
Abstract
Abstract
Background:
Complaints are an opportunity for patients and family members to report allegations of substandard care. No prior studies have examined complaints in hospice care and what might be learned from them.
Objectives:
To describe hospice complaint trends, characterize state investigation practices, and assess the relationship between complaints and hospice agency traits of interest.
Methods:
Retrospective analyses merged hospice complaints from 2005 to 2015 with agency characteristics from Medicare Cost Reports and Provider of Service files.
Measurements:
Annual rates of complaint allegations and deficiencies on a per agency and per 10,000 patient days basis, nationally and by state. Likelihood of having any complaint allegations and deficiencies. Mean days to investigation and substantiation rates, by state. Hospice traits of interest were accreditation and profit status.
Results:
Between 2005 and 2015, a total of 12,931 complaint allegations were received about hospice care, resulting in 6710 complaint deficiencies. Allegations centered on concerns about quality of care (45%), patients' rights (20%), and administrative/personnel concerns (14%). Complaint rates varied across states but were generally quite low—in a given year, 88% of agencies nationally did not have any complaints. Complaint investigation practices varied considerably across states, with 34% of complaints substantiated. For-profit agencies were 1.33 and 1.52 times more likely relative to not-for-profits to have a complaint allegation and deficiency, respectively.
Conclusions:
Although the number of complaints was low overall, these data have the potential to convey insights about the care that hospice agencies provide. Greater attention to the perspectives of patients and their families, even when focused on shortcomings in care, can help ensure transparency and accountability and promote higher quality hospice care.
Introduction
A
By definition, complaints reflect the perspectives of the individuals who make them, typically patients and families. Rather than adhering to a standardized oversight or certification schedule, complaint allegations arise in real time and reflect instances where the burden of filing the complaint is outweighed by the potential benefit of conveying information about the alleged harm. In a setting such as a nursing home, complaint investigations complement and wrap around extensive oversight activities that occur on a regular basis. In less heavily regulated settings like hospice, the focus of this study, complaints are an important mechanism to focus attention on quality problems and other issues that might otherwise go unchecked.
The question of what can be learned about healthcare providers from their complaint histories is not new. Prior studies of nursing homes, hospitals, and physicians have examined the frequency of complaints and their correlation with provider and facility traits of interest (e.g., factors that might be correlated with quality of care, such as profit status, provider experience, and performance on other quality metrics).1–7 Across healthcare settings, complaints generally are few in number and concentrated among a relatively small portion of providers. Consequently, complaints offer a somewhat narrow and negatively focused window into the care that patients receive.
We are not aware of any previous studies of hospice complaints. To address this gap, the following analyses will describe hospice complaint trends between 2005 and 2015, characterize related state investigation practices, and assess the relationship between complaints and hospice agency accreditation and ownership status. The analyses will use data on all hospice complaint allegations and the resulting deficiencies collected by the Centers for Medicare and Medicaid Services (CMS), merged with hospice agency traits over the same time period.
Methods
Overview
This study is a longitudinal analysis of hospice complaint allegations and deficiencies conveyed by state oversight agencies to the CMS between January 1, 2005, and December 31, 2015. Through their licensure authority, state oversight agencies (typically State Departments of Health) collect, monitor, and investigate hospice consumer complaints. Although some uniform standards exist, there can be considerable cross-state variation in these processes.8–10 The analyses describe trends in hospice complaints over time, detail state complaint rates and investigation processes, and assess the relationship between complaints allegations and deficiencies and hospice agency traits of interest. The analyses merge complaints information with agency characteristics from Medicare Cost Reports and Provider of Service (POS) files.
Data sources
Hospice complaint allegations and complaint deficiencies data
We obtained information from the CMS on hospice complaint allegations and complaint deficiencies. Complaint allegations include all complaints reported to state oversight authorities, including those that are not substantiated. Multiple allegations may be included in a single complaint that is filed against an agency (i.e., an individual could allege more than one instance of unsatisfactory care). Complaint deficiencies are the subset of complaint allegations that are substantiated and result in citations for noncompliance.
