
Abstract
Abstract
Background:
Even though no evidence suggests tube feeding is beneficial for individuals with advanced dementia, many are still tube fed.
Objective:
To assess perceptions of hospital staff regarding reducing tube feeding (RTF) of patients with advanced dementia.
Design:
Cross-sectional survey.
Setting:
A regional teaching hospital in Taipei, Taiwan.
Subjects:
Hospital staff (n = 624), including physicians, nurses, dieticians, paramedical personnel, social workers, volunteers, attendants, and administrators.
Measurements:
Anonymous questionnaires.
Results:
The overall awareness of RTF for advanced dementia patients averaged 10.2 ± 3.74 points (maximum, 19 points) among all respondents. Among the different hospital professions, dieticians scored the highest, whereas nurses and attendants/volunteers had relatively low scores. Over half of respondents (57%) agreed tube feeding is the best choice for advanced dementia with dysphagia. Physicians of different specialties had significantly different responses toward RTF with regard to the belief that tube feeding reduces the risk of aspiration pneumonia, referring patients who refuse tube feeding to other health care team members, and the belief that family members would be able to accept the patient's death along with insufficient food/fluid intake. Only 35.1% of respondents believed they were able to implement comfort feeding.
Conclusions:
The present survey shows a persistent knowledge gap among various health care professions regarding tube feeding of patients with advanced dementia. Also, there is insufficient awareness about this subject, indicating that promotion of comfort feeding by enhanced training and communication within medical teams is essential to achieving better person-centered care and preventing unnecessary suffering.
Introduction
I
Dementia is caused by different diseases, such as Alzheimer's disease, vascular dementia, dementia with Lewy bodies, or Parkinson's disease. Although the presenting symptoms and underlying neuropathology may differ, dementia progresses slowly and is incurable. Advanced dementia is closely associated with eating problems, such as poor appetite and dysphagia. 3 Inadequate food and fluid intake can result in malnutrition and dehydration that increase morbidity and mortality; thus, tube feeding is often considered an option for nutritional intervention. However, tube feeding of advanced dementia patients may neither prevent aspiration pneumonia4,5 nor prolong life.6–11 Cochrane Reviews also indicate that there is no evidence of benefit in nutritional status or pressure ulcers, 12 and the Society for Post-Acute and Long-Term Care Medicine recommends oral assisted feeding instead of inserting a “percutaneous feeding tube in individuals with advanced dementia.” 13 Nonetheless, the decision to forgo artificial nutrition supplementation through feeding tube for advanced dementia patients, especially those near the end of their life, is not easy to make. Many choose to implement a feeding tube for nutritional support due to moral concerns as opposed to scientific evidence. 14
A case–control study using Taiwan's National Health Insurance Research Database found that as high as 67.4% of people with dementia was tube fed in their last year of life. 15 Moreover, a nationwide cohort study in Taiwan shows that, among persons with dementia who receive national health insurance payments for palliative care in 2009–2013, 65.38% was tube fed as a life-sustaining intervention. 16 Since, the 2016 Taipei Declaration for Prevention of Suffering was launched to advocate for palliative care that reduces the suffering of both patients and their families, emphasizing patient-centered care and recognition of the patient's personal feelings on comfort and dignity. 17 Therefore, feeding strategies for advanced dementia patients should be carefully considered and reformed accordingly.
Comfort feeding only (CFO) 18 has been recently introduced in Taiwan as a new concept of providing nutrition (and hydration) exclusively through careful hand feeding without using feeding tubes. Effective communication is necessary to promote CFO, and medical staff play a crucial role in facilitating the decision-making process and implementing it. For people with advanced dementia, withholding of tube feeding may be seen as practically starving the patients by family members. This issue is especially prominent in Asian countries, such as Taiwan, where “filial piety” is an important virtue. 19 Therefore, tube feeding is widely adapted for dementia patients with poor oral intake to give family members peace of mind and prevent malpractice disputes. However, tube feeding has not been shown to significantly improve the nutritional status of malnourished individuals. The result of a previous nutrition survey in Taiwan demonstrated that tube-fed nursing home residents (43.2% of total residents) had a higher prevalence of malnutrition than those who were fed orally. 20
There are several possible obstacles to promoting CFO. Comfort feeding of advanced dementia patients by hand requires more time and different caretaker skills compared with tube feeding. Additionally, hospital staff may have different considerations that are affected by their roles in the health care team, as a family member, or even as a patient themselves when choosing the feeding method for themselves or their loved ones. For example, a multicenter survey of >1000 medical staff in Japan showed that while 43.4% of respondents agreed to tube feeding for family members suffering from eating difficulties, only 14.4% would agree to for themselves. 21 Since reducing tube feeding (RTF) and implementation of CFO requires a team approach, we conducted a survey of various professions at a teaching hospital, including medical and paramedical staff, attendants, and administrators, to comprehensively assess perceptions of RTF use in patients with advanced dementia.
