
Abstract
Abstract
Background:
International Association for Hospice and Palliative Care implemented Opioid Price Watch (OPW) to monitor availability, dispensing prices and affordability of opioids. We found that opioids with complex delivery mechanisms [fentanyl transdermal (TD) patches, sustained-release (SR) morphine, and SR oxycodone] had lower dispensing prices than immediate-release (IR) morphine formulations.
Objective:
Identify the extent that SR and TD formulations are dispensed at lower prices than generic IR morphine and the possible reasons to explain this observation.
Design:
Using OPW data for 30-day treatment Defined Daily Dosages, we identified where SR and TD formulations are dispensed at lower prices than IR morphine. Then we analyzed national lists of essential medicines (EML) in middle- and low-income countries to answer two questions: (1) Do they have opioids included? If yes, (2) Which ones? We then sought information on selection, budget allocation, and procurement for EML. OPW participants confirmed/verified the EML information.
Results:
Eighteen countries reported higher dispensing prices for IR morphine (oral and/or injectable) than TD or SR formulation. Injectable morphine was highest in seven and lowest in two (range: $74–$742). SR morphine was the least expensive, while TD fentanyl was second. Median dispensing price for IR oral morphine was higher than SR morphine. The EML for 10 countries include opioids in TD and/or SR formulations.
Conclusions:
Opioids in expensive formulations are being favored over IR morphine both at the dispensing level and in their inclusion in national EML. Governments must take decisions based on efficacy, safety, and cost-effectiveness of medications.
Background
A
WHO revises and updates its EML every two years by analyzing the evidence for the addition and deletion of medications in the list. In 2013, the WHO added a new section in the WHO EML called Medicines for Pain and Palliative Care and included morphine (in all its formulations) and oxycodone (as a substitute to morphine) for pain treatment. 4 Recently, two medications were added for the treatment of cancer pain: fentanyl transdermal (TD) patch and methadone (tablet, oral, and concentrate). 5
Given that opioids are internationally controlled medications under the Single Convention of Narcotic Drugs (hereon referred to as “Single Convention”), 6 to procure the opioid medications, the corresponding national authorities must buy from internationally licensed and authorized vendor(s). The tendering, procurement, licensing, and exchange of goods at the international level is monitored and controlled by the International Narcotics Control Board (INCB), as part of its mandate in the Single Convention. Controlled medicines are sold in the international market by wholesalers and proprietors of medications (i.e., Pharmaceutical companies), and not for profit entities (for cases of humanitarian emergencies in countries with limited resources). Countries can buy raw material for compounded preparations or for local manufacturing, and/or buy finished products, including branded and generic ones.
In 2014, the World Health Assembly unanimously adopted a Palliative Care Resolution, which urges governments to take the steps needed to ensure access to PC services to patients in need, including safe and effective access to medicines for the treatment of pain and palliative care. 7 However, the vast majority of patients with legitimate medical needs do not have adequate access to opioids for pain relief and other symptoms.8,9
Access to opioids is limited due to several reasons, including restrictive drug control laws and regulations, limited education of health professionals, and high prices.10,11 The use of opioid medications in low- and middle-income countries is particularly and significantly affected by cost.12,13 In previous studies, the dispensing price of opioids in low- and middle-income countries have been reported to be higher than in high-income countries. as well as higher in smaller towns and rural areas than in large urban areas. 14
In 2012, the International Association for Hospice and Palliative Care (IAHPC) developed and implemented a project called Opioid Price Watch (OPW) to collect, report, and monitor the availability, dispensing prices, and affordability of 5 opioids (fentanyl, hydromorphone, methadone, morphine, and oxycodone) in 13 formulations. The OPW project is a component of the agreement between IAHPC and WHO as an NGO in formal relations with WHO.
In the OPW study, participants were asked to provide the lowest dispensing price of the smallest selling unit and lowest strength of five opioids in 13 formulations from a licensed pharmacy located closest to a public facility that provides diagnosis/treatment for life-threatening conditions.
