psychosocial suffering of the patient. 28 The advanced role of palliative care pharmacists as independent prescribers with prescribing authorities under collaborative protocol is established and set the direction for the progression of the profession of pharmacy within the specialty of palliative care.4,29,30 Pharmacists have also been in the effort to combat and educate on opioid abuse and controlled substances diversion. 31
There are initial positive outcome studies evaluating the impact of a pharmacist on a palliative care team or consulting pharmacists for hospice.29,30,32–37 A high percentage of palliative care pharmacists' recommendations for clinical interventions is accepted within a team.33,35,37 Inclusion of a pharmacist on a palliative care team was well received by patients and healthcare providers and contributed to higher efficiency of the palliative care clinic. 36 Recommendations by consulting pharmacists to hospices predominantly achieved therapeutic goals.33,37 A study with a palliative care pharmacist seeing patients in a multidisciplinary clinic with physicians and nurses was able to show improved symptoms after initial visit and these improved symptoms were maintained in the subsequent visit. 30 Another study showed that pharmacist-led outpatient palliative care practice identified medication problems for management of pain and other symptoms and resulted in changes such as starting a new medication and/or changing the dose of the medications with trends of pain improvement. 38
To our knowledge, no study has evaluated an inpatient pharmacist's interventions and outcomes as part of an inpatient, transdisciplinary palliative care consultation team, while assessing impact of pharmacist involvement on patient variables. Our primary aim is to describe an inpatient palliative care pharmacist's interventions and outcomes; secondarily, we evaluate the impact on length of stay (LOS), length from admission to palliative care consult (LTC), and time from consult to discharge and death.
Methods
This was a retrospective analysis evaluating adult hospitalized patients (new and follow-up consults) seen by a specialist palliative care pharmacist as part of the palliative care consult team at University of California, San Diego academic health system, during a 15-month period between September 1, 2015, and March 30, 2017. This specific time frame was selected because the pharmacist interventions and outcomes flow sheet (Supplementary Data; Supplementary Data are available online at www.liebertpub.com/jpm) was implemented in the electronic health record (EHR) in September 2015. A 15-month period was thought to be sufficient to capture an initial description of the work of the palliative care pharmacist, while allowing for maturation of the process of documenting interventions and outcomes.
Data collection
All data were collected from a single EHR, EPIC™ flow sheet (Supplementary Data), and exported to an Excel™ spreadsheet. The flow sheet is connected to the palliative team's participation in the Palliative Care Quality Network and is completed on all patients by members of each consultation team. Primary components of the flow sheet are completed by the nurse practitioner. Pharmacist interventions and outcomes were self-reported from standardized drop-down menus (Supplementary Data) by one specialist palliative care pharmacist in the course of providing clinical care for patients in concert with the palliative consultation team. Data collection included patient demographics, admission and discharge date, age, sex, and primary diagnosis leading to palliative consultation. The drop-down menu options were created by the palliative care pharmacist with input from the palliative care leadership and further revisions by the EPIC team were made to customize word count for the flow sheet. These data were later extracted from the EPIC™ flow sheet for analysis. Additional data collection included the following: length of hospital stay (LOS), reason for consult to palliative care team, date of palliative care consult, LTC, and time from consult to discharge or death (CTD). Data were collected on patient dispositions, including discharged alive, hospice, facility w/out hospice, or home w/o hospice, and deceased. The primary endpoint was a descriptive report of most common interventions and outcomes for palliative care pharmacists. Secondary endpoints included correlation between palliative care pharmacist interventions and patient-specific factors: LOS, LTC, and CTD.
Previous internal data (unpublished) were used for comparing LTC and LOS data. To better elucidate timing and quantity of palliative care pharmacist interventions, chart review was completed by a single author (A.M.S.) on a subpopulation of patients seen between September 2015 and February 2016. These patients were selected because encounter codes were available to allow evaluation of the specific encounter referenced. To facilitate more detailed analysis, additional data were collected from the subanalysis population by retrospective chart review completed by a single author (A.M.S.) to obtain primary diagnosis leading to palliative involvement, date of first and last palliative care pharmacist intervention(s), as well as total number of palliative care pharmacist visits.
