
Abstract
Abstract
Background:
Preoperative advance care planning (ACP) may benefit patients undergoing major surgery.
Objective:
To evaluate feasibility, safety, and early effectiveness of video-based ACP in a surgical population.
Design:
Randomized controlled trial with two study arms.
Setting:
Single, academic, inner-city tertiary care hospital.
Subjects:
Patients undergoing major cancer surgery were recruited from nine surgical clinics. Of 106 consecutive potential participants, 103 were eligible and 92 enrolled.
Interventions:
In the intervention arm, patients viewed an ACP video developed by patients, surgeons, palliative care clinicians, and other stakeholders. In the control arm, patients viewed an informational video about the hospital's surgical program.
Measurements:
Primary Outcomes—ACP content and patient-centeredness in patient–surgeon preoperative conversation. Secondary outcomes—patient Hospital Anxiety and Depression Scale (HADS) score; patient goals of care; patient and surgeon satisfaction; video helpfulness; and medical decision maker designation.
Results:
Ninety-two patients (target enrollment: 90) were enrolled. The ACP video was successfully integrated with no harm noted. Patient-centeredness was unchanged (incidence rate ratio [IRR] = 1.06, confidence interval [0.87–1.3], p = 0.545), although there were more ACP discussions in the intervention arm (23% intervention vs. 10% control, p = 0.18). While slightly underpowered, study results did not signal that further enrollment would have yielded statistical significance. There were no differences in secondary outcomes other than the intervention video was more helpful (p = 0.007).
Conclusions:
The ACP video was successfully integrated into surgical care without harm and was thought to be helpful, although video content did not significantly change the ACP content or patient–surgeon communication. Future studies could increase the ACP dose through modifying video content and/or who presents ACP. Trial Registration: clinicaltrials.gov Identifier NCT02489799.
Introduction
Although most surgeries are performed successfully, perioperative morbidity and mortality can still be associated with these procedures.1–3 While patients at higher risk for complications can sometimes be identified, it is impossible to predict exactly which patients will die or suffer a major perioperative complication.2–4 Consequently, preoperative advance care planning (ACP) may benefit surgical patients, their family members, and providers. ACP allows individuals to contemplate future health states, clarify and discuss goals, and express goal-informed wishes for those health states—particularly if future illness may render the person unable to make decisions. 5 Demonstrated to be appropriate and nonharmful throughout multiple stages of illness 6 and associated with improved outcomes,7–12 ACP is recommended by key organizations such as the American Society of Oncologists, the National Comprehensive Cancer Network, and the Institute of Medicine.13–15 Previous studies suggest surgical culture resistance to integrating ACP and palliative care-related practices, particularly during the preoperative period.16–21 A recent systematic review of palliative care interventions for surgical populations 22 highlighted five studies23–27 that tested ACP in surgical populations; although the studies were overall small in size, preoperative ACP was associated with no harm to participants, improved concordance and decreased decisional conflict about goals of care,23,25,26 and improved documentation regarding power of attorney. 27 Study participants also deemed preoperative ACP to be helpful. 26
While verbal communication is the predominant ACP modality, 28 13 randomized controlled trials report that video-based ACP is effective and safe,29–41 although none were performed in surgical populations. Video-based ACP provides inherently stable content through a realistic modality that introduces ACP and educates and activates the patient to contemplate ACP wishes and discuss them with their medical team.42,43 Therefore, the objective of the current study was to develop and test the feasibility, safety, and early effectiveness of an ACP video developed for patients pursuing major surgery for cancer. In particular, we hypothesized that an ACP video could be successfully and safely integrated into surgical care and that patients who viewed the ACP video would engage more in preoperative ACP and patient-centered communication with their surgeons.
Methods
The study protocol has been previously published. 44
Study design
The study was a two-arm, phase II randomized trial of an ACP video developed for patients undergoing major cancer surgery compared with a control video that described the surgery department at the hospital, but contained no ACP content.
Study cohort
The sample included patients undergoing surgery with one of nine cancer surgeons at an academic tertiary care center. Inclusion criteria were age ≥18 years; nonemergent surgery with a participating surgeon with at least a day, optimally a week, to review the video before surgery; planned postoperative admission to the surgical intensive care unit; ability to give informed consent; and ability to speak and understand English (as both study videos were in English). Patients were excluded if they had visual or hearing impairments such that they were unable to view and/or hear the study videos.
Study setting
Patients were recruited from each surgeon's outpatient surgical oncology clinic. In study preparation, surgeons described practice variations regarding presurgical visits and agreed on a single format. Surgeons were shown and agreed with both study arm videos. Surgeons, patients, the principal investigator, and the study biostatistician were blinded to patient randomization.
