
Abstract
Abstract
Introduction:
Family conferences (FCs) may be important in communication. There is limited evidence about their value in palliative medicine. We examined specific information needs of patient-identified spokespersons (SP) and if the needs were met by a subsequent FC. Further data were collected on FC attendee characteristics, changes in SP distress, and SP assessment of FC value.
Methods:
We conducted a prospective observational study of the family SP perspective of consecutive first time palliative medicine FCs for cancer patients. The SP completed standardized questionnaires and a Distress Thermometer pre- and post-FC.
Results:
Seventy-eight FCs were eligible. Daughters/sons were the largest single attendee group. The median FC duration was 45 minutes (range 30–100). The location was usually at the bedside. Distress thermometer (DT) scores fell in 51%, rose in 26%, were stable in 23%, and were unaffected by patient presence. On average, there was a one-unit reduction in DT scores post compared to pre (p = 0.0059, 95% CI −1.5 to −0.3). The SP wanted information on a median of 15 (range 13, 17; 83%) questionnaire items beforehand; a median of 12 (range 10–14; 67%) were discussed. Overall, 62% of the total items were “needs met” in ≥50% of the SP.
Conclusions:
The FC attracted multiple participants; usually sons and daughters. Duration was typically 45 minutes and usually at the bedside. Nearly all SPs found the concept valuable both before and after the FC. Distress decreased or remained stable in most SPs. Most of their self-identified information needs were met. Thematic analysis of qualitative data supported the value of FC. Formal FCs are powerful and important communication tools in advanced cancer.
Introduction
C
The Harry R. Horvitz Center for Palliative Medicine is an acute care palliative medicine unit. 4 Most admissions are cancer-related. Over 400 FCs are completed each year. 8 All persons admitted are notified that FCs are a standard of care (subject to their explicit but informal approval) and given an overview of what to expect.9–11 The FC is scheduled when symptoms are controlled, the medical condition is reasonably stable, and the patient is appropriately aware of the illness. 12
There is no widely accepted definition of an FC. 13 Our concept is that of a formal prearranged multidisciplinary meeting between the clinical team and family members. The objectives are to enhance communication about the patients' clinical status and establish a therapeutic partnership with actual or potential caregivers. Our approach to FCs has been described elsewhere and follows a written protocol. 13 The patient appoints a family spokesperson (SP) beforehand. 13 The SP ensures that information from the medical team is communicated to the extended family and vice versa. 14 Distress in family members is common.15–17
FCs have been reported in various clinical settings. 18 Intensive Care Unit (ICU) studies show benefits to the family, healthcare team, and hospital operations. 18 One randomized controlled ICU study showed positive bereavement outcomes. 19 Cancer literature is sparse.6,7 A retrospective chart review (N = 123) found 59% of inpatient palliative medicine cancer FCs were attended by both patient and family. 20 In a follow-up prospective study (by the same program) of 140 consecutive FCs (attended by cancer patients), goals were discussed more than prognosis and death. 21
Palliative care FC guidelines exist and a pilot study concluded they were effective and beneficial.22,23 Patients, caregivers, and health professionals found FCs useful.24,25 In cancer care, expert opinion values the SP14,28 and supports FCs ability to provide accurate medical information.26–28
FCs are time consuming and expensive because of the personnel involved and the significant opportunity costs. We did this study because of the paucity of evidence about FCs in palliative medicine in general and cancer in particular. The primary aim was to determine whether the specific information needs of the SP were met by a subsequent FC. We also examined whether FCs impacted SP distress because of the high prevalence of caregiver distress in this population.
Methods
We report a study of 78 FCs in which a preidentified family SP completed Distress Thermometers and written questionnaires immediately before and after the FC. Further data were collected on attendee characteristics, influence on SP distress, and SP value assessment. A formal FC was defined as a scheduled meeting attended by at least one family member (to include the SP), the patient (when they wished or could participate), and two clinical specialists (MD and MSW). Teleconferences were arranged if the SP and/or family members lived far apart. Palliative medicine clinical fellows or an occasional attending physician chaired most FCs. From our established FC clinical guidelines, 13 protocol questions were developed by the Palliative Medicine Interdisciplinary Research Group. A pilot study (N = 5) first tested the clarity of the draft questionnaire.