The price for a 30-day treatment was calculated in three steps: first, the price per milligram (mg) was calculated by dividing the dispensing price of the package/bottle by the total mg in each. Second, the resulting price per mg was multiplied by the corresponding defined daily dose (DDD) 15 for the daily price. Finally, the resulting price per milligram per day was then multiplied by 30. Table 1 includes the DDD for each medication.
DDD, defined daily dose.
The results from the first phase of OPW indicated that patients living in countries in lower economic groups had to pay higher prices for opioids than those living in high-income countries. 16 Findings also indicated that regarding its international reference price, the median price of 10 mg of morphine oral solid immediate release (IR) was 5.8 times higher in low- and middle-income countries than in high-income countries. 17
In 2016, the IAHPC developed and implemented a second round of OPW. Results from this round were consistent with the results of the first and indicate that the availability of opioids at the pharmacy level is directly correlated to the country's Gross National Income and the human development index. 18
For both reports of OPW studies, we found unexpected favorable differences in the dispensing price of opioids with complex delivery mechanisms compared to IR oral and injectable morphine. In many instances, we found that fentanyl TD patches, sustained-release (SR) oral morphine, and SR oral oxycodone were dispensed at lower prices than IR morphine.
This is the third report of OPW. The purpose of this study was to identify the extent to which SR and TD formulations are dispensed at a lower price than generic IR morphine, and the possible reasons to explain this observation.
Methods
We designed and implemented a cross-sectional study during the months of February to June 2017, which included four steps:
Prices
Using the data collected and the results from both phases of the OPW, we identified the locations and the countries where the reported dispensing price of IR oral and/or injectable morphine was higher than at least one of the other opioids with complex delivery formulations (TD and SR) included in the study:
− Fentanyl [transdermal (TD) patches] − Hydromorphone [oral solid, SR] − Morphine [oral solid, SR] − Oxycodone (oral solid SR)
In this study, we included only those locations in which we observed higher dispensing price of IR morphine (oral and/or injectable).
Essential medicines
In a second step, from the list of 18 countries where we observed higher dispensing price of IR morphine (oral and/or injectable), we identified 12 that were classified either as middle (upper and low) or low, based on their income levels as per the World Bank. 19 One of the coauthors (N.A.) conducted an initial literature review and a search in the websites of the Ministries of Health, the WHO website, and the WHO Regional Offices websites and obtained copies of their national lists of essential medicines, either by downloading them directly from the Ministry of Health website or by requesting a copy from the Ministry of Health office. The lists of essential medicines were analyzed by two coauthors (N.A. and L.D.L.) to answer two questions: (1) Do they have opioids included? If yes, (2) Which ones? Those which had opioids with complex delivery mechanisms (SR and TD) were included in this second analysis.
Procurement process
In a third step, we tried to find information related to the budget allocation for essential medicines (in particular for opioids), any information on the process leading to the identification and selection of medications subsidized by the government programs, and any information on the procurement and tendering process for medicines in the public sector.
Confirmation of information
In a final step, we contacted through e-mail the participants of the previous two OPW studies and invited them to participate as collaborators. Individuals who accepted, received a letter that they could use to contact the corresponding office in the Ministry of Health or Drug/Medicines Administration Authority to inquire on the questions described in Step B above. We also asked them to request the relevant national authority permission to share their contact information with us, so that we could follow up with a direct e-mail or phone call. Participants were offered three months of free membership with IAHPC in exchange for their collaboration.
This study was approved by an ethics review board from the Fundación Federación Médica de Buenos Aires, in Argentina.
Data analysis
Survey results were exported to Microsoft Excel and analyzed using IBM SPSS Statistics. Descriptive analysis and bivariate analysis were conducted using nonparametric analysis as median and interquartile range and Kruskal–Wallis test for comparing groups.
Results
Prices
Eighteen countries reported higher dispensing price of IR oral and/or injectable morphine than at least one of the other opioids with complex delivery formulations (TD and SR). Table 2 includes the list of countries and their income category as per the World Bank. Four countries had multiple reports from different locations (India, Kenya, Mexico, and Poland) for a total of 25 reports. The Supplementary Table S1 (Supplementary Data available online at www.libertpub.com/jpm) includes all the prices reported from all the 25 locations.
d one for children (14 years old>). Information contained on this table considered both lists.
