
Abstract
Abstract
Context:
Opioid-induced neurotoxicity (OIN) is an underdiagnosed yet distressing symptom in palliative care patients receiving opioids. However, there have been only a limited number of studies on OIN.
Objectives:
Our aim was to determine the frequency of and risk factors for OIN in patients receiving opioids during inpatient palliative care.
Methods:
We randomly selected 390 of 3014 eligible patients who had undergone palliative care consultations from January 2014 to December 2014. Delirium, drowsiness, hallucinations, myoclonus, seizures, and hyperalgesia were defined as OIN and were recorded. The other 10 common symptoms in cancer patients were assessed using the Edmonton Symptom Assessment Scale (ESAS). Patient demographics, morphine equivalent daily dose (MEDD), comorbidities, OIN management, and overall survival (OS) duration were also assessed. The associations between the incidence of OIN and MEDD, the other 10 symptoms, and OS were analyzed.
Results:
Fifty-seven (15%) patients had OIN. The most common symptom was delirium (n = 27). On multivariate analysis, a high MEDD (p = 0.020), high ESAS pain score (p = 0.043), drowsiness (p = 0.007), and a poor appetite (p = 0.014) were significantly associated with OIN. OIN was not significantly associated with a shorter OS duration (p = 0.80).
Conclusions:
OIN was seen in 15% of patients receiving opioids as part of inpatient palliative care. Although OIN was not associated with OS, routine monitoring is especially needed in cancer patients.
Introduction
Pain is a common problem in cancer patients, particularly in the advanced stages of disease. 1 Opioids are the mainstay of cancer pain management and significantly improve pain control through primarily inhibitory effects on pain transmission. Opioid analgesics act on opioid receptors, which produce an analgesic effect but are also associated with other side effects upon activation. Physicians often report a wide range of responses to opioids in their patients in terms of analgesic efficacy, adverse reactions, tolerance, need for increasing daily dose, need for adjuvant treatment, and switching to another opioid. Dose escalation for inadequate pain control is frequently associated with multiple adverse events, such as opioid-induced neurotoxicity (OIN), nausea, and constipation. 2
OIN is a commonly used term to describe neuropsychiatric symptoms that result from opioid use; these range from excessive drowsiness (sedation) to hallucinations, delirium, myoclonus, seizures, and hyperalgesia.
3
OIN can worsen patients' quality of life and negate the benefit of opioids. The mechanism of OIN is thought to be multifactorial. On a biochemical level, it is thought to involve the endocytosis of opioid receptors and stimulation of N-methyl-
Sedative effects caused by opioids may represent a continuum of effect and might slow down cognitive function in most patients. Delirium is one of the most frequent neuropsychiatric complications in patients with advanced cancer and is described as coexisting with cognitive impairment, hallucinations, and other perception abnormalities. 2 Some of the other manifestations of OIN include myoclonus (jerking of the extremities) and hyperalgesia (increased sensitivity to pain with repeated stimulation). These are easier to define than sedation and delirium.
The opioids that are more commonly associated with OIN are those opioids with active metabolites, including morphine, codeine, meperidine, oxycodone, and hydromorphone. Fentanyl and methadone do not have active metabolites, and patients are less likely to experience OIN while on these medications. 2 Prior studies suggest that patients with renal failure, who are elderly, and who have infections or dehydration have increased risk of metabolite accumulation and thus increased neurotoxicity.2,3–6
OIN has been reported in several previous studies that have not focused on patients with advanced cancer. In an observational study of 156 patients, Kullgren et al. found that hydromorphone-induced neuroexcitation symptoms developed in 6.4% (10) of hospice patients. Hyperalgesia (n = 7), myoclonus (n = 8), allodynia (n = 1), or a combination of these symptoms was noted. 7
Finally, OIN has been reported when studying a focused topic such as opioid rotation for the management of uncontrolled pain or adverse effects. De Stoutz et al., in a retrospective study of 191 patients in a palliative care unit, found that the most common reasons for opioid rotation were cognitive failure (39%), hallucinations (24%), and myoclonus (11%). 10 In another retrospective study, Reddy et al. 24 evaluated the frequency of opioid rotation among cancer patients receiving strong opioids in an ambulatory setting; 12% (13 of 114) of the patients underwent opioid rotation due to OIN.