Study arms
Intervention video
The ACP intervention video was developed through a two-year process of intense engagement with palliative care clinicians, surgeons, patients and family members, perioperative nurses, and video ACP experts.45–51 Analogous to a drug trial, the video's ACP content was considered the drug to be tested with the dose and delivery of that ACP content heavily discussed, debated, and piloted throughout the development process. A systematic review revealed no existing surgical ACP videos 46 and thus video content was developed through interviews with surgeons, palliative care and ACP experts, and other stakeholders, 47 as well as through stakeholder summits.48,49 For a phase I trial of ACP video content, storyboards of the proposed video were reviewed by 365 self-identified surgery patients and/or family members; the content was deemed safe and helpful, and participant input was incorporated into final video content and clinical trial design. 49 The video was filmed, edited, and further refined through engagement with 70 stakeholders, including patient and family members, palliative care clinicians, and surgeons of diverse surgical practices and geographical regions. 51 The final video featured the following: (a) patients and family members discussing preparing for, undergoing, and recovering from major surgery and recommending preoperative ACP; (b) video footage of a patient and her family going through the surgery process from preoperative preparation area to operating room to the postsurgical intensive care unit; (c) physicians and nurses relating advice for patients preparing for surgery and specifically recommending ACP, and (d) final written and spoken messages that instructed patients to do the following: “Before surgery, identify the person who speaks for you and talk to that person. If issues should arise, that person needs to be ready to speak for you. Tell your surgeon and surgical team who will speak for you.” The intervention video is not publicly available.
Control video
The control video (125th Anniversary of The Johns Hopkins Hospital) was an informational video about the Johns Hopkins surgery program, which was independently created in 2014 by their marketing department. Cataloging the history and evolution of surgery at Johns Hopkins Medicine, the video highlighted scientific developments and innovations in patient safety and contained no ACP content.
Both videos were six minutes in duration. With each study patient as a unit of randomization, we randomized immediately following enrollment. Contamination bias was minimized through allocation blinding among participants. Hypothesizing that surgeon demeanor differences could impact some outcomes, randomization was stratified by surgeon with a block size of six. Immediately following randomization, patients viewed their allocated video in the surgeon's clinic in the presence of study staff and took home a password-protected video web link should they wish to rewatch it.
Study outcomes
Primary outcomes
Both primary outcomes were derived from audio-recorded preoperative conversations among surgeons and patients where they discussed the risks and benefits of the planned surgery and patients signed surgical consent. Audio recordings were analyzed using the Roter interaction analysis system (RIAS), which is a quantitative coding system for medical dialog with demonstrated reliability and predictive validity for patient satisfaction, utilization, and adherence.52–57
The coding unit of analysis is a complete thought that varies in length from a single word to a sentence. This study had two coders, who were blinded to patient allocation. Reliability of RIAS coding was calculated as the Spearman correlation coefficient between the two coders for all communication categories. Intercoder reliability was high, averaging 0.89. RIAS was used to capture the primary outcomes:
ACP content: Content-specific ACP communication markers were determined from a prior study
58
and the study team's review of initial recordings. Codes included medical decision maker/ACP (code of greatest interest), immediate death during surgery, long-term death after the surgery, severity/significance of the planned surgery, and goals for the surgery. Patient-centeredness: Patient–provider patient-centeredness52–57
is a ratio of statements that reflect the psychosocial and socioemotional elements compared with the biomedical and disease-focused elements of the patient's lived illness experience. This score reflects the conversation as a whole, rather than an individual's dialog. A value greater than one indicates a more patient-centered encounter, whereas a value less than one indicates a less patient-centered encounter.
Secondary outcomes:
Hospital Anxiety and Depression Scale (HADS),
59
The Iowa Goals of Care survey
60
includes seven nonmutually exclusive goals for why patients seek out medical care: “cure my medical condition,” “allow me to live longer,” “improve my current health,” “maintain my current health,” “allow me to accomplish something particular in my life, a personal life goal,” “make me comfortable,” and “learn more about my disease or health.” Helpfulness of the Video survey—a three-item measure regarding patient perceptions of ACP video helpfulness, which has been used in previous studies.29,35–37,39,42 Patient and Surgeon Satisfaction surveys—two six-item measures developed and used by Roter et al. to address either patient or surgeon satisfaction with interpersonal and informational aspects of medical visits.61–64
Medical decision maker designation—at study enrollment and study completion, patients answered whether they had designated a medical decision maker.