IR, immediate release; N, no; NA, medication not available at the time of the survey; SR, sustained release; Y, yes.
Injectable morphine was the highest priced medication in seven countries (Germany, Hungary, Kenya, Mexico, Nepal, Poland, and Rwanda), and the lowest one in two (Costa Rica and Togo). The range in the dispensing price of morphine injectable for 30 days of DDD was $74–$742 (Costa Rica and Mexico, respectively).
SR oral morphine was the most frequently favorably priced at the dispensing level. In 10 countries (Costa Rica, Germany, Guatemala, India, Ireland, Nepal, Norway, Panama, Rwanda, and Togo) SR oral morphine was less expensive than IR oral morphine (either solid tablet and/or solution). In 16 countries, SR oral morphine was less expensive than injectable morphine (El Salvador, Germany, Guatemala, Hungary, India, Ireland, Kenya, Lebanon, Mexico, Nepal, Norway, Panama, Poland, Rwanda, Sweden, and United Kingdom).
TD fentanyl was the second most frequently favorably priced at the dispensing level. In six countries (El Salvador, Germany, Hungary, India, Panama, and Poland), it was priced the lowest among the opioids available in the pharmacy the day the study was conducted. In additional 10 locations in 7 countries (Guatemala, Ireland, Kenya, Mexico, Norway, Poland, and Sweden), TD fentanyl was dispensed at a lower price than morphine IR solid or liquid and/or morphine injectable.
In a comparative analysis between prices and the countries' income groups, the highest prices were observed in countries in the upper middle-income level, followed by countries in low-income level (Table 3). We also compared the dispensing prices of the different opioid medications to IR oral morphine tablet and displayed in a box plot (Fig. 1). In this analysis, 1 means that the price of the other opioid formulation is the same as the price of IR oral morphine tab, >1 is less expensive, and <1 is more expensive. We found that the median dispensing price for IR oral morphine was higher than the price for SR oral morphine (Fig. 1). SR hydromorphone was available only in high-income countries, so we were unable to do comparisons with countries in other income levels.