Materials and Methods
Survey design
We designed an anonymous, 19-item questionnaire that respondents used to evaluate the attitudes of hospital staff regarding RTF for advanced dementia. The reference questionnaire was developed from an advance care planning workshop, where 15 items regarding tube feeding were discussed. These items can be categorized as aggressive nutritional support at the end of life, medical outcome of tube feeding, decision making for self or family, and caring for individuals refusing tube feeding. The questionnaire was modified for our study purposes and reviewed and revised by two experts, a geriatric physician and senior social worker. Subjects responded to each question by selecting one of five levels: strongly agree, agree, neutral, disagree, or strongly disagree.
Participants
The survey was conducted at a teaching hospital with seven branches in Taipei city, Taiwan, which employs ∼9000 staff, excluding volunteers. We distributed the questionnaires during routine meetings of various clinical departments to ensure inclusion of different specialists and increase the response rate; meeting topics were not related to nutritional support for individuals with dementia. The survey was conducted once in every participating department to avoid repeat responses from the same persons. We invited physicians (general medicine, family medicine, psychiatry, rehabilitation medicine, and dentists), paramedical staff (dietitians, nurses, pharmacists, speech therapists, occupational therapists, physical therapists, psychologists, and respiratory therapists), attendants, volunteers, social workers, and administrative staff to participate. We collected personal information, including gender, age, and seniority defined as years of service at the professional position at the surveyed hospital, and prior experience at equivalent positions at other institutions. All participants received a printed explanation of the stages and characteristics of advanced dementia before the survey. The present study was reviewed and approved by the Taipei City Hospital Research Ethics Committee (TCHIRB-10510109-E). We were permitted to distribute 700 questionnaires among the various professions within the hospital, and formal informed consent was waived since participation (versus nonparticipation) in the survey was considered implied consent.
Statistical analysis
The percentages of respondents agreeing (strongly agree or agree) with each question were transformed to indicate the percentages supporting RTF. The average score of RTF awareness was calculated as the mean ± standard deviation of the total points from the 19 questions (1 point per question). Multiple linear regression was applied for predicting the effects of gender, age, profession, and seniority on overall RTF awareness. The differences between different physician specialties were analyzed by Chi-squared test. Statistical analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC), and the significance level was set at p < 0.05.
Results
A total of 700 questionnaires were distributed. After excluding those that were unfilled or incomplete, 624 (89.14%) completed questionnaires were used for further analysis. Among the completed questionnaires, 522 respondents were female (Table 1), and 48.24% of respondents were30–44 years of age. Only 7.21% had been employed by the hospital <1 year, whereas 16.67% had been employed ≥20 years. In terms of professions, nurses constituted the largest group of participants (44.55%), reflecting the typical staff structure of a hospital. The Cronbach's α coefficient was 0.80, indicating good internal consistency.
n = 624 total respondents.
Pharmacists, speech therapists, occupational therapists, physical therapists, psychologists, and respiratory therapists.
The mean overall RTF awareness score was 10.2 ± 3.74 points (maximum, 19 points) among all 624 respondents, with a broad range of scores for each question (Table 2). Among all respondents, 72.60% agreed that advanced dementia patients should be given enough nutrition and fluid in any situation regardless of disease severity, that is, only 19.39% supported RTF. There were 43.91% of respondents who believed that tube-fed individuals would survive longer, and only 28.37% of all respondents associated tube feeding with better quality of life. Many reported inappropriate (53.20%) or overuse (43.59%) of tube feeding in severely demented individuals.