Pharmacist's role
The pharmacist is an associate faculty with her time split between campus activities and clinical responsibilities dedicated to the palliative care team two full days a week. The pharmacist's postdoctorate training included a postgraduate year 1 acute care pharmacy residency and fellowship training through San Diego Hospice and Institute for Palliative Medicine, ASHP: Pain Management and Palliative Care Traineeship at University of Maryland. The pharmacist had been working with the palliative care team for 11 years. She started in the ambulatory clinic with prescribing authority under DEA license and collaborative practice protocol,4,38 and then transitioned per team request as an inpatient pharmacist. On the inpatient side, the pharmacist guides the transdisciplinary team, including trainees, on medication selection; dosing including dose adjustments for kidney, liver dysfunction, and in anticipation of, or actual, corrected QT interval (QTc) prolongation; titration of medication based on medication pharmacokinetics; and monitoring clinical effect based on medication pharmacodynamics. The pharmacist provides patient and family education regarding use of medications, importance of adherence, and when and to what extent symptoms may be relieved. The pharmacist provides education to several pharmacy, medical, and nursing trainees, as well as other healthcare professional on palliative care approach and medication use both at the bedside and in formal education settings. The palliative care consultation team providers, including the pharmacist, usually recommend changes to medication orders, labs, and diagnostic testing, but as per primary team request or permission, the pharmacist and other providers may also enter these orders in the EHR. Perhaps most importantly, the pharmacist serves as a liaison between the palliative care team and the department of pharmacy at the medical center in ensuring appropriate, safe, medication effective use and patient care. Before discharge of patients from the hospital, the palliative care pharmacist ensures adequate home medication supply until next clinic appointment with their primary managing provider. In addition, if the patient was being followed by the palliative care clinic, the palliative care pharmacist ensures communication with the outpatient palliative care team, including the outpatient specialist palliative care pharmacist. The pharmacist's role is in line with the Center to Advance Palliative Care (CAPC) “Sample Job Description for Inpatient Palliative Care Clinical Pharmacist.” 39
Descriptive statistics and single-factor analysis of variance were calculated using a p < 0.05 as an indicator of significance.
Results
A single specialist palliative care pharmacist at one site within a large academic health system with 35% effort devoted to clinical practice saw 341 patients with the palliative team in a 15-month period. This represents 26.4% (n = 341 out of 1293) of the total patients seen by the palliative team at this site during this period of time. Each patient received an average of 3.5 interventions with an average of 4.1 documented outcomes. The most common palliative care pharmacist interventions were optimizing palliative medication regimen and providing education (Fig. 1). The most common outcomes were implementation of a change in palliative medication regimen and education of health professionals (Fig. 2).

Documented interventions of a palliative pharmacist on an inpatient palliative consultation team. (Potentially more than one per patient.) PDMP, prescription drug monitoring program.
