
Abstract
Abstract
Background:
Palliative care (PC) needs in patients with neurological diseases are becoming more recognized by neurologists and PC physicians.
Objective:
To qualify and quantify the PC education available in the United States adult neurology programs since the Accreditation Council for Graduate Medical Education (ACGME) published updated mandates in 2009.
Design:
A 22-question survey was electronically distributed to each neurology residency program in the United States.
Setting/Subjects:
All program directors (PDs) and assistant/associate program directors (APDs) of adult neurology programs.
Results:
This study had a 35% survey response rate (49 programs). Of the participating programs, 20% offer no PC education to residents. Communication, prognostication, and withdrawing life-prolonging therapies were the domains identified as the most important for resident education; these were also the domains PDs/APDs were most comfortable providing for their own patients, and the domains their residents are the best trained in currently. Addressing spiritual distress was the domain considered the least important, the domain PDs/APDs were least comfortable providing for their own patients, and the domains residents are currently the least well-trained in. Forty-two percent of programs were dissatisfied with the PC education available at their program. Time for teaching, availability of faculty, and faculty expertise were the most common barriers.
Conclusions:
PC education varies greatly across the United States adult neurology residency programs despite ACGME requirements. As time and resources limit current training, utilization of interdisciplinary educational teams and nationally available PC educational material may improve implementation of PC education in these residency programs.
Background
P
Increasingly, this recognition of the need for PC has resulted in the proposed integration of PC education into medical training across all levels. 19 In actuality, the quality and quantity of such education varies vastly between specialty programs and across institutions. Prior studies, among other subspecialties, demonstrated poor resident knowledge of PC topics, with a mean knowledge score of 44%. 20 The Accreditation Council for Graduate Medical Education (ACGME) mandated all residents in an adult neurology residency program “must demonstrate knowledge of palliative care,” only specifically mentioning pain relief, psychosocial support, and counseling in that requirement. 21 No studies have characterized how this requirement has been implemented in adult neurology residency programs. To improve neurology pedagogy, we sought to better characterize the PC education administered to residents in the United States adult neurology residency programs.
Design
The University of Virginia Institutional Review Board exempted this study from further review. There were no financial incentives offered for completion or participation in this study and participation was voluntary.
Survey development
We developed an anonymous, 22-question survey addressing 10 domains of PC. These domains overlapped across multiple resources, including the ACGME guidelines for PC education in neurology residency, educational milestones for PC fellowship, and in surveys of prior studies on PC education in non-neurology residencies and fellowships (emergency medicine residency, psychiatry residency, gynecologic oncology fellowship, pulmonary, and critical care fellowship).13,17–21 The survey included Likert questions, multiple choice questions, and free-text boxes for qualitative responses. All questions were optional and completion was not required to end the survey. The full survey is available in Table 1.
APD, associate program director; PC, Palliative care; PD, program director.
Participants
All adult neurology residency programs listed on the ACGME website as of May 2017 that were accredited at the time of survey distribution were eligible for inclusion in this study. Programs were excluded if they did not have any current residents. Names and contact information for program coordinators, program directors (PDs), and assistant/associate program directors (APDs) were obtained from the publicly available ACGME website and individual program websites. 22
Survey distribution
We distributed the web-based survey to 142 adult neurology residency programs using Qualtrics Research Suite (Qualtrics LLC) software in June 2017. Each program received one survey embedded with the IRB consent form. The authors initially contacted PDs directly through publicly available contact information or through program coordinators. PDs were sent reminder emails at one week after initial distribution. At two weeks, PDs were contacted by phone. At six weeks, APDs were contacted with an initial email. No APDs were contacted by phone. The survey was closed 10 weeks after distribution.
Data analysis
Data were summarized through the Qualtrics Research Suite software and Microsoft Excel program.
Results
Baseline characteristics of participating adult neurology residency programs
Of 148 adult neurology programs, 6 programs without active residents were excluded. Fifty programs initiated the online survey of which one was incomplete and excluded (35% response rate) and three were completed by APDs (6.4%) (Fig. 1). Baseline characteristics of participating programs are shown in Table 1. Programs employed between 14 and 160 neurology faculty members, working with between 4 and 42 residents. The majority of responses received were from programs affiliated with university hospitals (92%) and completed by the PD (92%).
