
Abstract
Abstract
Background:
Patient activation—or knowledge, confidence, and skill managing overall health—is associated with improved health behaviors such as exercise; it is unknown whether it is associated with advance care planning (ACP).
Objective:
To determine whether patient activation is associated with ACP.
Design:
This is a cross-sectional study.
Setting/Subjects:
A total of 414 veterans (≥60 years) with serious and chronic illness enrolled in an ACP trial.
Measures:
Patient characteristics and self-report surveys included the validated 13-item patient activation measure (PAM, five-point Likert) (e.g., “Taking an active role in your own healthcare is the most important factor…”) categorized into four levels (e.g., Level 1: “disengaged and overwhelmed” to Level 4: “maintaining behaviors”). ACP was measured with the ACP Engagement Survey including 57-item process scores (i.e., knowledge, contemplation, self-efficacy, readiness, 5-point Likert scale) and 25-item action scores (i.e., surrogate designation, yes/no items). Associations were determined with linear regression.
Results:
Participants were 71.1 ± 7.8 years of age, 43% were non-white, 9% were women, and 20% had limited health literacy. Higher PAM levels were associated with higher finances, having adult children, lower comorbidity, and more social support (p < 0.05). After adjusting for these characteristics, higher PAM (Level 4 vs. Level 1) was associated with higher ACP engagement (ACP process scores, 2.8 ± 0.7 vs. 3.8 ± 0.7 and action scores 9.7 ± 4.4 vs. 15.1 ± 6.0, p < 0.001).
Conclusions:
Higher patient activation to manage one's overall healthcare is associated with higher engagement in ACP. Interventions designed to foster general patient activation and self-efficacy to engage in health behaviors and disease management may also improve engagement in the ACP process.
Introduction
Advance care planning (ACP) is defined as a “process that supports adults at any age or stage of health in understanding and sharing their personal values, life goals, and preferences regarding future medical care.” 1 Studies suggest that individuals who do not engage in ACP may be more likely to receive care inconsistent with their goals and be less satisfied with the quality of care received and with communication with healthcare providers.2,3
Patient activation is a validated construct defined as the degree of knowledge, confidence, and skill that patients have to manage their overall health. 4 It is strongly associated with medication adherence, smoking cessation, cancer screening, weight loss and exercise,5–7 30-day postdischarge hospital utilization, and healthcare costs.8–10 It has also been associated with improved self-management of life-limiting diseases such as chronic obstructive pulmonary disease (COPD), heart failure, cancer, and chronic kidney disease.11–14 However, it is unknown whether patient activation is associated with engagement in the ACP process. This is important because studies have demonstrated that interventions can increase patient activation.15–17 Thus, interventions designed to improve overall health activation may also increase ACP engagement. Therefore, we examined whether a validated measure of patient activation was associated with engagement in ACP among older adults with serious and chronic illness.