Despite the occurrence of OIN in patients receiving treatment for pain in advanced cancer, and despite its debilitating consequences, there have been only a limited number of studies on the frequency of and risk factors for OIN in such patients in a routine clinical setting. 9 Research into this topic could provide us with a better understanding of the treatment and prevention of OIN. The purpose of this retrospective study was to determine the frequency of OIN in patients receiving opioids in the inpatient palliative care unit and to examine the association between the incidence of OIN and patients' overall survival (OS) duration.
Patients and Methods
In this study, 600 patients were selected randomly from 3014 consecutive inpatient palliative care team (PCT) consultations at The University of Texas MD Anderson Cancer Center (Houston, Texas) from January 2014 to December 2014 and were reviewed retrospectively to determine whether they met the following eligibility criteria: (1) advanced cancer, (2) ≥18 years of age, and (3) taking opioid medication for ≥24 hours. Of these 600 patients, 390 were eligible and were included. The data collection flowchart is shown in Figure 1. This study was approved by the Institutional Review Board of MD Anderson, which waived the requirement for informed patient consent.
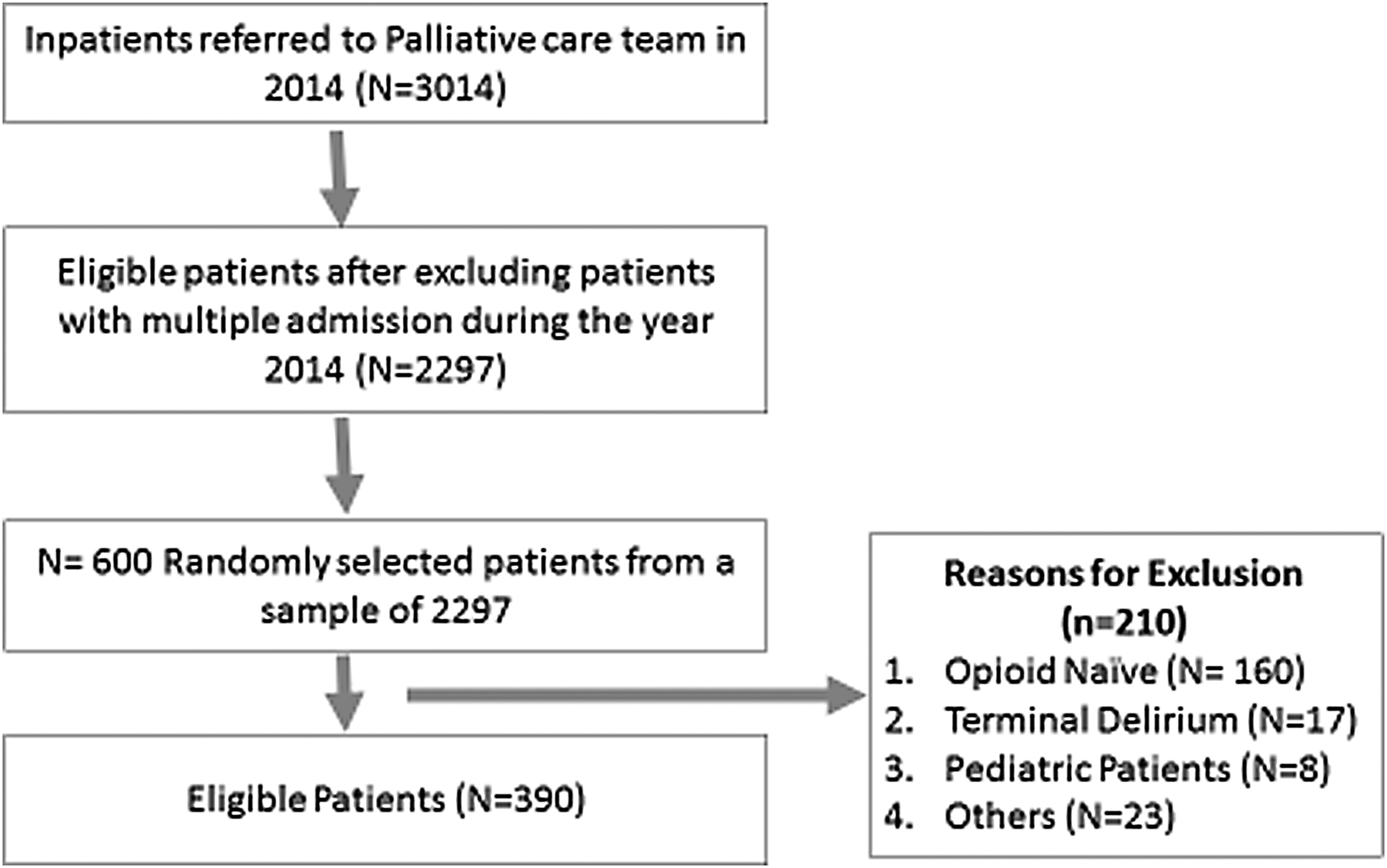
The study flow chart of data collection.
