
Abstract

Dear Editor:
Motivational interviewing (MI), a person-centered counseling approach in which the clinician helps individuals explore and resolve ambivalence about behavior change, 1 has been successfully employed to improve outcomes for behaviors including substance use, diet, and exercise. 2 Theories of behavior change have been shown to explain engagement in advance care planning (ACP). 3 MI may serve as a useful approach to bridge the gap between intensive clinician-led programs, and self-administered tools to promote ACP engagement. We developed and pilot tested an MI intervention for ACP.
The MI manual was written in an iterative process by an interdisciplinary team with expertise in MI and ACP. MI sessions were delivered by two health psychologists who were trained in general MI through a two-day workshop and received additional feedback during role-playing sessions. Sessions were conducted by telephone, audio-recorded, and reviewed using a modified version of the Independent Tape Rater Scale (ITRS), a reliable and valid measure that yields MI adherence and competence scores on 7-point Likert scales from not at all/very poor to extensively/excellent for five fundamental and five advanced MI strategies. 4 The ITRS also assessed motivation for participation in ACP at the beginning and end of each session using a 7-point scale.
The MI intervention consists of four steps as follows: (1) elicitation and clarification of patient's understanding of and current engagement in ACP, (2) building motivation for ACP, (3) developing a change plan, and (4) summarizing the overall discussion. ACP is discussed in terms of four behaviors as follows: (1) appointing a healthcare agent; (2) communication about the patient's values, with an exercise examining attitudes toward quality versus quantity of life; (3) completion of advance directives (ADs); and (4) ensuring that ADs are in the medical record. The elicit-provide-elicit approach is used to deliver ACP education in an MI-consistent manner. MI sessions were conducted with four male and two female veterans ranging from 64 to 75 years (mean 68.3; standard deviation [SD] 4.8) receiving treatment for post-traumatic stress disorder (n = 1), major depressive disorder with anxiety (n = 1), cancer (n = 2), and multiple chronic conditions (n = 2). Ratings for MI adherence and competence (Fig. 1) demonstrate that all sessions were delivered with at least adequate proficiency for both fundamental and advanced MI strategies. Panel C illustrates high levels of motivation for ACP engagement at the beginning of the sessions that nonetheless increased further by the end. The sessions lasted a mean (SD) of 34.9 (6.5) minutes, with a range of 26.7–46.0. Clinicians spent most time on clarifying values regarding quality versus quantity of life and preparing a change plan.
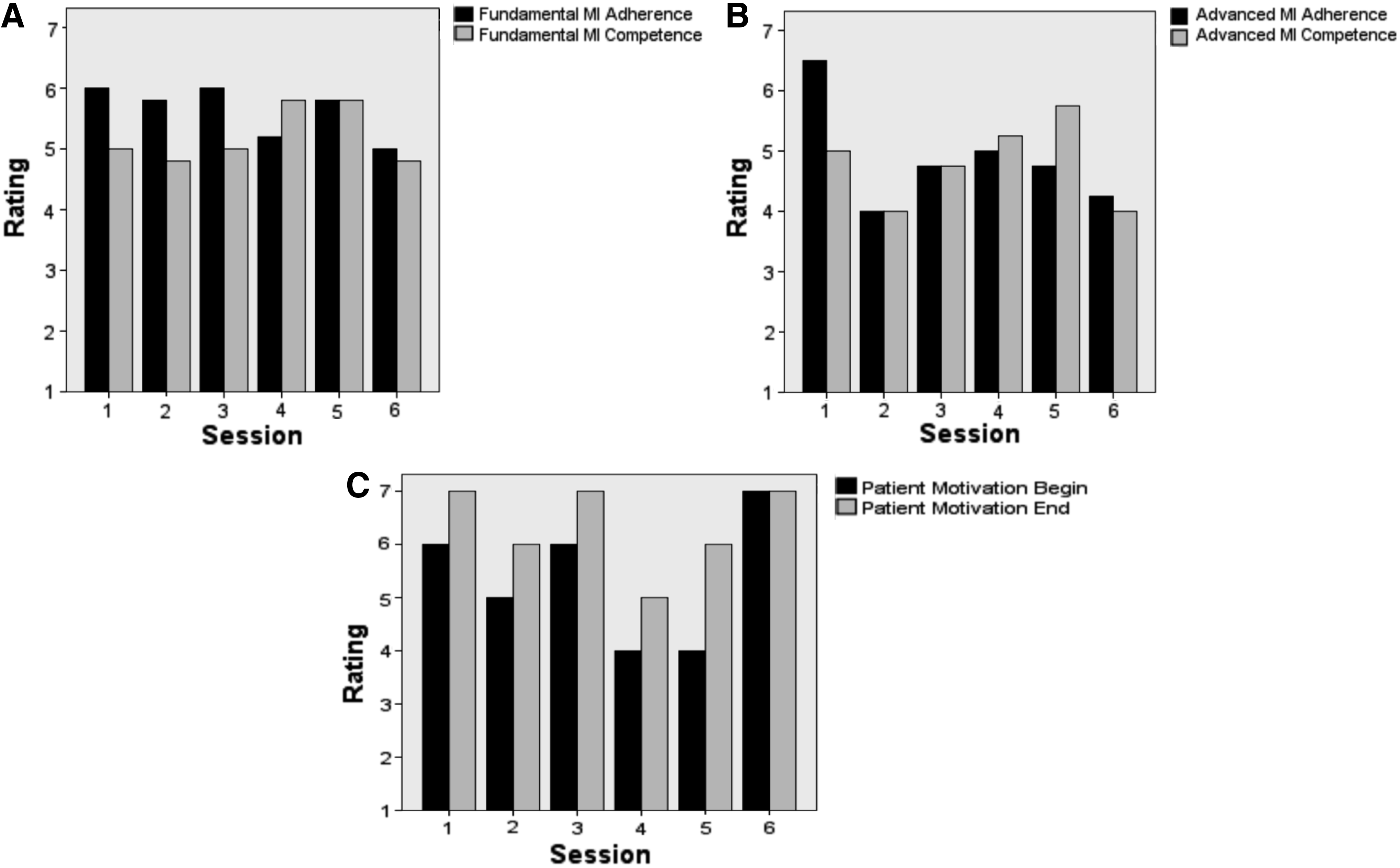
Panel
MI can be delivered in relatively brief sessions, reaching if not exceeding adequate thresholds of performance for both fundamental and advanced MI skills. Although it can be easy for the patient to become a passive recipient of information in ACP education, the MI intervention elicits the patient's active participation in this process, in the context of helping the patient to understand his or her motivations for engagement. Additional work is necessary to develop methods for involving surrogates and to examine clinical outcomes in larger samples.
Footnotes
Acknowledgments
This study was supported by Merit Review Award Number I01 HX HX002062 from the U.S. Department of Veterans Affairs Health Services Research and Development Service of the VA Office of Research and Development. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.