Strongly Agree + Agree percentages were used to determine the RTF awareness percentage, except for Q1–Q6, Q8, and Q17, where disagree + strongly disagree percentages were used instead because disagreement with those questions reflects a positive view toward RTF.
Mean ± standard deviation calculated from all responses, counting 1 point for each answer in RTF awareness (strongly agree/agree as positive or strongly disagree/disagree as negative views); the maximum score was 19 points.
RTF, reducing tube feeding.
Personal comfort was highly valued by 81.89% of respondents with respect to tube feeding, and only 22.60% considered the outcome of nutritional support to be more important than the patient's comfort. While 43.10% of respondents reported they could accept patient to die with insufficient oral food/fluid intake, only 20.51% believed the patient's family would be able to accept the situation. The majority of respondents (88.30%) regarded the opinion of family members as an important factor when choosing to tube feed a patient. Less respondents (33.82%) indicated they would refuse tube feeding for themselves than for a family member (42.15%). Regarding views on implementation, 81.41% reported that the caregiver's ability was important when considering the use of tube feeding. Additionally, only 35.10% of respondents reported having the ability to implement the policy of RTF.
Multiple regression modeling of the effects of each variable on overall RTF awareness showed no significant differences in gender, age, and seniority (Table 3). Among the various hospital professions, dietitians had a significantly higher RTF awareness than physicians, followed by attendants/volunteers; the difference between physicians and attendants/volunteers was not statistically significant (p = 0.059). Although overall RTF awareness was similar between physicians of different specialties, the responses to three items showed significant differences (Fig. 1). Only 25% of rehabilitation specialists agreed that tube feeding has a low risk of aspiration pneumonia, whereas 91.67% of psychiatrists reported the opposite. Only 20% of physicians of other specialties (e.g., Chinese medicine, general surgery, etc.) would refer the persons who refuse tube feeding to other health care team members for further nutritional care, whereas 81.82% of dentists reported they would recommend it. Furthermore, 50% of physicians of other specialties believed that family members would be able to accept a relative with advanced dementia to die with insufficient oral food/fluid intake, whereas only 3.57% of family medicine physicians agreed with that opinion.
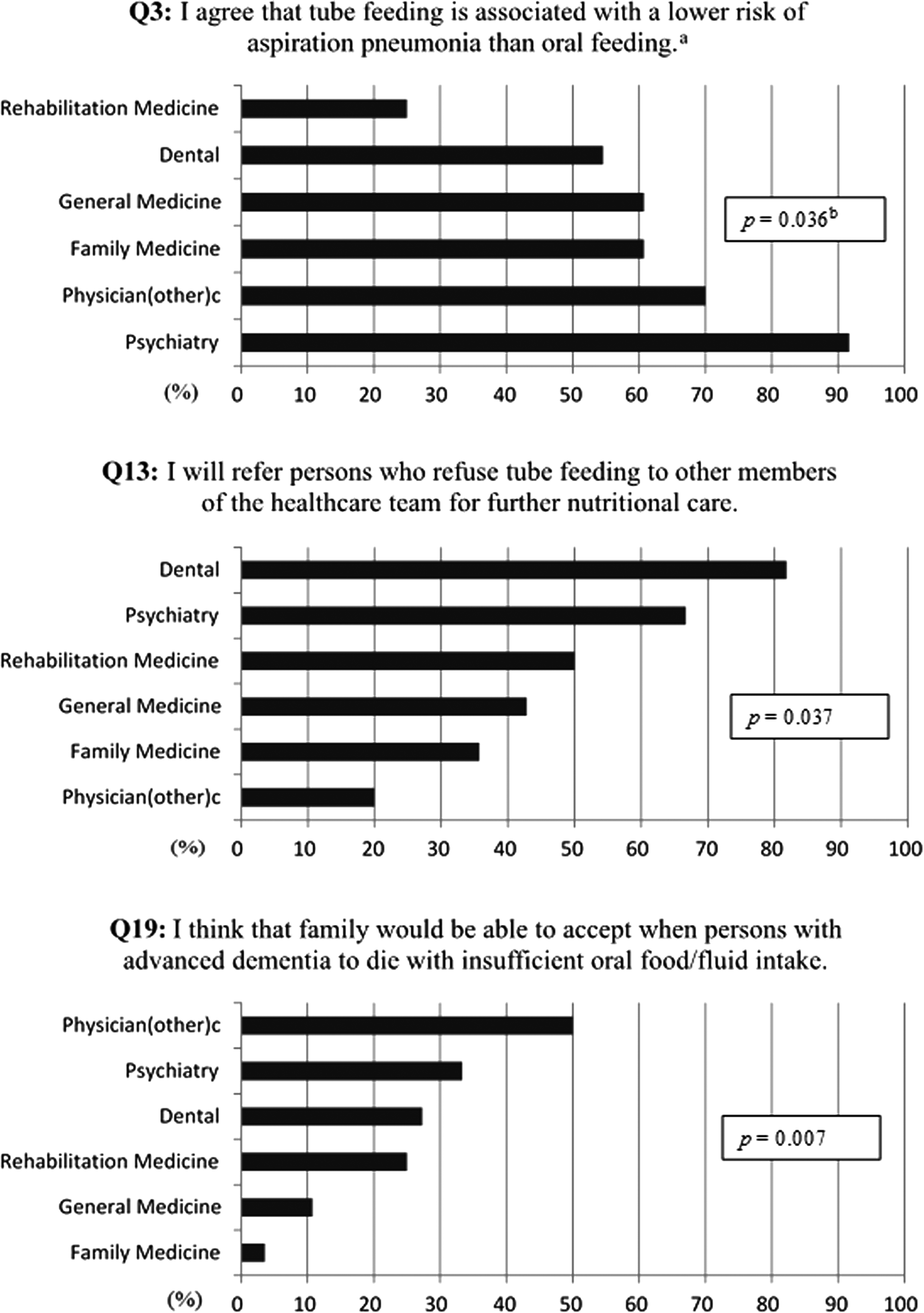
The three questionnaire items that showed significant differences between physician specialties. aA negative answer for this question indicates support for reducing tube feeding. bThe differences between different specialties were analyzed by Chi-squared test. cPhysicians of other specialties [physicians (other)] included physicians who specialized in general surgery, Chinese medicine, etc. The number of respondents per profession: 10 physicians (other), 12 psychiatrists, 11 dentists, 12 rehabilitation medicine physicians, 28 general medicine physicians, and 28 family medicine physicians.