Methods
This is a cross-sectional study of participant baseline responses to questionnaires before exposure to ACP interventions in the PREPARE randomized trial. 18 The study received approval from the University of California, San Francisco (UCSF) and San Francisco Veterans Affairs Medical Center (VA) Institutional Review Boards. Written informed consent was obtained for all participants. 19
As previously described, participants were recruited from several primary care clinics at the San Francisco Veterans Affairs Medical Center (VA) between April 2013 and July 2016. 20 Participants were included if they were ≥60 years of age, had ≥2 chronic conditions, had established care with a primary care provider (≥2 visits in the past year), and frequently accessed VA services (≥2 additional visits to a VA clinic, emergency room, or hospital admission within the past year). Exclusion criteria were dementia, moderate-to-severe cognitive impairment, blindness, deafness, delirium, psychosis, or active drug or alcohol abuse in the past three months. 20
ACP engagement was measured by the validated ACP Engagement Survey, a survey based on social cognitive and behavior change theories. 21 It includes 57 ACP behavior change process measures addressing decision-making associated with ACP behavior change. They include self-reported responses assessing ACP-specific knowledge, contemplation, self-efficacy, and readiness on an average five-point Likert scale. It also includes 25 yes/no action items on a 0–25-point scale, including identifying and asking surrogate decision makers, identifying and communicating goals for medical care, considering surrogate flexibility in decision making, and asking healthcare providers questions. 22
The patient activation measure (PAM) is a validated instrument designed to assess patient knowledge, skill, and confidence for overall general medical self-management (e.g., “How strongly do you agree with the statement: Taking an active role in your own healthcare is the most important factor in determining your health and ability to function”). 4 We used the 13-item PAM version. 23 Scores were produced from Likert responses fitted to a four-point scale and sorted into four validated stages of activation: Level 1: Not taking an active role; Level 2: Gaining confidence and knowledge to take action; Level 3: Taking action; and Level 4: Maintaining behaviors and pushing further. The PAM has been used in a variety of patient populations including adults with serious multimorbid conditions.4,9,24–26
We also assessed self-reported age, gender, race/ethnicity, education, financial circumstances, presence of adult children, and presence of a potential surrogate decision maker. We measured health literacy with the validated short test of functional health literacy (s-TOFHLA), 27 and social support with the 11-item Medical Outcomes Study Social Support Survey (MOS), 28 with scores ranging from 11 (no support) to 55 (full support). Comorbidity was measured by the Deyo adaption of the Charlson Comorbidity Index (CCI): score of 0 (no comorbidity) to >4 (severe comorbidity). 29
Statistical analyses
We conducted descriptive analyses stratified by PAM level. The association between PAM levels and patient characteristics was evaluated by unadjusted linear regression. Means and standard deviations for ACP Engagement Process and Action scores were stratified by PAM level. After controlling for variables associated with PAM, linear regression was used to assess associations between PAM level and ACP Process and Action scores, with p-for-trend calculated across the four PAM levels. R-squared was used to describe the portion of the variance in ACP scores attributed to variables in regression analyses. Beta coefficients and standardized beta coefficients were used to describe the contribution of variables to the model.
Results
Four hundred fourteen veterans participated (Table 1). The mean age was 71.1 ± 7.8 years, 9% were women, 43% identified as non-white, 20% had limited health literacy, 66% had adult children, and 92% could identify a potential surrogate.
Participant Characteristics
significant trend, p < 0.05.
PAM-1, “Not taking an active role”; PAM-2, “Gaining confidence and knowledge to take action”; PAM-3, “Taking action”; PAM-4, “Maintaining behaviors and pushing further”; SD, standard deviation.
CCI, Charlson Comorbidity Index Score, 0 = no comorbidity, 1–3 = average comorbidity, >4 = severe comorbidity.
MOS, Medical Outcomes Study Social Support Survey, 11 = no support, 55 = full support
PAM, patient activation measure.
Eight percent of participants tested in the lowest PAM Level 1, followed by 20% in PAM Level 2, 50% in PAM Level 3, and 21% in the highest PAM Level 4. Higher PAM levels were associated with higher finances, having adult children, lower comorbidity, and more social support (p < 0.05), but not other characteristics (Table 1).
In unadjusted linear regression, participants in the highest versus lowest PAM Level (1 vs. 4) had overall higher ACP process scores, 3.8 versus 2.8 on a 5-point scale, and action scores, 15.1 versus 9.7 on a 25-point scale, p < 0.001. PAM levels accounted for 14.5% of the variance of overall ACP process scores and 8.3% of overall ACP action scores.
After adjusting for finances, having adult children, comorbidity, and social support, a higher PAM level was associated with higher overall ACP process scores, p < 0.001 (Fig. 1) and higher overall ACP action scores, p < 0.001 (Fig. 2). In addition, all ACP process subscores of knowledge, contemplation, self-efficacy, and readiness were associated with higher PAM levels, p < 0.001 (Fig. 1). PAM was also associated with ACP action subscores of quality of life, p < 0.001, flexibility, p < 0.001, and asking doctors questions, p < 0.001 (Fig. 2). PAM was not associated with ACP action subscore of surrogate decision makers.