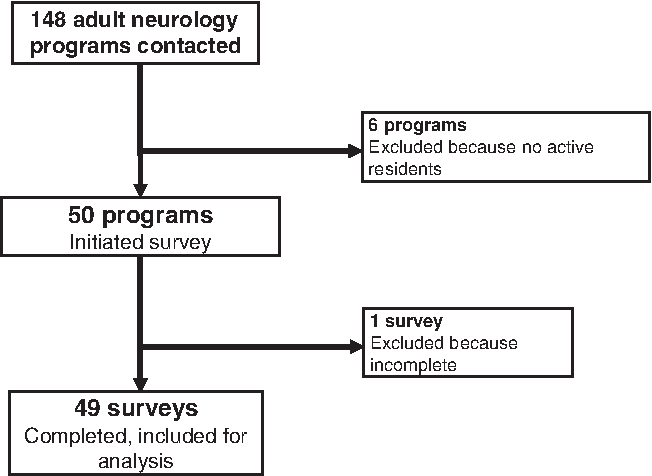
Study inclusion and exclusion criteria. Of 148 United States adult neurology programs, 6 programs were excluded because they had no residents at the time of survey distribution and 1 was incomplete and therefore excluded.
Current PC education in adult neurology programs
Nearly all participating programs (90%) had a PC specialty service at their institution. At those programs with formal PC education (80%), PC faculty, neurology faculty without any PC training, and ethics faculty provided the majority of the PC education (Table 2). Formal PC education for residents includes structured education identified by program leadership specifically as PC or end-of-life care.
AAHPM, American Academy of Hospice and Palliative Medicine; CAPC, Center to Advance Palliative Care; DNR, do not resuscitate; DNI, do not intubate; EPEC, Education in Palliative and End-of-Life Care; NRELEP, National Residency End-of-Life Education Program.
According to PDs/APDs, the most important domains in PC education for neurology residents were communication, prognostication, and withdrawing life-prolonging therapies. PDs/APDs identified addressing spiritual distress, nonpain symptom management, and care of the imminently dying as domains with lesser importance (Fig. 2).
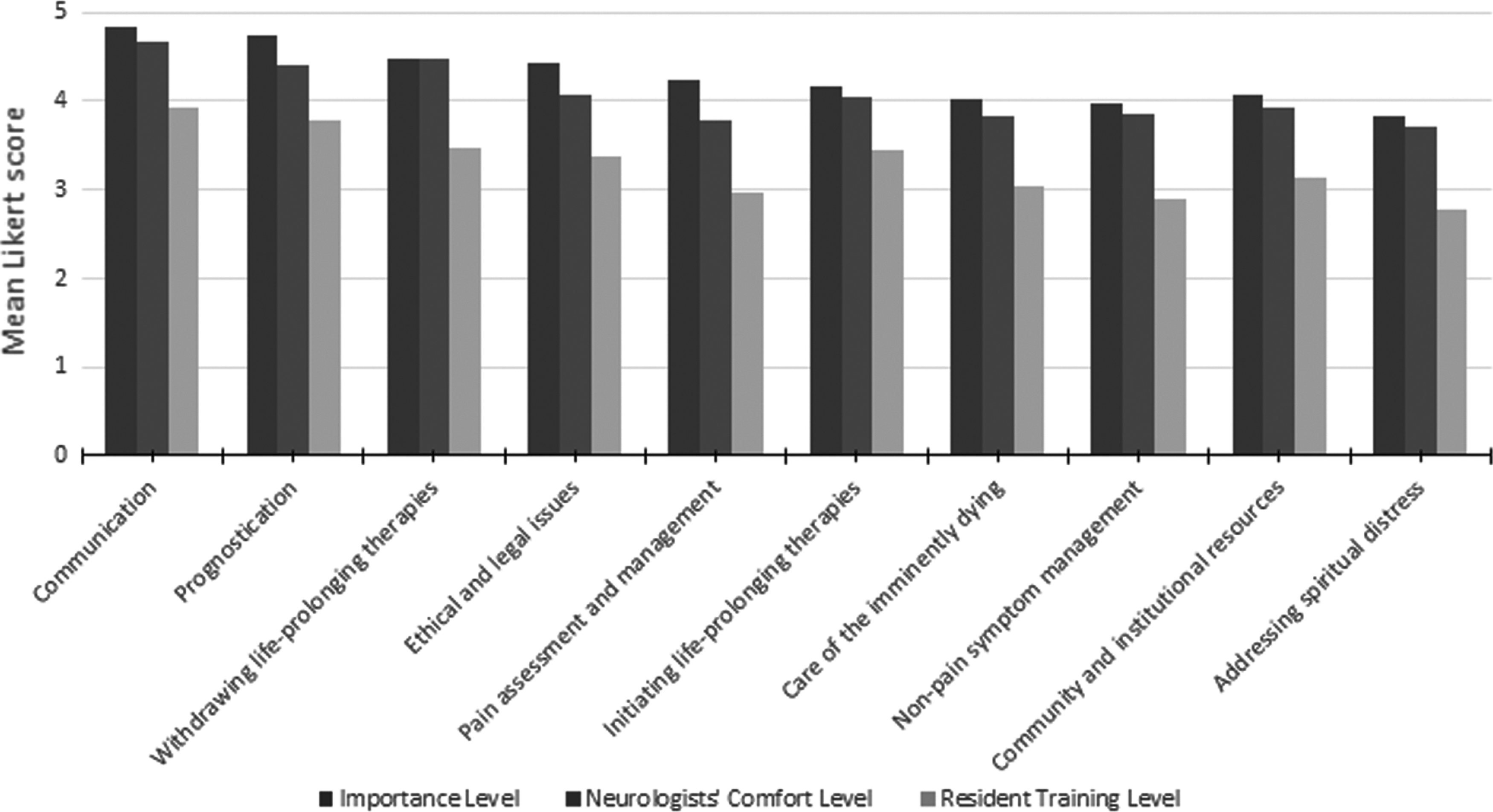
Evaluation of current palliative care educational domains by program directors/assistant program directors of adult neurology residency programs. Mean Likert scores of participating adult neurology residency programs assessing the current palliative care education