States report information about all complaints that are received to the CMS, including the date the complaint is received, the nature of the allegation(s), the date the complaint is investigated or closed, and whether or not the complaint is substantiated. In addition, these data include information about complaints that result in deficiencies. Deficiency information identifies the aspect in which the hospice agency was out of compliance (e.g., in care planning, quality assessment and performance improvement, or patients' rights).
Medicare Cost Reports
We used Medicare Cost Reports to obtain information about hospice ownership and the number of patient days for each study year. All Medicare-certified hospice agencies must submit Cost Reports yearly to the CMS, and these data are publicly available. As detailed elsewhere, 11 we have coded each hospice agency nationally over time as for-profit, not-for-profit, or government-owned.
POS files
Similar to Medicare Cost Reports, the POS data collection requires Medicare-certified providers to self-report data to the CMS. POS files contain administrative information and limited practice data. For these analyses, we incorporated information on hospice agencies' accreditation status (yes/no) and the year the agency was initially certified by Medicare, from which we calculated the “agency age” at the time of the complaint. Across the 11-year study period, we dropped 405 agency-year observations from analyses that included accreditation status, as this variable was missing from these agencies' POS record in a particular year.
Analyses
The analyses focus on several elements related to complaints made about hospice care in the United States between 2005 and 2015. First, we described the number and type of hospice complaint allegations and complaint deficiencies over time. Second, we detailed the rate of hospice complaints and key complaint investigation metrics across states. In particular, we examined the mean days between the report of an incident and its investigation and the rate at which complaints are substantiated or confirmed as true. Although not formal measures of investigative rigor or quality, each of these metrics gives an indication of the variation that exists across states and has been examined previously in the context of nursing homes.3,12 Third, using the hospice agency-year as the unit of analysis, we calculated complaint allegation and complaint deficiency rates per agency for accredited and unaccredited hospice agencies across ownership types. Our choice of these hospice agency traits reflects their use in prior analyses of hospice care, in particular an extensive literature documenting relative gaps in care among for-profit relative to not-for-profit agencies.13–18 To account for differing agency size, we also calculated these rates per 10,000 patient days, with very similar results (data not shown). We tested for significant differences in the outcomes of interest using t tests to compare accredited and unaccredited agencies and ANOVA to compare the three ownership categories. Finally, we used regression models to explore the relationship between hospice agencies' ownership and accreditation status and whether the agency had any (i) complaint allegations and (ii) complaint deficiencies in a given year, controlling for agency size, year, and state. Given the large percentage of agency-year observations with no complaints, we modeled the outcomes of interest as dichotomous (yes/no) and used logistic regression models. As a sensitivity check, the model is run without state fixed effects (data not shown), producing very similar results.
Results
During the 11-year study period (2005–2015), a total of 12,931 complaint allegations were received about hospice care in the United States, resulting in 6710 complaint deficiencies (Fig. 1). The number of complaint allegations received annually almost doubled over the study period (with a low of 777 in 2005 and a high of 1482 in 2013). In contrast, the number of complaint deficiencies grew more slowly (with a low of 465 in 2005 and a high of 728 in 2013), leveling off in the last year observed. Important context to interpret these increases is that the number of hospice agencies and hospice patient days increased considerably over the study period. On a per agency basis, the rate of complaint allegations increased by around 27% over the study period, and the rate of complaint deficiencies decreased slightly, given that the number of agencies increased from 2769 agencies in 2005 to 3915 agencies in 2015.