Pilot study
A 19-item draft questionnaire was piloted by one research fellow (RF), with 6 SPs, before the study. This examined study procedures. Some questions were changed to meet the minimum USA literacy standard for 13-year-olds. Some SPs needed clarification about specific terms, for example, “Resuscitation Status” and “Durable Power of Attorney for Healthcare.” Other draft protocol terms required explanation, (e.g., code status). Most pilot participants were noted to be anxious about the words “hospice” and “resuscitation.” This guided a subsequent decision to be physically present with the SP during the survey. We also reworded some questions for clarity based on a separate informal review with one family of two parents and two teenage children.
Study design
We studied the family SP (for eligible cancer patients) perspective in consecutive first time palliative medicine FCs in an observational prospective design. The routine FC process was unchanged for the duration of the study. Clinical staff conducted the FC per usual clinical practice. The SPs were unaware of our FC protocol.
Study procedure
The study was approved by the Cleveland Clinic Institutional Review Board (IRB). Study eligibility screening was during the daily (Monday–Friday 8 am) routine clinical Interdisciplinary Team Meetings. 9 Three RFs conducted the study and met with the SP before and after the FC. The attending physician of record introduced the study to the patient. The patient approved the SP by providing verbal consent to the attending physician and then to the RF. Demographic data were collected from the electronic medical record and eligibility was evaluated.
Inclusion criteria:
>18 years of age Cancer diagnosis First scheduled palliative medicine FC Established patient-identified SP (or durable power of attorney [DPOA])
If patients did not have decision-making capacity at enrollment, consent was sought from their DPOA. If there was no DPOA, the next of kin (according to State of Ohio informed consent law) was approached 29 but this did not arise. The patient (or DPOA) was excluded if unable or unwilling to provide consent or if no SP was identified. Impromptu, informal, or unscheduled FCs were excluded. Patients/SPs were withdrawn if the patient died before the FC (or transferred to another clinical service). Exclusion criteria, patient withdrawals, and deaths were recorded (Fig. 1). The patient was given an IRB—required brief information letter. The patient-designated SP was approached separately by an RF to explain the study. This usually took 1–2 days. Patient and SP data recorded included patient relationship, knowledge of cancer diagnosis, and reason for FC. The participant numbers reported included only the patient, SP, and attendees. Physician, social worker, and researcher numbers were excluded.

Family conference eligibility and data collection.
The SP Distress Thermometers and questionnaires took about 40 minutes to complete. The distress thermometer (DT) was done first and adapted with permission from the National Comprehensive Cancer Network Distress Guidelines. 30 It is an 11-point (0 = no distress; 10 = severe distress) validated screening instrument for family members. 31 A score ≥4 indicates distress. The SP rated their distress level “right now” (immediately before and after the FC).
The 19-item pre-FC (Appendix 1) and 20-item post-FC (Appendix 2) questionnaires were administered immediately before and after the FC. The RF administered these verbally on the scheduled FC day. Twenty-four hours were allowed for the latter. The individual questions in the pre-and post-FC questionnaires were scored and compared.
The same RF administered both assessments (but was not present during the FC). The results were not shared with the clinical team before or after the FC or during the study. One extra SP question (Q19) inquired about the FC value (yes/no) pre- and post- FC. Another (Q20) requested SP comments post-FC. These were both open-ended questions and verbatim responses were recorded. Attendees and their patient relationships were noted. The MD recorded FC duration (minutes) and the items discussed. All SPs were contacted the next day by the MSW for follow-up per usual practice.
Statistical analysis
One hundred four patients were screened to obtain a data set of 78 consecutive FCs for analysis. Data were downloaded into Research Electronic Data Capture (REDCap; Vanderbilt University, Nashville, TN). REDCap is a secure, web-based application designed to support research studies. 32 We used all available data in analysis. All data for eligible patients were typed into a Microsoft Excel (2003, Microsoft, Redmond, WA) spreadsheet and analyzed with SAS® software 9.2 (SAS Institute Inc., Cary, NC). A paired samples t-test compared the DT scores pre- and post-FC. The paired t-test also examined whether the DT scores differed by patient attendance. All tests were two-sided; p < 0.05 indicated statistical significance. Qualitative analysis of Questions 19 and 20 verbatim responses were completed. These were reviewed and discussed for consensus and themes identified.
Results
Participation and completion
All consecutive eligible FCs in a five-month period were included. One hundred four scheduled FCs were screened. Seventy-eight were eligible. Twenty-six of the 104 (25%) were excluded (Fig. 1). The most frequent reason (N = 10) was that clinical or research personnel were unavailable. Five declined to participate (two patients; three SPs); four of these were African-American. Seventy-four FCs had complete data.