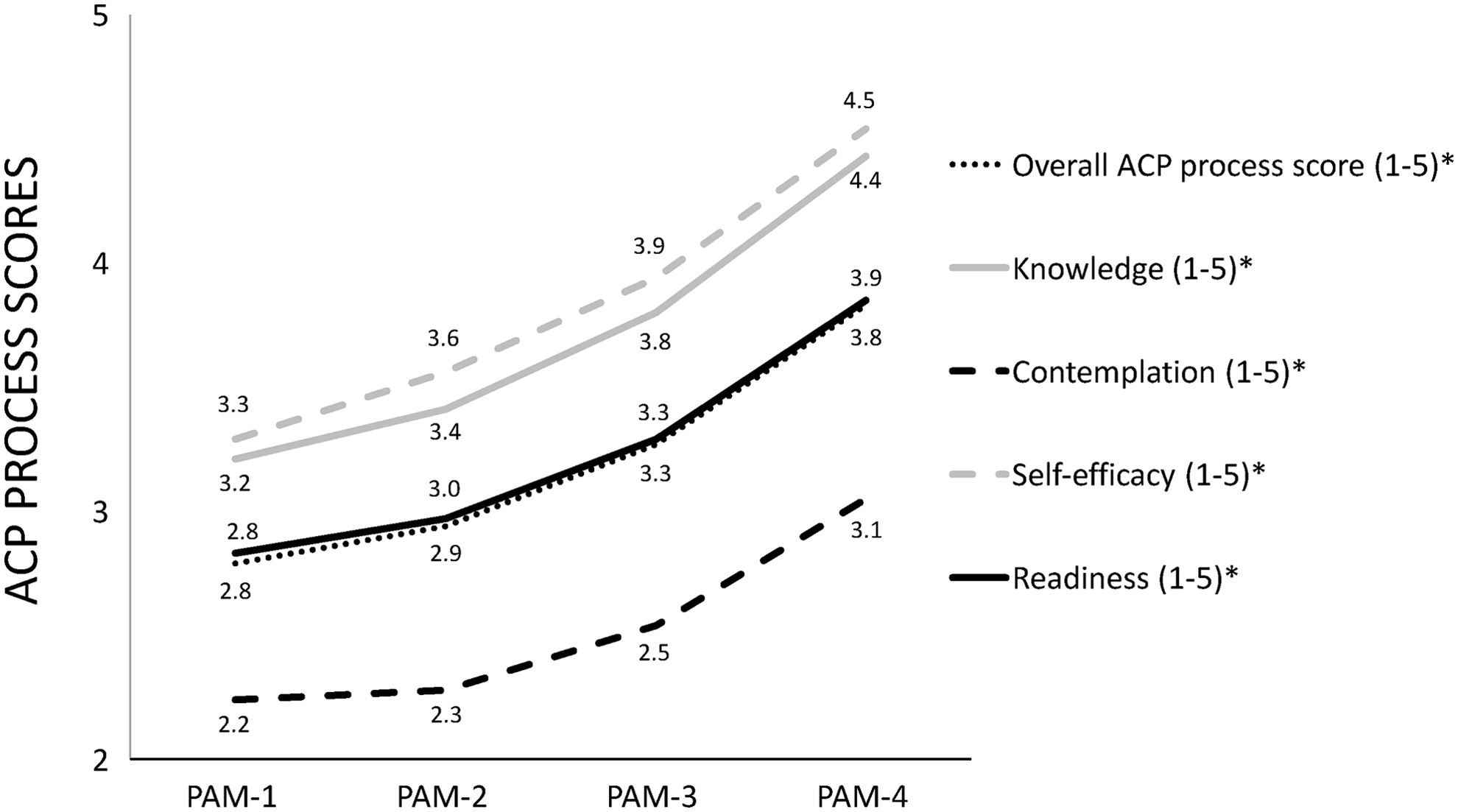
ACP process scores. *p-for-trend <0.001, linear regression adjusted for variables associated with PAM level (having adult children, being unable to financially have ends meet, comorbidity, and social support). PAM, patient activation measure.