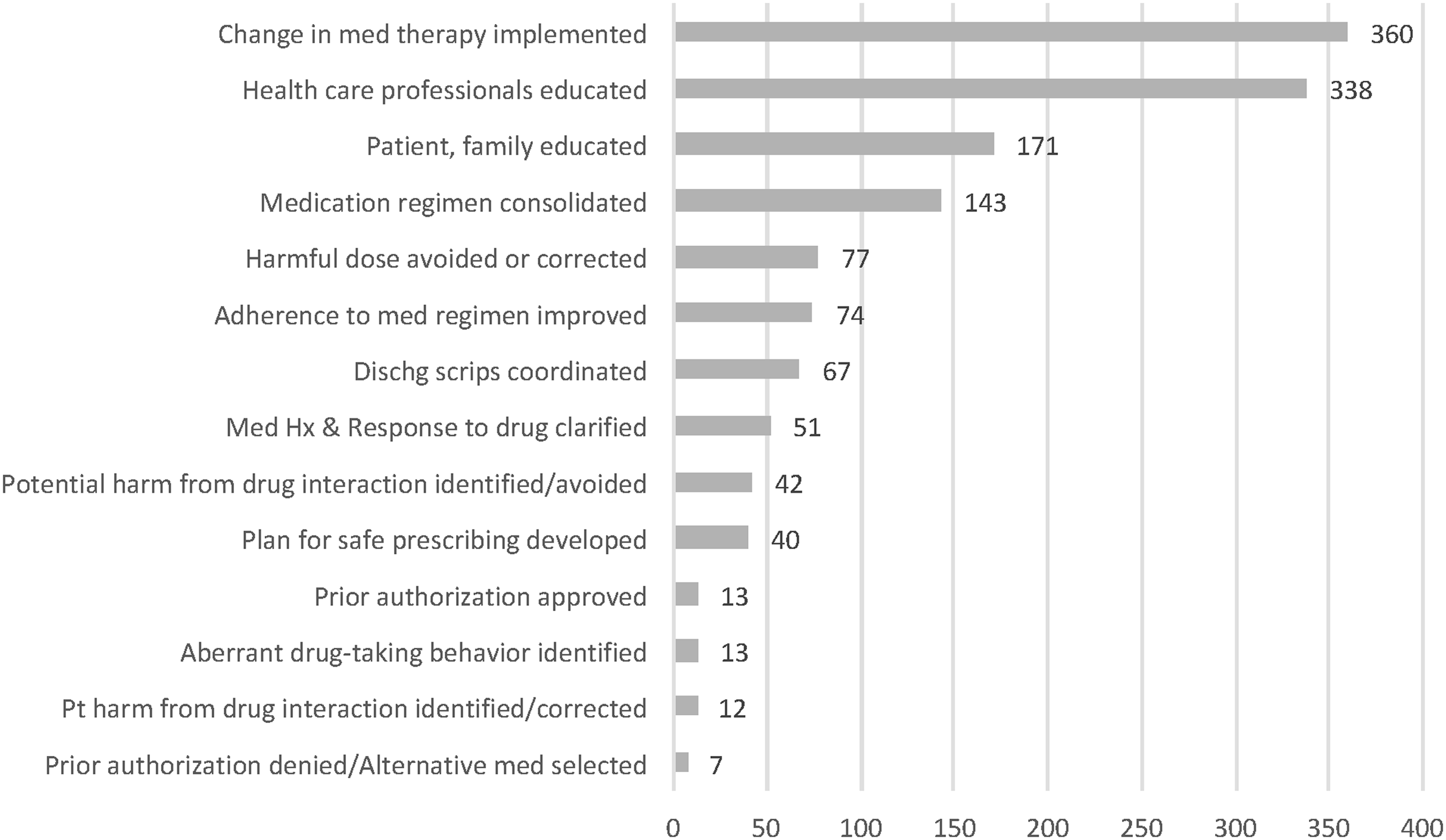
Documented outcomes of a palliative pharmacist on an inpatient palliative consultation team. (Potentially more than one per patient.) dischg, discharge; Hx, history; med, medication; Pt, patient.
Patients seen by the palliative care pharmacist (Table 1) were consulted for pain management 80.9% (n = 276) of the time. Their mean age was 53.9 with 132 males (38.7%) and 209 females (61.3%). These patients had a mean LOS of 14 days with a mean LTC time of 4.8 days and a mean CTD time of 9.5 days (compared to 8.2 days for all patients seen by palliative care, p < 0.005). Two hundred ninety-seven (87.1%) patients were alive at discharge. Of these patients, 219 (64.2%) were discharged home, 42 (12.3%) were discharged to a facility, and 31 (9.1%) were discharged to hospice care either at home or at a facility. Forty-four (12.9%) patients died during their hospitalization. Overall, patients seen by the palliative care pharmacist were younger (p < 0.05), more likely to be female (p < 0.05), and more likely to have a primary palliative care team consultation reason listed as “pain” (p < 0.005). There was no difference in disposition status observed between the two groups.