available in their programs by palliative care domains. Residency program directors and assistant program directors answered the following questions: (1) How important do you believe it is for neurology residents to receive education on the following palliative care topics? (designated as “importance”) (2) As a neurologist, how comfortable are you with providing the following palliative care for your patients? (designated as “comfort”) (3) How well do you think your neurology residents are trained in the following palliative care topics? (designated as “resident training”). Each Likert response was assigned a numerical value (none = 1, extremely = 5). The mean Likert score was calculated.
Responding programs reported they most commonly utilize some form of formal didactics (seminars/conferences or small group/role playing) and elective rotations to teach PC (Fig. 3). They also reported that formal didactics, specifically seminars/conferences, are the least effective method of delivery. Responding programs reported self-directed reading materials, formal didactics seminars/conferences, and formal didactics small group/role playing as the least effective methods of providing PC education. Programs reported using no predeveloped materials (33%), using materials developed independently (28%), or using nationally available educational materials (38%). Education in Palliative and End-of-Life Care (EPEC), Neurology Residency End-of-Life Physician Education Project (NRELEP), and Fast Facts Palliative Care Network of Wisconsin were most commonly used (Fig. 4).
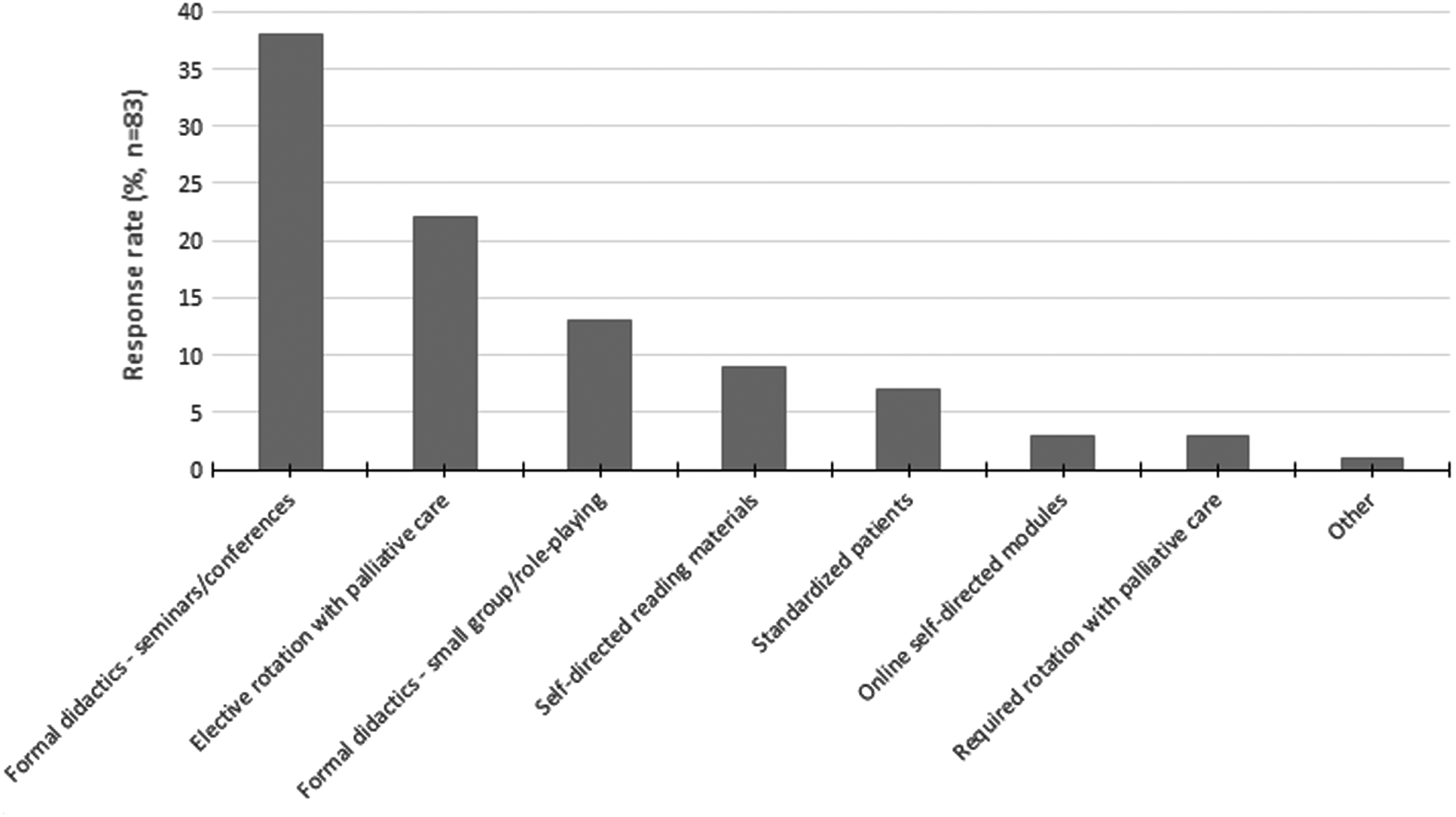
Palliative care teaching methods currently utilized in adult neurology residency programs. The methods of delivery of palliative care education currently being utilized in adult neurology residency programs. Programs were asked to identify which education methods they currently utilized and which are the least and most effective. Responses were not limited to one answer.
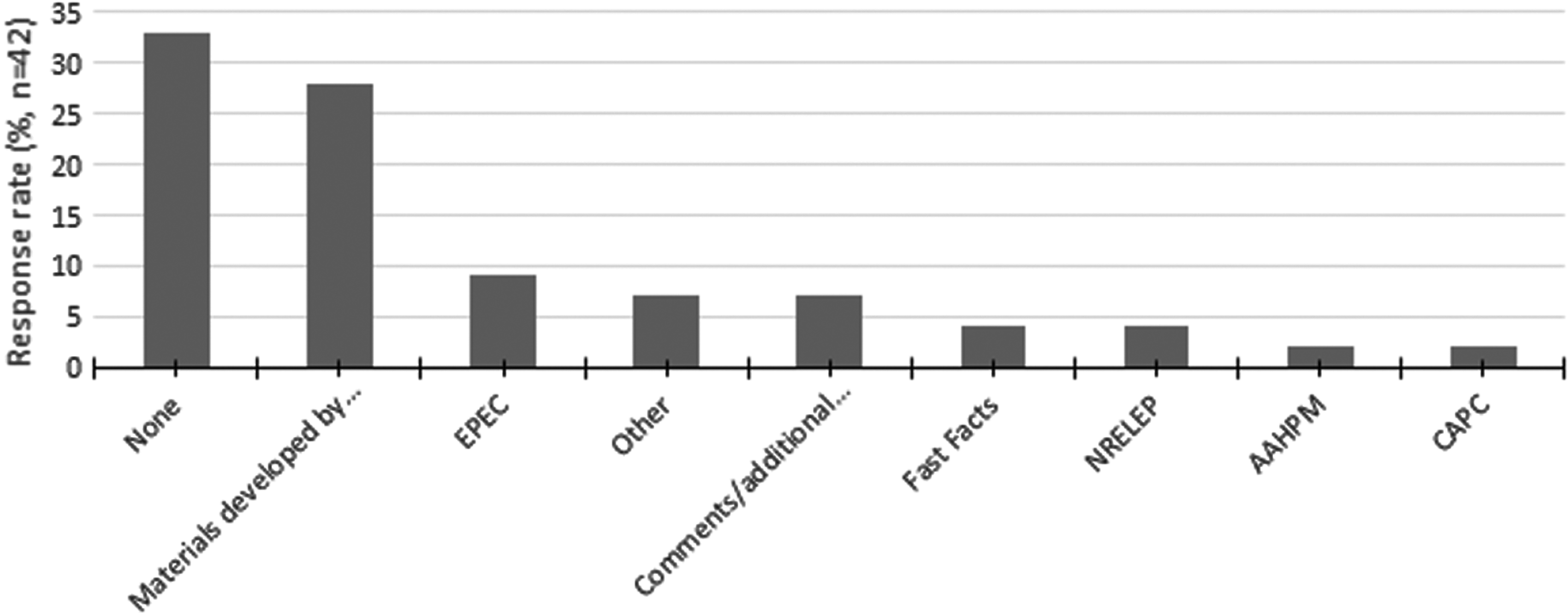
Nationally available palliative care education tools utilized in adult neurology residency programs. Programs were asked to identify which nationally available palliative care educational resources they currently utilize to teach their neurology residents. Responses were not limited to one answer. EPEC, Fast Facts–Palliative Care Network of Wisconsin, NRELEP, AAHPM, CAPC resources. AAHPM, American Academy of Hospice and Palliative Medicine; CAPC, Center to Advance Palliative Care; EPEC, Education in Palliative and End-of-Life Care; NRELEP, Neurology Residency End-of-Life Physician Education Project.
Examples of materials developed by programs were described as “vital talk and modified communication workshop developed at our program,” “lectures designed by our palliative care faculty,” “standardized patients and didactics,” and “case simulation.” One program commented that they “developed a brain death/difficult discussions simulation-based medical education module.” Other programs stated that they were “not sure what materials are used or if they are consistently used” and another stated they “do not know what resources the palliative team uses.”
Evaluation of current PC education in adult neurology residency programs
Survey respondents reported being extremely satisfied (10%), somewhat satisfied (48%), somewhat dissatisfied (40%), or extremely dissatisfied (2%) with the current PC education available in their adult neurology residency program.
PDs/APDs identified the domains of communication, prognosis, and withdrawing life-prolonging therapies as the domains in which their residents are the most well trained. The domains of addressing spiritual distress, nonpain symptom management, and pain assessment and management as the domains in which their residents are the least well trained (Fig. 2).
Barriers to providing PC education in adult neurology residency programs
The domains of communication, withdrawing life-prolonging therapies, and prognostication were reported by PDs and APDs as the domains they themselves felt the most comfortable providing for their own patients. The domains they felt the least comfortable providing for their own patients were addressing spiritual distress, pain assessment and management, and care of the imminently dying.
Programs reported the most common barriers to providing PC education in adult neurology residency programs were time for teaching (28%), availability of faculty (23%), and faculty expertise (18%) (Fig. 5). In addition to the barriers listed in the survey, some respondents described other barriers, such as “residents have too many other things to learn” and “if not for the rotation on palliative service, [it] would have been very hard to provide [palliative care] experience.”