ACP action scores. *p-for-trend <0.001, linear regression adjusted for variables associated with PAM level (having adult children, being unable to financially have ends meet, comorbidity, and social support).
In adjusted models, higher PAM levels and greater social support were associated with higher ACP behavior change process scores (Table 2). Higher PAM levels, higher health literacy, greater social support, and lower comorbidity were associated with higher ACP action scores. Collectively, the models accounted for 28.8% of the variability in overall ACP process scores and 16.4% of the variability in overall ACP action scores. PAM levels independently accounted for 4.8% of the variance of the overall process scores (p < 0.001) and 3.6% of the overall action scores. Only social support contributed more to ACP than PAM levels, accounting for 11.9% and 5.6% of the variance, respectively.
Factors that Contribute to Overall Advance Care Planning
Multiple regression, p < 0.05. Beta coefficients represent the degree of change to the overall ACP process/action score for each unit of change of individual predictor variables. Standardized beta coefficients demonstrate the strength of the effect of each predictor variable on the overall ACP process/action score relative to the other predictor variables in the model.
ACP, advance care planning.
Discussion
In this study, older veterans with higher patient activation had higher levels of ACP engagement than those with lower patient activation. Patient activation has been shown to be important for self-management in individuals with life-limiting conditions including COPD, heart failure, cancer, and chronic kidney disease.11–14 However, this is the first study to demonstrate that patient activation is a key component of ACP.
Our results suggest that older adults participate in a range of ACP behaviors that correspond to their level of activation. Activation was specifically associated with all subdomain behavior change processes such as knowledge, contemplation, selfefficacy, and readiness to engage in ACP. Although most were able to name a potential surrogate decision maker, an activity not affected by PAM levels, only those individuals with higher patient activation completed more complex ACP activities, such as discussing and documenting values and quality of life and asking clinicians questions. 18 The mechanism in which patient activation is tied to ACP is not clear. However, given that patient activation was most strongly associated with ACP process measures, one hypothesis is that patient activation enhances the motivational, contemplation, and self-efficacy components of ACP preparation that precede ACP action in behavior change models. Consequently, those with higher patient activation may be primed for ACP behavior change.
Besides social support, PAM explained a greater portion of the variance in ACP scores than literacy or comorbidity; however, all three factors are important codeterminants and have been identified as key contributors to patient activation in other self-management behaviors.30–32 However, the overall variance explained by PAM was low, likely representing the complexity of many contributing factors to the ACP process. This study supports a dynamic ACP paradigm consistent with self-management constructs of empowerment, skill building, and active continuous engagement rather than traditional approaches that often result in singular passive documentation of ACP wishes.
This study offers practical implications for clinicians. First, PAM has been successfully used to screen patients at risk for suboptimal health-sustaining behavior and may help identify patients at risk for deficient ACP who may require additional support.5–7 Second, although providers may be unable to improve social support for patients, interventions designed to increase general patient activation may improve engagement in ACP, especially for socially isolated adults. Third, easy-to-use ACP tools designed to increase patient empowerment and activation may help overcome health literacy needs of diverse patient populations.18,33
Limitations
There are some limitations in this study. In this cross-sectional study, we are unable to infer causality between patient activation and ACP. Further research is needed. This study took place in one area of the country and included mostly male veterans, which may limit generalizability, although close to half were nonwhite and the percentage of women is representative of the VA population.
Conclusion
Higher patient activation to manage one's overall healthcare is associated with higher engagement in ACP. Interventions designed to foster general patient activation and self-efficacy to engage in health behaviors and disease management, including easy-to-use ACP tools, may also improve engagement in the ACP process.
Footnotes
Author Disclosure Statement
No competing financial interests exist.