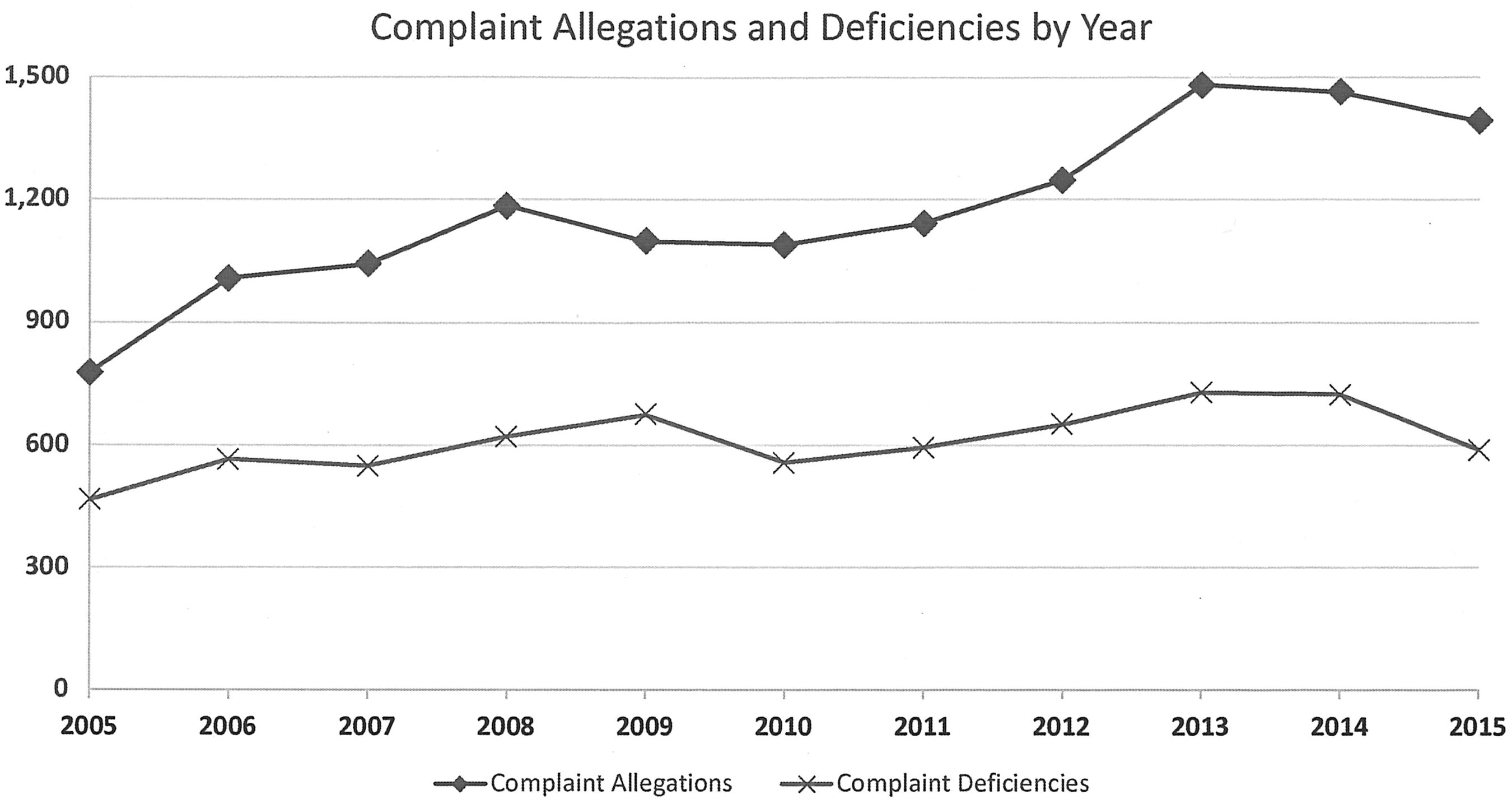
Complaint allegations and complaint deficiencies by year. Complaint allegations and complaint deficiencies data are from the Centers for Medicare and Medicaid Services. One hundred fifty-four allegation observations were dropped because the provider number and year did not correspond to the Medicare Cost Report data. One hundred thirty complaint deficiencies were dropped because the provider number and year data did not correspond to Cost Report data.
Complaint allegations largely centered on concerns about quality of care (45%), patients' rights (20%), and administrative or personnel concerns (14%) (Table 1). The categories into which complaint deficiencies fall are distinct, as they reflect specific statutory requirements assessed by surveyors (documented as L-tags or deficiencies). The most common types of complaint deficiencies over the study period are care planning (29%), clinical records (12%), organizational and administrative concerns (10%), the delivery of core services (10%), and issues with patients' rights (10%).