The following information was collected for each patient: demographics, Eastern Cooperative Oncology Group performance status, Edmonton Symptom Assessment Scale (ESAS) score, 10 Memorial Delirium Assessment Scale, 11 Cut-down, Annoyed, Guilty, Eye-opener (CAGE) 12 questionnaire, pain characteristics (nociceptive, neuropathic, or both), tobacco and illicit substance use, comorbidities such as renal and hepatic dysfunction, morphine equivalent daily dose (MEDD), subtype of OIN, management of OIN, and date of death or last follow-up.
Opioids included morphine, hydrocodone, hydromorphone, oxycodone, methadone, oxymorphone, and fentanyl. The MEDD was the total dose of opioids administered in 24 hours converted to an equivalent dose of oral morphine. It was calculated using the standard conversion ratios 13 ; a conversion factor of 5 was used for methadone.14,16
The Memorial Delirium Assessment Scale was used to measure the presence and severity of delirium. A score of ≥7 of 30 has been recommended as a cutoff for establishing a diagnosis of delirium. 11 The CAGE score is a four-item validated tool that is used to screen for alcoholism. The threshold varies according to sex. A score of ≥2 is considered positive for men, whereas a score of ≥1 is considered positive for women. 12
Symptoms such as drowsiness (excessive sedation), hallucinations, delirium, myoclonus, seizures, and hyperalgesia were recorded and defined as OIN in this study. A board-certified palliative care specialist (PCS) made the diagnosis of OIN.
Drowsiness was recorded if the PCS reported opioid-induced drowsiness or drowsiness that improved after the opioid was discontinued, decreased, or changed. Opioids were considered a cause of delirium if the condition improved after they were discontinued, decreased, or changed. Hallucinations were recorded if the PCS described opioid-induced hallucinations and differential diagnoses such as psychiatric disease, substance abuse, metabolic derangements, and brain neoplasms had been excluded. 8 Myoclonus was on the basis of opioid-induced myoclonus or the presence of twitching, jerking, or myoclonic movements in relation to opioid use. 18 Seizures were defined as any reported tonic clonic motor activity with loss of consciousness witnessed by PCU staff or family in a patient with no history of seizures. 16 Hyperalgesia was reported as allodynia or hyperalgesia, as described by the PCS.
The ESAS was used to assess 10 symptoms that are common in patients with cancer during the 24 hours preceding the administration of opioid: pain, fatigue, nausea, depression, anxiety, drowsiness, shortness of breath, appetite, sleep, and well-being. The severity of each symptom is rated from 0 to 10 (0 = absence of that symptom; 10 = worst possible severity of that symptom). The instrument is valid and reliable for assessing the intensity of symptoms in patients with cancer.10,15
Statistical analysis
Data were first summarized using standard descriptive statistics and contingency tables. The association between categorical variables was examined by chi-square test or Fisher's exact test. The t test was used to examine the differences in continuous variables between and among groups. Univariate logistic regression analysis was used to assess the effect of demographic and clinical factors on the presence of OIN using a univariate logistic regression model. A subsequent multivariate regression analysis was performed using variables that were noted to be significant to determine the best model for predictors. Significance levels <0.05 were considered statistically significant. Patients' OS duration was defined as the time in months from the palliative consultation to death and was estimated using the Kaplan–Meier method. Comparisons between patients with OIN and without OIN were evaluated by the log-rank test.