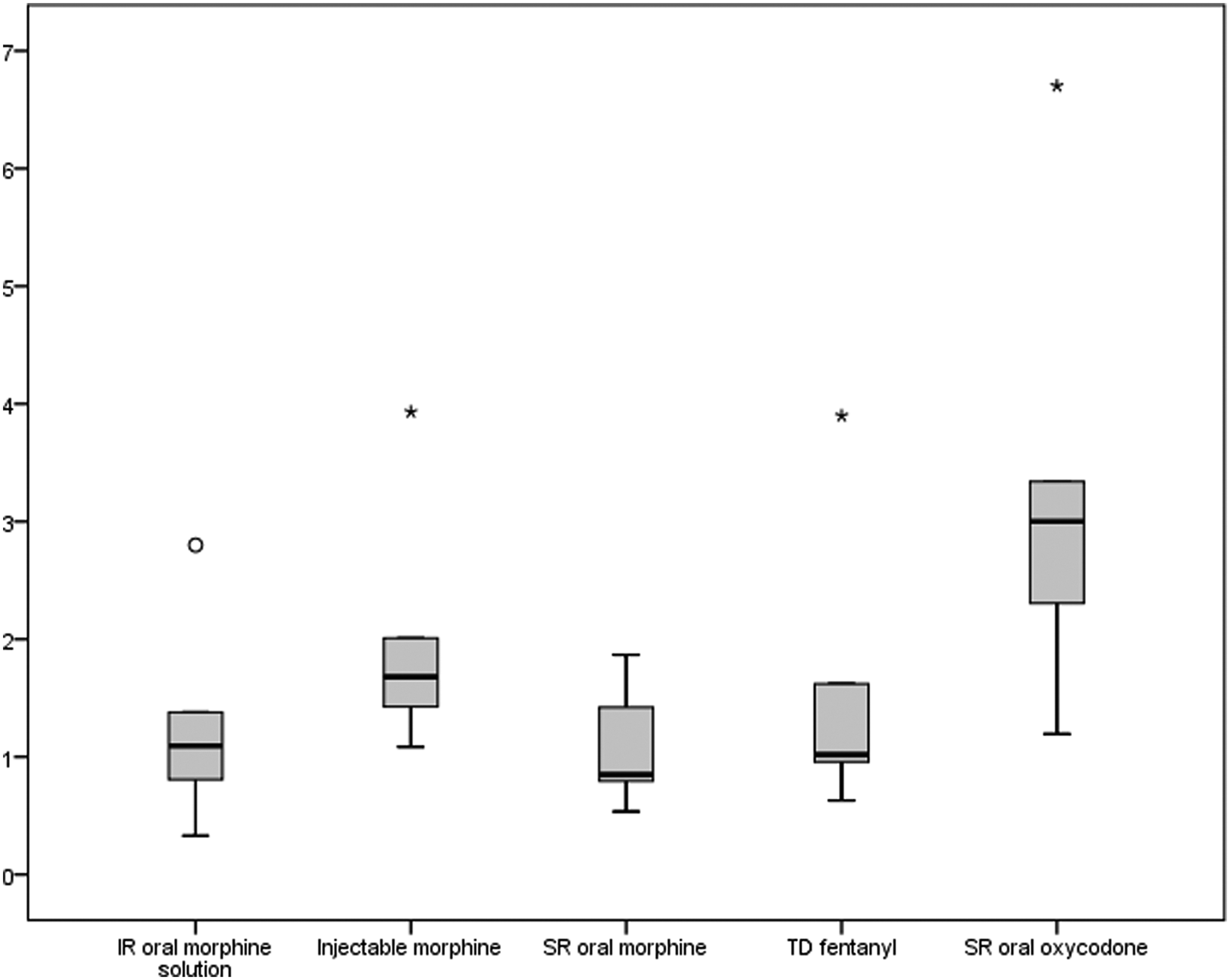
Box plot of the dispensing price of selected opioids compared to the price of IR oral morphine (gold standard). IR, immediate release. (oatypical values; *extreme values.)
(4 years old>). Information contained on this table considered both lists.
TDP, transdermal patch; NA, not available.
Lists of essential medicines
From the 18 countries in Step A, 12 countries were identified either as middle income or low income and we located their national lists of Essential Medicines: [Costa Rica, 20 El Salvador, 21 Guatemala, 22 India, 23 Kenya, 24 Lebanon, 25 Mexico, 26 Nepal, 27 Panama, 28 Poland, 29 Rwanda, 30 and Togo31,32].
After an initial review, we found that opioids with complex delivery mechanism (SR and TD) are not included in the lists of essential medicines of Poland and Rwanda, and thus were excluded from this step.
Table 4 shows the list of 10 countries (Costa Rica, El Salvador, Guatemala, India, Kenya, Lebanon, Mexico, Nepal, Panama, and Togo) that have opioids with TD and SR formulations included in their national lists of essential medicines. Nine countries include at least one formulation of IR morphine (oral and/or injectable). In Lebanon, morphine IR injectable is included in the EML for anesthesia and includes an SR oral morphine tablet in formulations “from 10 mg to 100 mg,” but does not specify which formulations in this range are essential. Togo has two essential medicines lists, one for adults and one for children (<14 years old).
PAHO: Pan American Health Organization (WHO regional office for the Americas).
In Lebanon, morphine IR injectable is included in the EML for anesthesia.
In Lebanon, the EML includes an SR oral morphine tablet in formulations “from 10 mg to 100 mg.” The EML does not specify which formulation(s) in this range is (are) essential.
In Mexico, the list of EM (“Cuadro Básico”) distinguishes between medications needed for the first level and medications needed for second and third levels. Opioids are included in the second and third levels only.
Togo has two EM lists, one for adults and one for children (14 years old>). Information contained on this table considered both lists.