Demographic and Admission Characteristics of Inpatients at an Academic Medical Center Seen by Specialist Palliative Care Pharmacist Compared to Those Seen by Specialist Palliative Care Team During a 15-Month Period
Significant.
LOS, length of stay.
Given the part-time nature of the specialist palliative care pharmacist coverage, patients who were seen by the pharmacist had a significantly longer time on the palliative team as represented by CTD (median of 4.3 days for all patients seen by palliative compared to a median CTD of 7.2 days for those seen by pharmacist, p < 0.005). There was no significant difference between the two groups in overall LOS. LTC time was also significantly longer for the subset of this population seen by the pharmacist (all patient median LTC 4.1 days, mean 6.7; pharmacist subset median LTC 6.3, mean 8.9; p < 0.005).
Prior internal analysis for our teams has found that there is a beneficial impact on overall LOS, intensive care unit stay, and cost if the palliative care teams are consulted on or before day 3 of hospitalization. This was true for 752 of the patients (58.2% of all patients seen by the palliative care team) included in this study, 243 of whom were seen by the palliative care pharmacist. In this study, the median LOS for all patients seen by palliative care teams on or before day 3 of their hospital stay was 5.7 days (mean 8.3 days), and a reduction of 3.3 days over the median in all patients seen by palliative teams during the study period. In the population seen by pharmacist, the median LOS was eight days (mean of 10.5), which was significantly longer (p < 0.005).
A subanalysis through manual chart review was completed on a subset of patients seen by the palliative care pharmacist between September 2015 and February 2016 (n = 110) where encounter-level identification was available. This subset of patients demonstrated a significant difference in total hospital LOS and LTC time compared to the overall population (see Table 2). For these patients, the majority (87.4%) had a cancer diagnosis related to the palliative consult (see Table 3). First, pharmacist visit to discharge time was shorter than that for the overall palliative care team CTD time (mean 3.84 days, median 4.57 days). Mean and median number of palliative care pharmacist visits were 1.72 and 1, respectively.
Subanalysis of Visit Details for Patients with a Visit by Palliative Care Pharmacist Documented Between September 2015 and February 2016 (n = 110)
PC, palliative care.
Subanalysis of Visit Details for Patients with a Visit by Palliative Care Pharmacist Documented Between September 2015 and February 2016 (n = 110)
In this same subpopulation, if the first palliative care pharmacist visit happened before day 3, total hospital LOS (mean 10 days, p < 0.005), LTC (mean 3.8 days, p < 0.05), and CTD (mean 6.1 days, p < 0.005) times were significantly reduced compared to patients seen by palliative care pharmacist on or after day 3. There was no significant difference in the number of palliative care pharmacist visits (see Table 4). These times were longer than those of the patients seen by the overall palliative team before day 3, however (mean 8, 1.2, and 8.2 days, respectively).
Subanalysis of Patients with a Visit by Palliative Care Pharmacist Documented Between September 2015 and February 2016 by Timing of Pharmacist Visit (n = 110)
HD, hospital day.
Discussion
In this retrospective analysis of adult hospitalized patients seen by a palliative care specialist pharmacist as part of a consult-based palliative care team, an average of 3.5 interventions and 4.1 documented outcomes was observed per patient. It is not surprising that interventions and outcomes by the pharmacist are predominantly related to symptom management and medication changes as pharmacists are the lead experts on pharmacodynamic and pharmacokinetic properties of medications on a palliative care team. This supports a prior study evaluating palliative care pharmacists in the ambulatory care setting 38 that similarly identified pharmacist interventions as primarily related to medication changes that were associated with an outcome of improvement in patients' pain. 38 In addition, our results showed that a main role of the palliative care pharmacist within a transdisciplinary team in an academic medical center was to educate other members of the team as well as other healthcare providers on medication pharmacology. The ASHP guidelines on the Pharmacist's Role in Palliative and Hospice Care 26 lists “provide drug information and lead the team efforts on evidence-based therapy to optimize symptom management” as an essential role of palliative and hospice care pharmacists. Walker et al. 27 also highlight the importance of palliative care pharmacists educating other healthcare providers on “palliative care pharmacotherapeutic principles.”