Seventy-eighty patients were enrolled (Table 1). English was the primary language in all except one. The ethnic composition (N = 23; 29% African American) reflected that of the City of Cleveland. 22 (28%) had a full code resuscitation status at the time of the FC. Educational level (N = 74) was a median of 12 (range 3–18) years. 98% of the patients knew their main illness was cancer, but 13 (17%) did not understand the specific diagnosis. In 8 (10%) it was not recorded. Most (N = 57; 73%) knew that the reason for the FC was to discuss their illness and discharge plan. The SP (Table 2) came from three major relationship groups: partners/spouses (N = 36), daughters/sons (N = 25), and siblings (N = 9).
Two nieces, one cousin, one grandchild, one nephew.
FC characteristics
Seventy-eight FCs had a total of 348 attendees (Fig. 2); median (range) = 4 (1–12). Daughters/sons (N = 105) were the largest single attendee group. The median FC duration was 45 minutes (range 30–100). The location was at the bedside with the patient present in 47/78 (60%). The rest were held in a dedicated meeting room. Thirteen attendees (one SP) participated by teleconference (17% of FC).
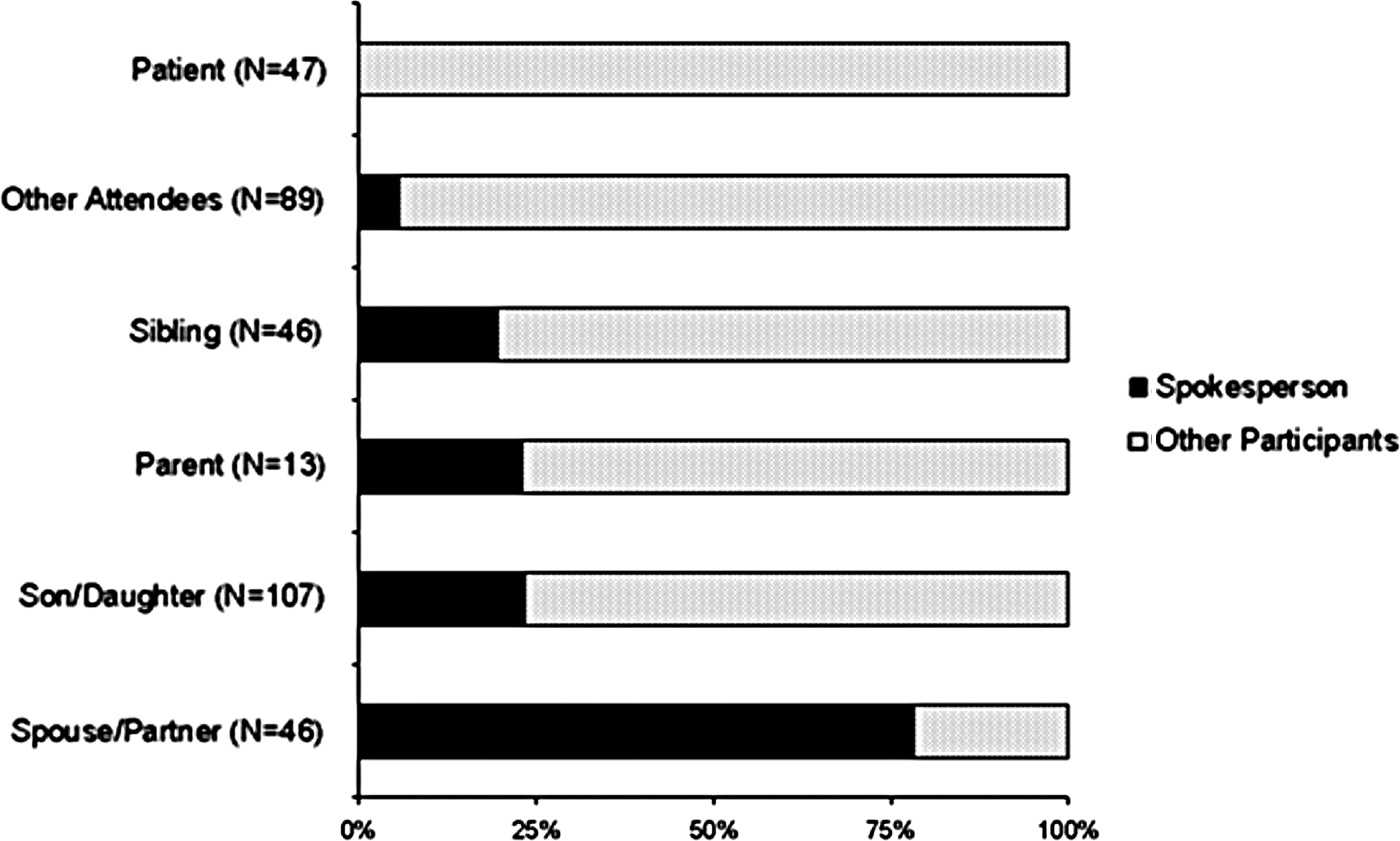
Family conference spokespersons and attendees (n = 348).