Complaint allegations data are from the Centers for Medicare and Medicaid Services. One hundred fifty-four allegation observations were dropped because the provider number and year did not correspond to the Cost Report data.
Complaint deficiencies data are from the Centers for Medicare and Medicaid Services. One hundred thirty complaint deficiencies were dropped because the provider number and year did not correspond to the Cost Report data.
Other allegations include general, life safety code, misappropriation of property, other services, physical environment, state licensure, state monitoring, transplant, facility administration/physical environment, analytic, preanalytic, and postanalytic.
Other deficiencies include hospices that provide inpatient care directly; short-term inpatient care, medical director; personnel qualifications; licensed professional services; infection control; nursing; compliance with federal, state, and local laws; physical therapy, occupational therapy, speech-language pathology; and furnishing of noncore services.
SNF, skilled nursing facility; INF, intermediate care facility.
Across states, the rates of complaint allegations and complaint deficiencies varied, as did complaint investigation processes (Table 2). Overall, the rates of complaint allegations and complaint deficiencies were quite low across most states on a per agency basis. In fact, only two states, Florida and Texas, had more than 1 complaint allegation per agency per year, and only two states, Florida and Delaware, had more than 0.50 complaint deficiencies per agency per year.
State, agency, and patient data from Cost Reports and POS files. Data include all 50 U.S. states and D.C. Averaged data calculated over 11 years, 2005–2015.
Complaint allegations and complaint deficiencies data are from the Centers for Medicare and Medicaid Services. One hundred fifty-four allegation observations were dropped because the provider number and year did not correspond to the Cost Report data. One hundred thirty complaint deficiencies were dropped because the provider number and year did not correspond to the Cost Report data.
One hundred one observations for days to investigation were coded as “missing” because days to investigation reported as negative.
Values greater than two years coded as “missing.”
POS, Provider of Service.
On an absolute basis, only 8 states received more than 25 total complaint allegations per year, on average. Still, the disposition of complaint allegations after intake varied considerably across states. The mean number of days between when a complaint was received and when the complaint survey or investigation occurred was 67 days, ranging from a low of 6 days in North Dakota (which received fewer than one allegation per year on average) to a high of 239 days in Oklahoma (which received 36 complaint allegations per year on average). In 12 states, more than 90 days passed, on average, between the receipt of the complaint and the complaint survey. Around one-third of all complaints (34%) were substantiated nationally over the study period. Fifteen states substantiated fewer than a quarter of all complaints that were received.
Table 3 displays unadjusted annual rates of complaint allegations and deficiencies by accreditation and ownership status. We present the per agency per year results, which are consistent with the per 10,000 patient days analyses (data not shown). The national rate of complaint allegations was 0.35 allegations per agency per year or an average of 1175 allegations over 3357 agencies each year. The per agency per year rate of allegations was not significantly different across accredited and unaccredited agencies (p = 0.74). In contrast, complaint allegation rates were significantly different across hospice ownership types (p < 0.001). For-profit agencies had the highest complaint allegation rate (0.42 per agency per year or an average of 794 allegations over 1904 agencies each year), around 1.4 times that of not-for-profit agencies (0.29 or an average of 358 allegations over 1226 agencies each year). Although they are a very small portion of the hospice market, government agencies had the lowest complaint allegation rate on a per agency basis (0.10 or an average of 23 allegations over 227 agencies each year). The rate of complaint deficiencies followed similar patterns: the national annual rate per agency was 0.18 (608 deficiencies over 3357 agencies), with accredited and unaccredited agencies having similar rates (p = 0.11). Complaint deficiencies were again significantly different across ownership types (p < 0.001). For-profit hospice agencies had 1.8 times as many complaint deficiencies per agency (0.23 or 439 deficiencies over 1904 agencies each year) relative to not-for-profit agencies (0.13 or 159 deficiencies over 1226 agencies) and 5.5 times as many relative to government agencies (0.04 or 9 deficiencies over 227 agencies).
Agency, patient, profit, chain, and accreditation data from Cost Reports and POS files. Data include all 50 U.S. states and D.C. Averaged data calculated over 11 years, 2005–2015. Accredited and unaccredited agencies, patients, allegations, and deficiencies may not sum to total of ownership type due to rounding. Four hundred five agency-year observations were dropped because accreditation status was missing from the agency's POS record.