WHO, World Health Organization.
The EML for Mexico is developed by the National Health Council (Consejo de Salubridad Nacional), a national health body representing the major health institutions and the Ministry of Health. The EML (“Cuadro Básico”) distinguishes between medications needed for the first level and medications needed for second and third levels. Opioids are included for use in the second and third levels only. The EML for Mexico had the most number of opioid in SR and TD formulations (SR morphine, SR oxycodone, SR tapentadol, and TD fentanyl patches).
The oldest essential medicines list is from Togo (2012) and the most current ones are from El Salvador, Kenya, Nepal, and Mexico (2016), and Panama (2017).
Procurement process
Despite different attempts and efforts to find information regarding budget allocation for essential medicines (in particular for opioids), and information on how the procurement process for medicines is financed in the public sector, we were not successful. We were also unsuccessful in our effort to contact directly the corresponding Ministry of Health representative who could provide this information.
Confirmation process
Eleven participants in previous OPW responded and verified/confirmed the country information with their corresponding Ministry of Health. They also confirmed their voluntary participation. Participants are listed in the Acknowledgments section.
Discussion
Prices
The analysis of prices was based on the results of previous findings of the OPW. All the OPW reports were from large or medium urban centers. This is not surprising given that the prices we requested were for pharmacies close to or inside a health facility that provides diagnostic and treatment services for patients with life-threatening conditions such as HIV and cancer, and that these major treatment centers are usually located in large urban areas.
Our previous OPW studies and this one as well, indicate that despite having a lower price in the international market, generic IR oral morphine tends to be dispensed at a higher price than formulations that are more expensive, in particular SR oral morphine and TD fentanyl patch.
Injectable morphine was one of the highest priced medications and we are unable to determine the reason behind such a large overhead between the reported purchase price and the selling price. Ampoules contain generic morphine and thus should not be priced at such high levels.
Results also show that for six formulations, countries in the upper middle-income category had the highest prices for a 30-day treatment among the gross national income groups. Sadly, in many of these countries, the ability to negotiate lower prices at the international level and the funding pool to share healthcare expenditures is still inadequate or not available, and thus these higher costs are transferred to the patients who must pay out of pocket.
The fact that this study and the previous OPW studies have shown favorable pricing for medications that are more expensive in the international suppliers' market indicates that there is little interest and limited political will to improve availability and access to IR generic morphine, both in oral and injectable formulations. We are unable to identify the reasons behind this, which is common across several countries in all income levels. Options could be that the countries in lower income levels may have less negotiating power when buying in the international markets, lack of knowledge about less expensive vendors of morphine tablets in the international market, and/or may fall under the influence of groups and individuals who have a vested interest in more expensive opioids over IR generic morphine. A recent report published by a Lancet Commission on Global Access to Palliative Care and Pain Relief stresses the importance of improving access to generic morphine in both injectable and oral formulations, particularly in countries with less resources. 33 Governments that have not done so should include IR generic morphine formulations in their national health programs to maximize the use of resources in the procurement of medicines.
Lists of essential medicines
The WHO updates its model list of essential medicines every two years and the decisions are taken by a committee of experts, based on analysis of scientific evidence and cost effectiveness through an open transparent process. The inclusion of medications in a national EML should also fulfill the criteria of efficacy, safety, and cost-effectiveness, and indicate the political will to ensure their availability and affordability of such medicines, especially to those living under the poverty line.
Of the list of 12 countries included in the essential medicines analysis, the lists of El Salvador Guatemala and Panama were the first editions. Two countries (Poland and Rwanda) did not include expensive formulations in their list of essential medicines, thus ensuring that government funds are used to buy the least expensive medications and formulations, leading to greater cost-effectiveness. All countries include at least one formulation of IR morphine (oral and/or injectable). Nepal and El Salvador had a very detailed description of the methodology as well as the names of those who took part in the process to revise and update the list of essential medicines. The essential medicines lists for Guatemala and Lebanon state that the selection is based on evidence and prepared by a committee of five experts (names provided). The Ministry of Health publication of Panama and Rwanda described the process for the selection of the medicines in the national essential medicines, stating that the input from the relevant stakeholders and the opinion of specialists were taken into consideration, but no names were given.