Distress thermometer scores
Overall (N = 74), DT scores fell in 38 (51%), rose in 19 (26%), and were stable in 17 (23%). There was a statistically significant one-unit reduction in DT scores afterward (p = 0.0059, 95% CI −1.5 to −0.3). 38 (51%) had scores <4 post-FC. Pre-FC (N = 74) severe distress was prevalent; 10 DT = 10 and 22 scored ≥8. In 13 of that 22 (59%), the score fell post-FC. 11 of 74 (15%) were still distressed (DT ≥4) afterward. In a minority (8/74), DT increased >2 points.
The median DT score (N = 74) fell from six (range 0–10) to three (range 0–10) and the median decrease was two (range 0–8). The son/daughter group had the greatest median decrease = −2 (range −3.2 to 1). Categorical analysis (N = 74) of median DT changes ≥2 showed 34 (46%) were stable, 29 (39%) decreased, and 11 (15%) increased. Patient presence (N = 43 of 74) made no difference: 25 (58%) decreased, 11 (26%) were unchanged, and 7 (16%) increased. If the patient was absent, the DT dropped by 1 unit (mean change −1.0, 95% CI −2 to 0.04). When the patient was present, the DT dropped by <1 unit (mean change −0.9, 95% CI −1.7 to −0.01). The difference was not significant (difference in means −0.1, 95% CI −1.4 to 1.2, p = 0.88).
Mean DT scores pre-FC = 5.5 (SD 3.2) and post-FC = 4.5 (SD 3.3) (Table 3). The mean (SD) decrease = 0.8 (SD 2.8). The mean decreased in all SP groups. Those with the most frequent decreases overall were (in descending order) relatives 4/5, parents 2/3, sons/daughters 14/23 (61%), siblings 5/10 (50%), and spouse/partner 12/33 (36%). Increases were most often 13/33 (40%) in spouses/partners; they had the most volatile rank order score changes of all SP groups. Their scores were most likely to increase and least likely to decrease. Stable scores were evenly distributed between the different SP groups.
Change is reported in mean (SD).
FC, family conference; DT, distress thermometer; SP, spokesperson.
SP questionnaires