Complaint allegations and complaint deficiencies data are from the Centers for Medicare and Medicaid Services. One hundred fifty-four allegation observations were dropped because the provider number and year did not correspond to the Cost Report data. One hundred thirty complaint deficiencies were dropped because the provider number and year did not correspond to the Cost Report data.
We tested for significant differences in complaint and complaint deficiency outcomes using t tests to compare accredited and unaccredited agencies and ANOVA to compare hospice ownership types.
Reflecting the low number of complaint allegations and deficiencies across hospice agencies, 88% and 95% of all agencies, respectively, had zero complaint allegations and complaint deficiencies in a given year. Even looking over the previous five years, the percentages were relatively high: 61% of all agencies had no complaint allegations over the previous five years and 79% had no complaint deficiencies (data not shown). The proportion of agencies with zero complaint allegations and complaint deficiencies in a given year was similar regardless of agencies' accreditation status (p = 0.67 and p = 0.05, respectively). Relative to other ownership types, modestly lower proportions of for-profit agencies had zero complaint allegations and deficiencies in a given year (p < 0.001).
Finally, Table 4 shows the regression results modeling the likelihood of having a complaint allegation and a complaint deficiency. Controlling for agency size, state, and year fixed effects, for-profit agencies were 1.33 times more likely to have a complaint allegation relative to not-for-profit agencies. Government agencies were 0.77 times as likely to have a complaint allegation relative to not-for-profit agencies. Accredited agencies were 0.78 times as likely to have a complaint allegation compared with unaccredited agencies. For complaint deficiencies, the results were similar except accreditation status had no significant effect. For-profit agencies were 1.53 times as likely to have a complaint deficiency relative to not-for-profit agencies. Government-run hospice agencies were 0.65 times as likely to have a complaint deficiency relative to not-for-profit agencies. The model without state fixed effects yielded very similar results for both hospice ownership and accreditation status.
Logistic regression models used to assess the relationship between hospice agencies' ownership and accreditation status and complaint outcome of interest, controlling for agency size, year, and state. Four hundred five agency-year observations were dropped because the accreditation status was missing from the agency's POS record.
CI, confidence interval.
Discussion
Our analyses offer insights into complaints about hospice care in the United States. The first and most basic finding is that the number of complaints filed against hospice agencies over the last decade was strikingly low. The overall rate of hospice complaints has been fairly steady over the last decade. In fact, the vast majority of hospice agencies do not have a complaint against them in a given year, and many do not have any complaints over longer time horizons either. These findings could reflect a general satisfaction with hospice quality of care, a notion supported by prior analyses of hospice satisfaction and experience with care.19–21 Alternately, the low rate of hospice complaints could reflect a lack of awareness on the part of patients and families about filing complaints, logistical or other barriers to filing a complaint, or some combination of these factors, as has been documented in other settings.3,8,22 Because hospice complaints occur in the context of a patient's terminal illness, for instance, it is conceivable that many patients and families are either unable or reluctant to complain formally about their care.
Most complaint allegations focus on things that directly impact patients and families—quality of care, patients' rights violations (e.g., around admission and discharge), and administrative and personnel concerns—making them especially salient when they do arise. Although the rate of complaints was low overall, we found modest associations about what types of agencies are more likely to have complaints lodged against them. Our analyses found that accredited agencies had a modestly lower rate of complaint allegations relative to unaccredited agencies; however, accreditation status had no significant relationship with the rate of complaint deficiencies.
Relative to not-for-profits, for-profit agencies, in aggregate, consistently had a higher rate of complaints across our analyses. For-profit agencies were around 1.5 times as likely as not-for-profits to have complaint allegations and deficiencies in a given year. Based only on our study data, it is impossible to know whether for-profit agencies' higher complaint rates reflect relatively poor quality of care (as has been reported in the literature13–18 ), a more activated patient population, differing expectations of care, or some combination of these and other unobserved factors. In fact, a key limitation of our study is that it lacks information about the patients receiving care from individual hospices, not only complainants but also others who do not complain. It is possible that the differential complaint rates we report reflect unobserved differences in patient populations (e.g., education and socioeconomic status) that might affect their ability or propensity to complain as opposed to instances of substandard care.