Results
Patient characteristics are summarized in Table 1. Their median age was 55 years. Among the 390 patients included in this analysis, 51% (197) were men, 64% (249) were white, and 64% (248) were married. Eleven percent of patients (44) had a history of drug abuse, 52% were smokers or ex-smokers, and 15% (59) had a positive CAGE score. Fifty-seven percent (223) had a performance status of ≥3. The most common primary malignancy was gastrointestinal cancer, which was found in 86 patients (22%).OIN was reported in 15% (57) of patients.
Patient Characteristics
CAGE, Cut-down, Annoyed, Guilty, Eye-opener; ESAS, Edmonton Symptom Assessment Scale.
The characteristics of patients with and without OIN are summarized in Table 2. Of 57 patients with OIN, 25 (44%) had one symptom of OIN and 32 (56%) had more than two or more symptoms. Patients with two or more symptoms had a higher MEDD than did those with one symptom (p = 0.002). The most common symptom of OIN was delirium 47% (n = 27). Drowsiness, hallucination, and myoclonus were reported in 42%, 40%, and 37% of patients, respectively. There were no cases of opioid-induced seizure or hyperalgesia in this study. The agents that caused OIN were hydromorphone (n = 16), morphine (n = 13), oxycodone (n = 11), fentanyl (n = 10), hydrocodone (n = 2), or a combination (n = 2).
Demographic and Clinical Characteristics of Patients with Opioid-Induced Neurotoxicity and Those without Opioid-Induced Neurotoxicity
GI, gastrointestinal; GU, genitourinary; GYN, gynecological; MEDD, morphine equivalent daily dose; OIN, opioid-induced neurotoxicity.
The most common management approach for OIN was opioid rotation, which was used in 40 (70%) patients, followed by opioid reduction/discontinuation, which was used in 16 (28%) patients. Other therapies for OIN were hydration (n = 5) and close monitoring (n = 2). The rotated agents were morphine (n = 16), hydromorphone (n = 11), fentanyl (n = 6), methadone (n = 4), oxycodone (n = 2), and oxycontin (n = 1) (Table 3). On univariate analysis, the factors that were significantly associated with OIN were poor performance status (p = 0.021), ESAS pain (p = 0.023), ESAS drowsiness (p = 0.012), ESAS appetite (p = 0.005), ESAS well-being (p = 0.01), and high MEDD (p = 0.003). No difference in the two groups was found with regard to age, sex, race, education, primary cancer diagnosis, drug abuse history, smoking history, CAGE, or comorbidity, such as renal or hepatic dysfunction.
OIN Pattern for Patients with Opioid-Induced Neurotoxicity
The number of OIN exceeds that of the subjects, due to patients with multiple OINs.
The results of the multivariate analysis for predictive factors of OIN are presented in Table 4. A high MEDD (odds ratio [OR] = 1.00 per mg, p = 0.020), high ESAS pain score (OR = 1.27 per point, p = 0.043), drowsiness (OR = 1.28 per point, p = 0.007), and a poor appetite (OR = 1.29 per point, p = 0.014) were significantly associated with OIN.
Multivariate Logistic Regression Analysis of Predictive Factors for Opioid-Induced Neurotoxicity
CI, confidence interval; OR, odds ratio.
The median OS duration of this study population was 2.6 months (95% confidence interval [CI]: 2.0–3.2 months). The median OS durations in patients with and without OIN were 2.2 months (95% CI: 1.2–3.2 months) and 2.7 months (95% CI: 2.0–3.3 months), respectively (Fig. 2). There was no significant difference in OS duration (p = 0.893) between patients with and without OIN. In addition, none of the OIN symptoms, such as drowsiness (p = 0.066), hallucinations (p = 0.056), myoclonus (p = 0.409), or delirium (p = 0.555), was associated with OS duration. There was also no significant difference in OS duration by the number of OIN symptoms (p = 0.870).