The SP wanted information on a median of 15 (range 13–17; 83%) questionnaire items beforehand; 12 (range 10, 14; 67%) were discussed (Fig. 3). The most frequent items were (in descending order) diagnosis, prognosis, expected complications, team role, discharge plan, and hospice. Overall, 62% of the total questions were “needs met” in ≥50% of the SPs. Of the total 18 individual questions, 10 were “needs met” in >75%; 4 50–75%, and 4 < 50%. The last 4 were <50%; in descending order of “needs met” they were:
Living Will DPOA Rule Resuscitation Status SP Role
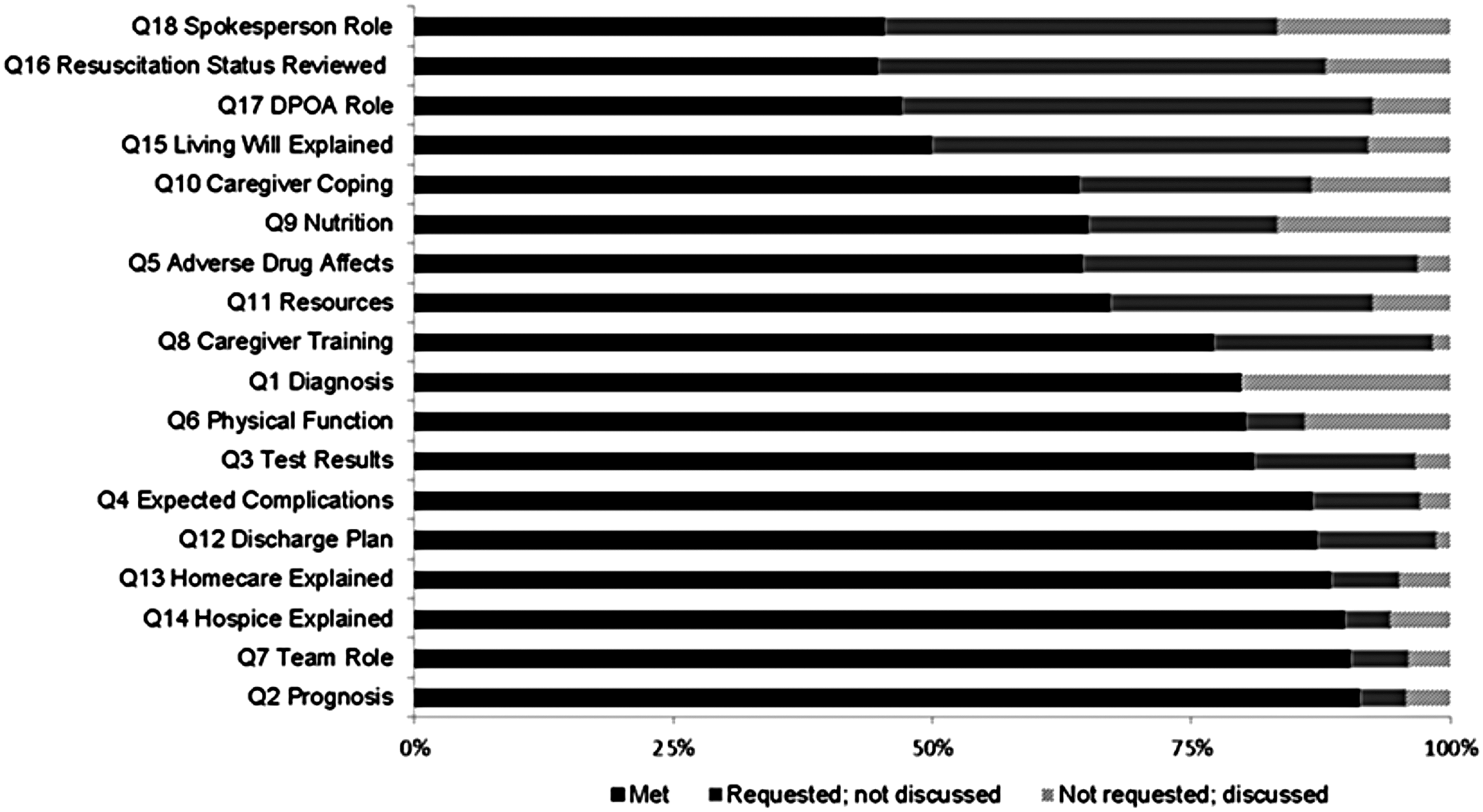
Spokespersons information needs met and unmet (questions 1–18).
FC value and feedback
The SP positive response rate to question 19 (“Was FC of value?”) was 77/78. There were 51 verbatim responses to question 20. The comments were 29 (57%) positive, 17 (33%) neutral, and 5 (10%) negative. Positive examples included the following: (1) “everyone in family knows now”; (2) “FC should be mandatory”; and (3) “covered everything, explained everything.” Three main themes emerged from the qualitative analysis of these responses. The SP was
Specific about their information needs Aware of the potential positive and negative emotional toll of the FC Intuitive regarding the potential (pre-FC) and actual (post-FC) benefits, particularly clarity about the plan of care
A common positive informal observation (during or after the FC) was “nobody has ever talked to us like this before.”
Discussion
All the SPs except one found the FC valuable. It is noteworthy that beforehand when FCs were a concept, they were also viewed positively. Distress was moderate pre-FC and decreased post-FC (except for spouses). In a significant minority, distress increased or was unchanged. High levels of distress were evident pre-SP. The SP identified pre-FC information needs in about 15 areas. Most needs were met and the SP and MD agreed about the information.
Overall, FCs appeared to be an effective communication tool. Items less satisfactorily explored (in the view of the SP) were usually accomplished earlier in the hospital stay. This was due to perceived clinical urgency, for example, resuscitation status. Revisiting and reinforcing such items was important to the SP irrespective of prior communication. Repetition of key messages is therefore important (particularly in large, geographically scattered or dysfunctional family groups).