Although complaints are fairly rare across most states, complaint investigation processes appear to vary widely, with many states lagging in the number of days between when a complaint is received and when it is ultimately investigated. Given the fact that hospice quality oversight is relatively minimal, 23 it is concerning that some states appear to be relatively ineffective in investigating the few complaint allegations they do receive, in particular around the timeliness of initiating investigations. The wide variation in substantiation rates also is concerning, although it is unclear whether this variation reflects weaknesses of investigative processes or other factors about the complaints themselves. Importantly, any potential shortcomings in hospice oversight likely reflect broader challenges faced by states in assuring quality of care across other settings, such as nursing homes.24–27
In the context of our findings, hospice complaints might best be viewed as a signal of potential problems rather than as a representative view of an agency's quality of care. This limitation stems not only from the low number of complaints in our data (e.g., the vast majority of agencies look identical in a given year based only on their complaint profile) but it also reflects the fact that complaints are a negatively focused measure. Even if fewer hospice agencies were “complaint free,” this would not necessarily imply that they offered high-quality patient- and family-centered care. An analogous challenge arises in the context of nursing home quality assessment, where lower rates of pressure ulcers, falls, restraints, and even survey deficiencies are not necessarily indicative of high-quality care.28,29
The broader challenges of assessing and monitoring hospice quality of care have received increased attention among clinicians, patients, and policymakers in recent years. Media and governmental reports have alleged instances of deficient care, questionable enrollment and billing practices, and insufficient regulatory oversight.23,30–33 At the same time, the science of hospice quality measurement has steadily advanced, along with modestly enhanced oversight requirements. The Affordable Care Act of 2011 authorized the Hospice Quality Reporting Program (HQRP) and its creation of the Hospice Compare website, and the IMPACT Act of 2014 established the first requirements for how often hospice agencies must be recertified (every three years).
Embedded in these quality-related efforts is a commitment to incorporate the perspective of patients and their families. In addition to the clinically focused measures of the Hospice Item Set, the HQRP includes the newly developed Consumer Assessment of Healthcare Providers and Systems (CAHPS) hospice survey focused on the patient and family experience. The hospice CAHPS survey is completed by the primary caregiver of the hospice recipient and is administered two months following a patient's death.34,35 Required as a Medicare condition of participation for agencies with at least 50 hospice deaths over the prior year, information from the CAHPS survey is being submitted by hospice agencies nationwide and has recently become part of the Hospice Compare tool.
In the context of these trends, complaints could be seen as a complement to the CAHPS Hospice Survey, especially when CAHPS survey results differ little across hospice agencies. Beyond the primary use of complaints in ongoing quality assurance activities, which should continue, complaints might be incorporated into public reporting efforts, as they are for nursing homes. Even if complaints arise rarely, seeing a higher number of patient complaints detailed on a tool such as Hospice Compare could help patients and their families identify possible lapses in care and prompt useful conversations between physicians, patients, and families about local hospice agencies and the care they provide. To inform consideration of such an approach, further research could investigate the correlation between hospice complaints and other validated quality metrics, in addition to exploring more fundamental aspects of complaint intake and investigation processes across states.
This study presents the first national evidence about hospice complaints. Although the number of complaints over the last decade has been quite low overall, these data have the potential to convey important insights about the care that hospice agencies provide to their patients. Perhaps even more important, monitoring hospice complaints and ensuring their robust investigation should be essential components of hospice quality assurance and fit well with an increased emphasis on hospice quality assessment and oversight. Ultimately, greater attention to the perspective of patients and their families, even when it focuses on shortcomings in care, can help ensure transparency and accountability and promote higher quality hospice care overall.
Footnotes
Acknowledgments
We thank Haiden Huskamp and Joan Teno for comments on a previous draft. This work was funded by the Gordon and Betty Moore Foundation.
Author Disclosure Statement
No competing financial interests exist.