In Mexico, a National Health Council composed of representative of the major health institutes and the Ministry of Health determines the overall EML for the whole country. In turn, each institution has the autonomy to define its own list according to the population they serve and their needs. The EML of the institutions can include less, but not more or beyond those approved by the National Health Council. So, in some institutions, the EML may differ from another, including opioids. For the purpose of this study, we analyzed the overall EML approved by the National Health Council, which includes SR morphine, SR oxycodone, SR tapentadol, and TD fentanyl patches. 31
None of the contact persons in the countries we worked with had taken part or was invited to provide guidance and feedback on the medicines for palliative care, despite being leaders in the field. Governments should update their national lists of essential medicines periodically, taking into consideration their current epidemiological changes and health needs, and consider the opinion of experts for the relevant sections in their lists of essential medicines. As in the WHO Model List, the addition or deletion of medications to the proposed essential medicines list in a country should be based on scientific evidence and following a transparent process, to ensure that the population is offered the medications proven to be most safe, efficacious, and cost-effective in the market.
Procurement process
We were unable to find any information on how funding is allocated for the procurement and tendering of medicines for the countries included in this study. Countries in lower income levels have very limited resources to subsidize the needed medications to patients with no significant income. Hence, the decisions as to which medications are subsidized and included in the national essential medicines lists should be based on evidence on efficacy, safety, and affordability, and unless unavoidable, not favor commercial, patented products over nonproprietary products with proven equal or better characteristics.
Additional research needs to be developed to identify the reasons behind some of the differences in prices among the medications, especially those in TD and SR formulations with IR generic morphine. This also includes research on the process for the selection of medications for the national lists of essential medicines.
Study limitations
The analysis of prices is based on a sample of data of a few local pharmacies, which is not representative of the prices in the whole country. However, the fact that pharmacies were located near major treating center, may suggest that other pharmacies distant from hospitals may have even higher prices.
OPW uses DDD for its analysis, which may not be completely aligned with clinical practice, so the ability to conclude adequate clinical care is limited. DDD is a statistical tool and not a measure of adequate dosing.
The information we found on the lists of essential medicines in the countries was retrieved from the corresponding Ministry of Health websites and the Department of Essential Medicines at WHO, and although we tried to ensure that our analysis included the most updated versions, we were unable to confirm so with a representative from the corresponding Ministry of Health office.
Conclusion
OPW is the only global monitoring mechanism to report the dispensing price of opioids and as such serves as a unique source of information on how prices affect access. This study indicates that patented products with complex delivery mechanisms such as TD patches and sustained-release formulations are significantly being favored over generic IR morphine formulations. Government representatives need to revise the allocation of budgets for the procurement and tendering of medications at the international level and the decision process for the inclusion of expensive medications in the national lists of essential medicines. Governments in countries with limited resources, where there are less pooling mechanisms to share the burden of the cost of care, need to take decisions based on evidence and cost-effectiveness.
Footnotes
Acknowledgments
Technical support for this study was provided by Dr. Gilles Forte Team Coordinator at the WHO Department of Essential Medicines and Health Products, Health Systems and Innovation in Geneva.
Collaborators who confirmed/verified the information were (in alphabetical order by country) as follows: Andrea Medina (Costa Rica), José Mario Lopez Saca (El Salvador), Eva Rossina Duarte (Guatemala), Arunangshu Ghoshal (India), Gladys Nduku (Kenya), Hibah Osman (Lebanon), Iraima Matos (Mexico), Sunita Panta (Nepal), Rosa Buitrago (Panama), Aleksandra Kotlinska-Lemieszek (Poland), and Koffi Anoumou Tengue (Togo). This study was partially supported by a grant to the IAHPC from the Open Society Foundations (grant number OR2016-29149).
Author Disclosure Statement
The authors declare that they do not have a conflict of interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.