Other studies that support the value of the FC include two smaller studies of similar structure.23,25 In the first, 23 care needs were met and the FC was judged valuable. In the second, 25 the FC reduced caregiver concerns and increased confidence. In a retrospective review, 20 of note was high patient participation but less candid discussion when the patient was present. In 140 consecutive formal FCs in a cancer center inpatient palliative medicine unit, a prospective study by the same group 21 reported high emotional distress in patients and family members. Primary caregivers were most often female spouses. Patients attended in 50%. Data were only collected post-FC. None used a SP. Using a formal SP is important14,28 and essential 10 in our model (particularly given the prevalence of patient delirium).
In our experience, informal and unplanned FCs have the potential to do harm. Successful meetings require thoughtful preparation and appropriate structure. 33 A badly organized FC might be worse than no FC.34–36 The clinical team must respect nonpathological denial and other common family dynamics.34,35 Professional follow-up by the MSW is important. This should include a written record of what transpired and the outcomes. The distinctive characteristic of the FC in our settings was that they were routine, formal, and multidisciplinary.
All the FCs reported were chaired by an MD trained in FC conduct. The time commitment is considerable (and did not include preparation and follow-up). This must be set against the varied and unpredictable consequences of ineffective communication. We believe that all physicians should get formal FC training. Specialist training 36 of all clinical staff minimizes psychological and physical risks in emotional encounters. The presence of at least two professional disciplines is important.
The study had several limitations. FCs often involve bad news and are inherently stressful. It is possible that the physical presence of the researchers before the FC and/or the study measures affected SP distress. The research was conducted in as natural a setting as possible but the study may have affected the behavior of clinical staff during the FC. We did not evaluate what the long-term impact on distress or other outcomes were. FCs might also be more effective if conducted by more experienced attending physicians. Significant methodological challenges in an acute care setting were evident. Further longitudinal and randomized studies seem important. Outcomes should include resource utilization, opportunity costs, and bereavement outcomes. The process might be improved by a pre-FC needs assessment similar to the one used in this and another 25 study (as FC guidance).
Conclusions
The FC attracted multiple participants; usually sons and daughters. Duration was 45 minutes and usually done at the bedside. SPs found the concept valuable both before and after the FC based both on direct questions and verbatim feedback. There were higher levels of SP distress in patients' spouses and siblings. Distress decreased or remained stable in most SPs and was unaffected by patient presence. On average, there was a one-unit reduction in DT scores after the FC. Qualitative analysis of SP verbatim responses revealed three positive themes around information needs, the emotional impact of the FC and the benefits of the FC structure in communicating the plan of care. Most SP information needs were met and their presence (and role) is we believe an important determinant of success. Some information requests needed more attention (even if explored in prior clinical encounters). Formal FCs are powerful and important communication tools in advanced cancer. They should be routine practice but require specialized training in their conduct.
Footnotes
Acknowledgments
Our thanks to Drs. A. Alvarez, A. Aziem, M. Khan, S. Parminder, and T. Gutgsell who chaired the conferences. Dr. D. Khoshknabi-Seyidova helped with the pilot evaluation. Drs. M. Davis, S. LeGrand, R. Lagman, and A. Parala-Metz helped recruit patients. The Palliative Medicine Social Worker was Amy Bauer, MSW, Matt Karafa, PhD, helped with data management. Barb Hullihen, BS, assisted with study management. Ellen Schleckman, Aditya Nair, and Nikhil Makkar helped with data entry and qualitative analysis of the data.
The Harry R. Horvitz Center for Palliative Medicine is a World Health Organization Demonstration Project in Palliative Medicine and is an ESMO Designated Integrated Center of Supportive Oncology and Palliative Care. This study was presented in part at the seventh European Association for Palliative Care Research Congress, June 7–9, 2012, Trondheim, Norway.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1. Pre-FC Spokesperson Questionnaire
Assigned Study Number: W___P___
Directions to the Presurvey: This survey is to assess what information is important for you to have explained in the family conference today. For example I am going to ask you if you need Mr/Ms _____ medical condition explained to you today. And you will have the following options to answer the question: Yes/No/Do Not Know/Not Apply
Appendix 2. Post-FC Questionnaire for Physician/Physician Asisstant or Social Worker
Assigned Study Number: W___P___
Directions to the Postsurvey: This survey is to assess what information needs were addressed by the physician and social worker in the Family Conference.
Length of FC: _______________
You will have the following options to answer the question:
Yes/No/Do Not Know/Not Apply