This analysis, to our knowledge, represents the first published literature on the most common interventions and outcomes made by a palliative care pharmacist in the routine care of patients in the inpatient setting. Prior studies have revealed a positive impact made by pharmacists in the outpatient palliative or hospice palliative setting.30,33–38 While interventions made by the palliative care pharmacist did not lead to a decrease in LOS, this may be due to the part-time coverage provided by palliative care specialist pharmacist and the significantly longer LTC of the patient population seen. We were not surprised by this fact as our prior internal analysis revealed that impact on LOS was seen in patients on or before day 3 of hospitalization. In addition, the pharmacist may be recruited by the palliative care team to be involved with complex patients, in which discharge barriers related to pain and other symptoms not being well controlled and gaps in medication transition to home may be a factor. This hypothesis is supported by our subanalysis of patients with known date of first palliative care pharmacist visit, which found significantly improved LOS, LTC, and CTD for patients with early access to palliative pharmacy (in addition to the other members of the palliative team). Further studies evaluating reason for increased LOS and complexity of patients seen by palliative care pharmacists are needed to substantiate this hypothesis. Our subanalysis also revealed that if the palliative care pharmacist visit happened before day 3, LOS, LTC, and CTD were significantly reduced compared to patients seen on or after day 3 by the palliative care pharmacist. This demonstrates the importance of having the palliative care pharmacist involved early on after the consult is placed. These times were longer compared to the patients seen by the overall palliative team, which may have been influenced by the aforementioned differences in patient population and possible complexity of patients seen by the palliative care pharmacist.
A limitation of this study includes the part-time coverage provided by the palliative care specialist pharmacist. Less than half of all patients seen by the palliative care team were seen with the palliative care pharmacist. The patients seen were younger, more likely to be female, had a primary reason for consult as “pain,” and had a longer LTC. These differences may have led to results observed in this analysis. Ideally, a prospective study randomizing patients to either a pharmacist-involved palliative care team or to one without should be conducted. Furthermore, comparison of these data to those from a site with a full-time specialist palliative care pharmacist may yield insight into any additional impact on patient outcomes when a palliative care pharmacist is continuously available to the patient and team. Both interventions and outcomes were reported by a single specialist palliative care pharmacist in the course of providing care to patients. As such, the data may be affected by reporter bias. We plan further analysis of patient-level outcomes such as subjective symptom control in relation to specialist palliative care pharmacist interventions as, although these data are tracked, it was unavailable to us for analysis for this study.
Conclusion
This study provides the types of palliative care pharmacist interventions as well as the documented outcomes a palliative care pharmacist can provide on an inpatient palliative care consult service as part of transdisciplinary team. While outcomes like decreased LOS have not been demonstrated with this study, this was a secondary analysis and it is encouraging that multiple interventions and documented outcomes are made by the pharmacist on each patient seen. We speculate that future studies will reveal that palliative care pharmacist involvement as part of the transdisciplinary inpatient palliative care team will lead to positive outcomes, similar to results seen in the outpatient setting. In addition, this study demonstrates one way pharmacists can document and integrate their interventions and patient outcomes into an electronic medical record.
Footnotes
Acknowledgments
The authors thank Debra Paulson for her assistance with data support. The Palliative Care Quality Network registry provided data for the total population of patients seen by the University of California, San Diego Health (UCSDH) specialty palliative care teams, with assistance from the UCSDH Performance Improvement and Patient Safety Department in uploading team data.
Author Disclosure Statement
No relevant competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.