p < 0.05; data were analyzed by multiple linear regression and adjusted for gender, age, profession, and seniority.
Pharmacists, speech therapists, occupational therapists, physical therapists, psychologists, and respiratory therapists
Discussion
In the present study, a 19-item questionnaire was designed to assess opinions on RTF, including whether advanced dementia patients should receive aggressive nutritional support through tube feeding and whether tube feeding can reduce aspiration pneumonia, prolong life, improve quality of life, or enhance medical outcomes. The questionnaire also addressed if tube feeding was considered comfortable and if the respondents would accept tube feeding for themselves and/or for a family member, the importance of family opinions, acceptance of forgoing artificial hydration and nutrition, ability to implement CFO, and referral of patients to other members of the health care team. Overall, the mean survey score was 10.2/19 points, showing that medical staff in the hospital surveyed currently do not have sufficient awareness or a consensus on RTF. The results also revealed different RTF awareness due to the staff profession and physician specialty.
With advancements in medical nutrition and their wide clinical application, patients having difficulties with oral intake can still be well supported nutritionally. However, dementia is irreversible and progresses slowly; a survey in a nursing home showed that the survival rate was under 50% in 1.5 years. 3 Particularly, it may be challenging to define the final stage of life in advanced dementia patients, which is a critical element in deciding when and whether to apply palliative care and/or CFO. Thus, dealing with eating problems in patients with dementia is a difficult yet unavoidable issue. Various studies and guidelines indicate that tube feeding is not recommended to ensure the quality of life and comfort of patients. 22 Caring for individuals with dementia takes a team approach 23 and requires effective communication and shared decision making 24 —a lack of consensus and/or essential understanding of options at any stage can lead to difficulties in medical decisions. The present results revealed profession to be the most decisive factor associated with RTF awareness, with dietitians having a significantly better understanding of RTF than physicians. Moreover, while attendants are potentially skilled at oral feeding, they showed little support for RTF. These differences may be related to the level of training on the topic. Deciding between tube and oral feeding also requires experience with both practices, especially considering that each involve different modes of care and dedication; time and manpower are important factors in CFO.