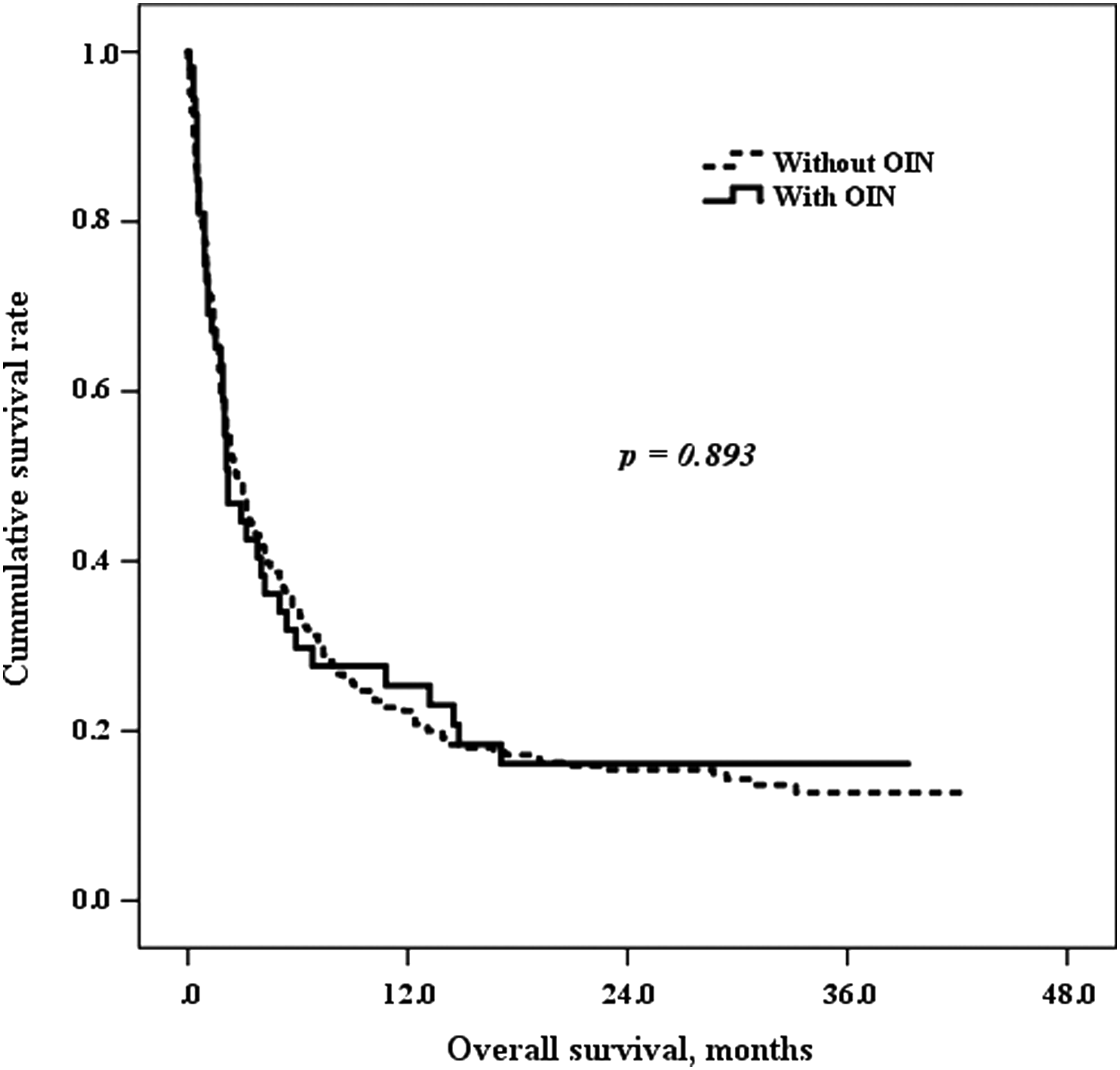
Survival between patients with OIN or those without OIN. OIN, opioid-induced neurotoxicity.
Discussion
In this study of 390 consecutive patients with advanced cancer who underwent PCT consultation, 15% experienced more than one symptom of OIN, which was associated with high MEDD or a high baseline ESAS pain score, drowsiness, and poor appetite. OIN was not significantly associated with a short life span.