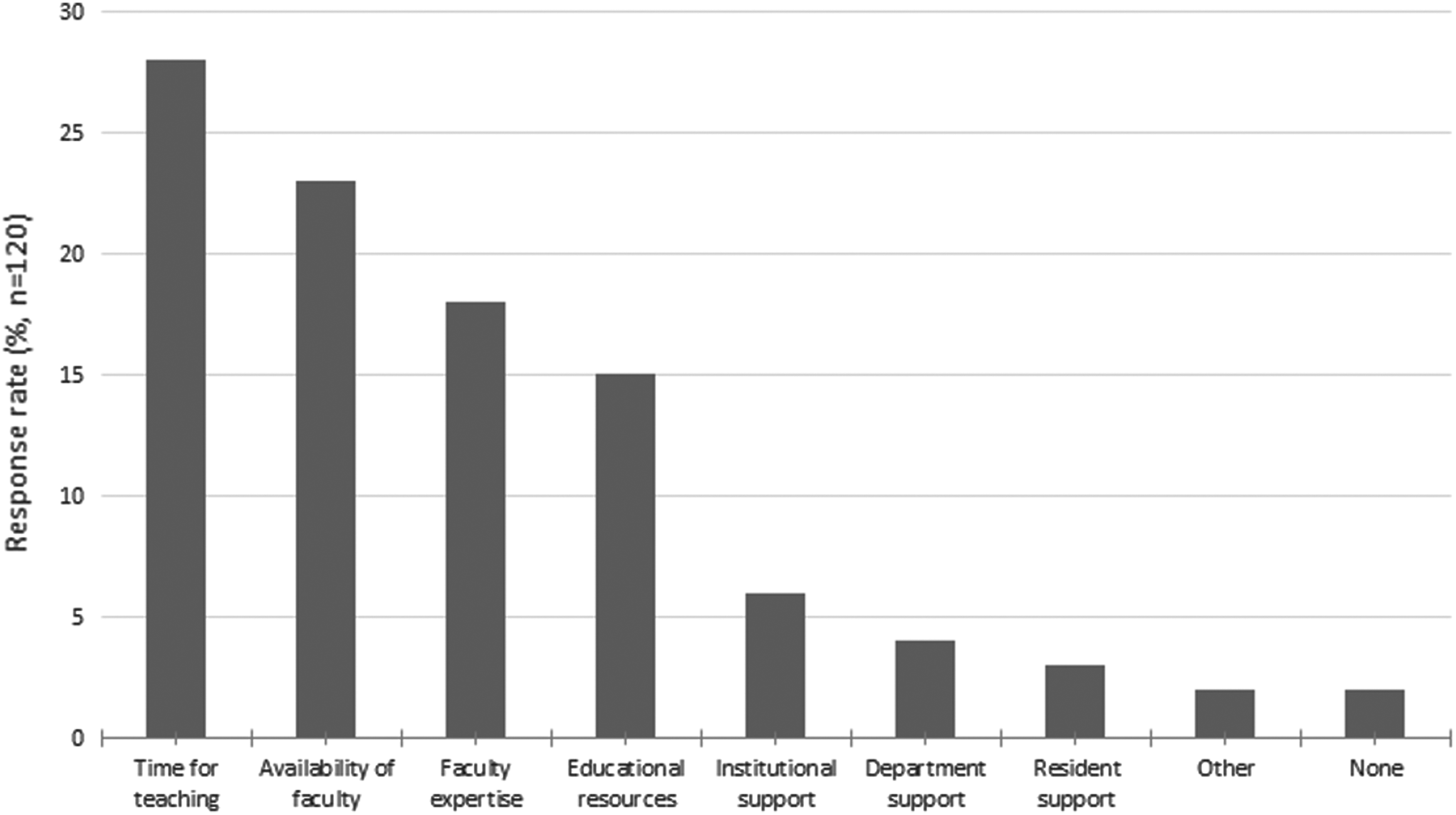
Barriers to teaching palliative care in adult neurology residency programs. Programs were asked to identify educational barriers they experience when implementing palliative care education in their adult neurology residency programs. Responses were not limited to one answer.
Discussion
The need for PC education in the current training of adult neurology residents in the United States has been previously reported and is reflected in the establishment of requirements for PC education by the ACGME. Schuh et al. evaluated the PC education in one neurology residency program before and after completing the NRELEP conference. 22 Only one study has evaluated the state of education in adult neurology residency programs; however, it did not specifically evaluate the PC education available and was published before the ACGME published its updated program requirements in 2009. 23 We sought to perform a needs assessment of PC education within the United States adult neurology residency programs since the implementation of the 2009 ACGME education requirement. To our knowledge this is the first study to comprehensively assess how neurology residency programs are providing PC education to their residents with both quantitative and qualitative responses.
Current PC education in neurology residency
Despite an increase in the amount of PC services and educational materials available nationwide, we found that one-fifth of responding programs did not have any form of PC education available in their residency program. The programs that have some form of PC education reported a wide variation in content and teaching methods.