Although physicians are the opinion leaders in medical decision making, the current results showed significant discrepancies between physicians of different specialties regarding perception of RTF, risk of aspiration pneumonia with tube feeding, referring to other health care team members, and family member acceptance of patient death after feeding tube withdrawal. The results may reflect different responsibilities associated with medical decision making and experience in caring for patients with advanced dementia. Since most advanced dementia patients are elderly and often have multiple chronic diseases, decisions on feeding method often involve professionals from various specialties. This is why we chose to enroll hospital staff whose major responsibilities may not include caring for individuals with dementia. While physicians from different specialties may face the dilemma of choosing between feeding strategies, lack of consensus on possible treatment options, such as RTF, may hamper communication with patients and/or family members, as well as lead to increased confusion and anxiety. Therefore, strengthening interdisciplinary communication between members of the attending medical team is essential to enhancing the quality of care for dementia patients. On the other hand, medical caregivers may face feeding issues themselves or for a family member. Our research found that acceptance of tube feeding was not the same for self and family. This discrepancy likely reflects the effect of cultural and social expectations when making decisions for others as opposed to deciding for oneself.
The prognosis of advanced dementia patients may be affected by age, comorbidities, and quality of care, all of which can further complicate decisions related to proper treatment. The ultimate treatment goal for individuals with advanced dementia should focus on providing patient-centered care and quality of life. Moreover, it is crucial to view the patient and their family as a unit to provide transparent and adequate information on the pros and cons of each treatment. A recent study found that requests of patients or their family were the most common factor influencing the physicians to “choose wisely” regarding percutaneous feeding tubes for advanced dementia patients. 25 Hence, establishing an effective form of communication and a shared decision-making process are essential to resolving challenges faced by caregivers. 24 More importantly, hospital staff should be made aware that there is no evidence indicating individuals with advanced dementia benefit significantly from tube feeding. Since the prevalence of dementia is expected to dramatically increase in aging societies, it is equally critical to ensure a consensus on the issue of tube feeding among hospital staff and enhance public awareness of dementia and palliative care. Furthermore, action must be taken by the entire population of Taiwan to effectively implement the 2016 Taipei Declaration for Prevention of Suffering.
Although the present results provide a valuable reference for rethinking the practice of RTF and comfort care for advanced dementia patients, our study had some limitations. The survey was not conducted through random sampling, and the sample size only covered 7% of total staff in one hospital. Therefore, the results may not be fully representative of all staff positions. Also, the survey only delineated general seniority in the profession which may not reflect specific experience with caring for individuals with advanced dementia. Finally, we did not collect the opinions of patients with early stage dementia or their families. These issues are worth considering in future studies.
Conclusions
The present study showed a persistent knowledge gap among various hospital staff professions regarding tube feeding for individuals with advanced dementia. Moreover, respondents had insufficient awareness of RTF for advanced dementia patients. Introductory training and enhanced interdisciplinary communication are urgently needed for better shared decision making and implementation of high-quality person-centered care for advanced dementia patients.
Footnotes
Acknowledgments
The authors would like to thank all of the hospital staff who participated in the survey. They thank their colleagues Hsiao-Yun Hu and Shu-Yi Lin for professional assistance with data analysis; Yi-Fen Lin, Hsiu-Jung Tu, Ya-Han Chan, Tzu-Ying Lin, Pei-Li Hsu, Yi-Fang Chiu, and Chien-Chen Chou at Taipei City Hospital for their assistance with data collection. English Editing was provided by the Department of Medical Research at National Taiwan University Hospital (Taipei, Taiwan).
Author Disclosure Statement
No competing financial interests exist.