OIN can be difficult to control and can be misinterpreted as disease progression; in addition, it is associated with increased suffering in patients with advanced cancer. Particularly in the nonpalliative care environment, there can be a certain nihilism with advanced cancer patients, a willingness to attribute any rapid decline in status to disease progression. This is one precise scenario in which palliative care management might improve prognosis, as we have learned that it is important to be alert to reversible complications of the drugs in use.
The definitions of many OIN symptoms are not clear in many studies. For instance, the rate of opioid-induced drowsiness in previous study ranged from 3% to 88%, as previously reported.17–19 However, studies with higher opioid doses seemed to have the highest incidences of drowsiness, indicating an association between drowsiness and dose. In our study, 6.2% of patients (n = 24) with advanced cancer receiving palliative care experienced opioid-induced drowsiness.
Similar findings were observed in regards to the diagnosis of delirium. The incidence of delirium varies from 15% to 50% in elderly patients admitted to a general medical floor to as high as 80% of patients who are near the end of life.20,21 The incidence of delirium was associated with higher and long duration of opioids. Thwaites et al. showed that 27% of terminally ill hospice patients who received continuous parenteral hydromorphone experienced delirium and that delirium was significantly associated with a higher dosage and a longer duration of continuous infusion. 16 De la Cruz et al. reported that 13% of patients developed delirium from medication, including opioids. 22
This study also indicated that patients with a diagnosis of delirium had a lower median OS duration than did those without delirium. Therefore, it is more important to screen for the presence of delirium, especially in patients undergoing palliative care. In our study, opioid-induced delirium occurred in 6.9% of patients. Unlike in previous studies,22,23 opioid-induced delirium was not associated with OS duration, which may be attributed to recovery after appropriate management. In addition, opioid rotation has been associated with delirium reversibility, 23 indicating that it could be a treatment option for opioid-induced delirium.
Our study confirmed that a high dosage of opioids was a risk factor for OIN. 2 We also found that MEDD was associated with the frequency of OIN (i.e., the higher the MEDD, the more frequently OIN was reported). On the basis of these findings, disease progression, as evidenced by poor performance status and poor appetite, could be considered a risk factor for the onset of OIN. Clinicians should pay more attention to patients with such risk factors when prescribing opioids.
In regards to the management of OIN, we found that opioid rotation is still the most popular solution. Together with the findings that OIN was not significantly associated with a shorter OS duration and that OIN symptoms were more frequent in a cohort of advanced cancer patients with poor performance scores, higher symptom burden, and higher MEDD who underwent inpatient palliative care, one possible and important reason for OIN may be inappropriate opioid dosing for pain syndromes that are relatively unresponsive to the usual opioids and the availability of treatment strategies, such as opioid rotation, that can easily alleviate this syndrome. Therefore, OIN screening and management should be part of routine cancer care. 23
Our study identified various factors that were associated with an increased risk of OIN (high MEDD or a high baseline score of ESAS pain, drowsiness, and appetite). Future studies should validate these findings and determine whether routine assessment and treatment of these risk factors and OIN, such as with opioid rotation (Table 3), would be effective in OIN.
There are several limitations to our study due to its retrospective nature, such as missing data and limited data on the natural history of OIN symptoms. Further studies are needed to evaluate the time interval after the initial evaluation to determine a diminution of sedation and delirium after opioid rotation or reduction and thus optimize treatment of OIN. A considerable number of delirium cases were caused by multiple factors, such as infection, dehydration, opioids, and hypercalcemia. These patients were treated with several simultaneous corrections, including hydration, antibiotics, and opioid rotation or reduction.
In cases of drowsiness, many patients with advanced cancer took hypnotics or antidepressants together with opioids, which likely resulted in more sedation. However, we did not count these patients with multifactorial causes, as we had a priori defined criteria for the diagnosis of opioid-induced drowsiness or delirium in this study. Therefore, opioid-induced drowsiness or delirium might have been underestimated in this study. Prospective studies should capture such information with more accuracy in the future.
Footnotes
Acknowledgment
Ann M Sutton, PhD, ELS, Department of Scientific Publications, The University of Texas MD Anderson Cancer Center, for article review.
Author Disclosure Statement
No competing financial interests exist.
This publication was partially supported by the National Institute of Nursing Research of the National Institutes of Health under Award Number R21NR016737 (S.Y.).