Programs included at least one domain as important for neurology residents to learn, but each domain varied. There was also a wide range across domains that programs identified as most important to teach and which ones their residents are well trained in. The domains identified as most important to teach and the ones that residents are most well trained in also correlated with the domains PDs and APDs felt most comfortable providing for their own patients. The same was seen with domains identified as the least important (addressing spiritual distress and care of the imminently dying). This may account for some of the content differences across programs.
We also found that teaching methods are varied and the most commonly utilized methods of teaching were ones that programs reported to be the least effective. Programs identified experiential learning (rotations with the PC service, both required and elective, and standardized patients) as the most effective methods. Yet, neurology residents are less likely to receive PC education with experiential methods from our assessment.
The variation in content and implementation across programs is most likely because the ACGME requirements for PC education in adult neurology programs are vague and provide limited guidance for programs. We found a disconnect between which domains are most important for residents to learn as specified by the ACGME and by neurology programs. The domains of most importance to respondents (communication, prognostication, and withdrawing life-prolonging therapy) are not clearly identified in the ACGME requirements except to the extent that communication and prognostication intersect with “psychosocial support and counseling.” 13 Pain assessment and management was specified by the ACGME as a requirement, yet this was not reported as a domain of top priority for teaching. Addressing spiritual distress was identified as the domain in which residents were not well trained in, as one of the least important domains to be taught, and one that respondents were uncomfortable providing for their own patients. Neither is it specified in the ACGME requirements. Yet, numerous previous studies have identified the care of spiritual distress as an important component of caring for patients with neurological illnesses, which is why national PC education programs include spiritual care education.15–17,22,24,25
Barriers to PC education in neurology residencies
Lack of faculty expertise, availability, and time were identified as the main barriers to providing PC education in neurology programs. Our findings are consistent with barriers identified in prior studies in other disciplines.26,27 Prior studies suggest practicing neurologists may not be comfortable providing aspects of end-of-life care due to lack of expertise.22,28 No previous studies have evaluated barriers for teaching PC in neurology programs. The incorporation of more nationally available published PC educational materials would help to address some of these barriers by providing neurology programs with standardized PC content and expertise. Many programs reported utilizing their own educational materials. Sharing materials across programs would decrease time spent independently developing teaching content. Incorporating more interdisciplinary teaching experts would reduce the neurology faculty teaching burden and could promote satisfaction. For example, inviting chaplains to participate in formal didactics may improve residents' ability to address spiritual distress in their patients. In this study, less than 3% of programs have chaplains as faculty teaching PC to neurology residents. Additionally, inviting other professionals to teach would address the stated lack of faculty expertise. Resident, departmental, and institutional lack of interest was not identified as a barrier to teaching PC in neurology programs.
There are recognized limitations to our study. This survey included only PDs and APDs. Residents were not included, which results in reporting bias. PDs/APDs may be biased in favor of their programs; therefore, programs with little or no formal PC education or with leadership less interested in PC, may have been less likely to complete this survey. While PDs/APDs and residents are equally important stakeholders in residency programs, PDs/APDs will have unique perspectives on their program's successes and weaknesses. They may be unable to report the true efficacy of PC education in their program since their evaluation of resident PC skills may not translate directly to clinical outcomes. Future studies of residents' evaluation of their education will be necessary for program development. Despite these limitations, this study calls to attention the opinions of PDs/APDs who are ultimately responsible for the development and leadership of these educational programs. Recognizing their assessments allows for further program development and improvements.
Changes in program leadership that occurred during the data collection period may not have been reflected in the results. Our survey respondents were primarily from large, academic institutions with smaller representation by community hospitals and military programs. Therefore, constraints unique to these settings may have been missed.
Conclusions
The intention of this survey was to identify the current PC educational needs of neurology residency programs. We found that despite existing ACGME requirements and programs' interest in providing this education, the delivery method and content continues to be heterogeneous across programs. This suggests future collaborations between neurology and PC departments are necessary to improve the quality and availability of PC for patients with neurological diseases. Neurologists and PC specialists should write more content together and share these overlapping resources. Clinical experiences could be joint. For example, patients referred to PC specialists by neurology residents could be seen together both in the inpatient and outpatient settings. PC fellows and neurology residents could join team rounds to improve exchange of ideas and learning. Just as PC fellowships emphasize interdisciplinary education, neurology residencies could ensure formalized education, including presentations, conferences, and didactics that are taught by interdisciplinary educators, such as chaplains, social workers, and pharmacists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.