Analytical and statistical approaches
Sample size calculation
The study was powered based on previous studies utilizing RIAS.58,65 Based on these data and with a 0.6 effect size, the required sample size was 72 patients (36 per group) for a one-tailed test of study hypotheses (power = 0.8 and alpha = 0.05). Based on a previous study, 66 we hypothesized that we would obtain recordings for 80–90% of recruited patients and, accounting for an 80% rate, a desired number of 72 recordings would require recruitment of 90 patients.
Statistical approaches for study outcomes
Statistical analyses were performed using Stata statistical software 67 and rerun with R statistical software 68 for confirmatory analysis. Summary univariate statistics (mean, standard deviation, median, interquartile range, max, min, count, and percentage) of outcomes stratified by intervention assignment were determined. Differences in outcomes between study arms at each visit were tested by a two-sample t test/Mann-Whitney test or Fisher's exact test/chi-squared test based on the data type. If appropriate, descriptive statistical analyses were followed by multilevel modeling analyses, using generalized estimating equation models. 69 To address the potential unmeasured surgeon-level attributes on patient-level outcomes, we nested the models by surgeon. Models assumed either an exchangeable or independent covariance structure and robust standard errors. For many outcomes, the parameter of interest was intervention effect, the coefficient of the arm indicator.
Conduct of the study
The Johns Hopkins School of Medicine and the Sidney Kimmel Comprehensive Cancer Center Institutional Review Boards reviewed and approved the study. A Data and Safety Monitoring Board reviewed study results approximately halfway through the study.
Results
Ninety-two patients were enrolled in the study, with 45 patients randomized to the intervention and 47 randomized to the control video (Fig. 1). There were no differences between the intervention and control groups on demographics, including age, sex, race, and primary diagnosis (all p > 0.05) (Table 1). Average age was 60.4, and participants were 86% white, 11% African American, and 63% female. The most common primary diagnoses were pancreatic cancer (31.5%) and hepatobiliary/other gastrointestinal cancers (27.2%).

CONSORT diagram. *Due to technical error or withdrawal of audio recording consent, not all preoperative consent visits (V2) were recorded and used in RIAS. RIAS was based on 61 recordings; 31 control recordings and 30 intervention recordings. RIAS, Roter interaction analysis system.
Baseline Characteristics of Study Patients
ACP, advance care planning; SD, standard deviation.
The ACP video was delivered successfully to all participants in the intervention arm with no harm noted in either study arm at any time. Due to several factors, including emergent surgery or patient decision to not undergo surgery or undergo surgery at another hospital, 61 participants had patient–surgeon conversations that were audio-recorded and analyzed.
Primary outcomes
There were no differences in discussion of ACP content between intervention and control groups, although surgeons and participants in the intervention group were more likely to discuss ACP/medical decision maker (23% vs. 10%, p = 0.182, Table 2). Patient-centeredness did not differ between study arms (IRR = 1.06, confidence interval [0.87–1.30], p = 0.545, Table 3). While slightly underpowered, study results did not signal that further enrollment would yield statistically significant results.
Measured Advance Care Planning Content in the Presurgical Consent Visit (Primary Outcome)
No values are statistically significantly different in this table.
Measured Patient-Centeredness in the Presurgical Consent Visit (Primary Outcome)a
A value greater than one indicates a more patient-centered encounter emphasizing psychosocial and socioemotional communication, whereas a value less than one indicates a less patient-centered and more biomedical encounter.
CI, confidence interval; IRR, incidence rate ratio.
Secondary outcomes
HADS total scores (Table 4) remained stable before surgery (V1 and V2), peaked at postoperative one week (V3), and then dropped at one month in the postoperative period (V4); there were no differences between study arms. Among participants in both study arms and at all four study time points, patients most frequently indicated that their goal was to cure their medical condition (Fig. 2). In both groups and across all time points, the same three goals were also most frequently selected: “cure my medical condition” (94%), “allow me to live longer” (94%), and “improve my current health” (85%). Compared with the control video, participants more likely rated the ACP video as very helpful or somewhat helpful (p = 0.007; Table 5). There were no differences between study arms in whether participants felt comfortable with the video (p = 0.908) or would recommend the video to others (p = 0.526). Both patients and surgeons reported high satisfaction with communication, with no differences between study arms. At baseline, a majority of patients in both intervention (80.0%) and control (76.6%) arms reported having a designated surrogate decision maker. By study end, that designation increased in both intervention (80.0% to 94.4%) and control (76.6% to 100%) arms with no statistically significant difference between the two.
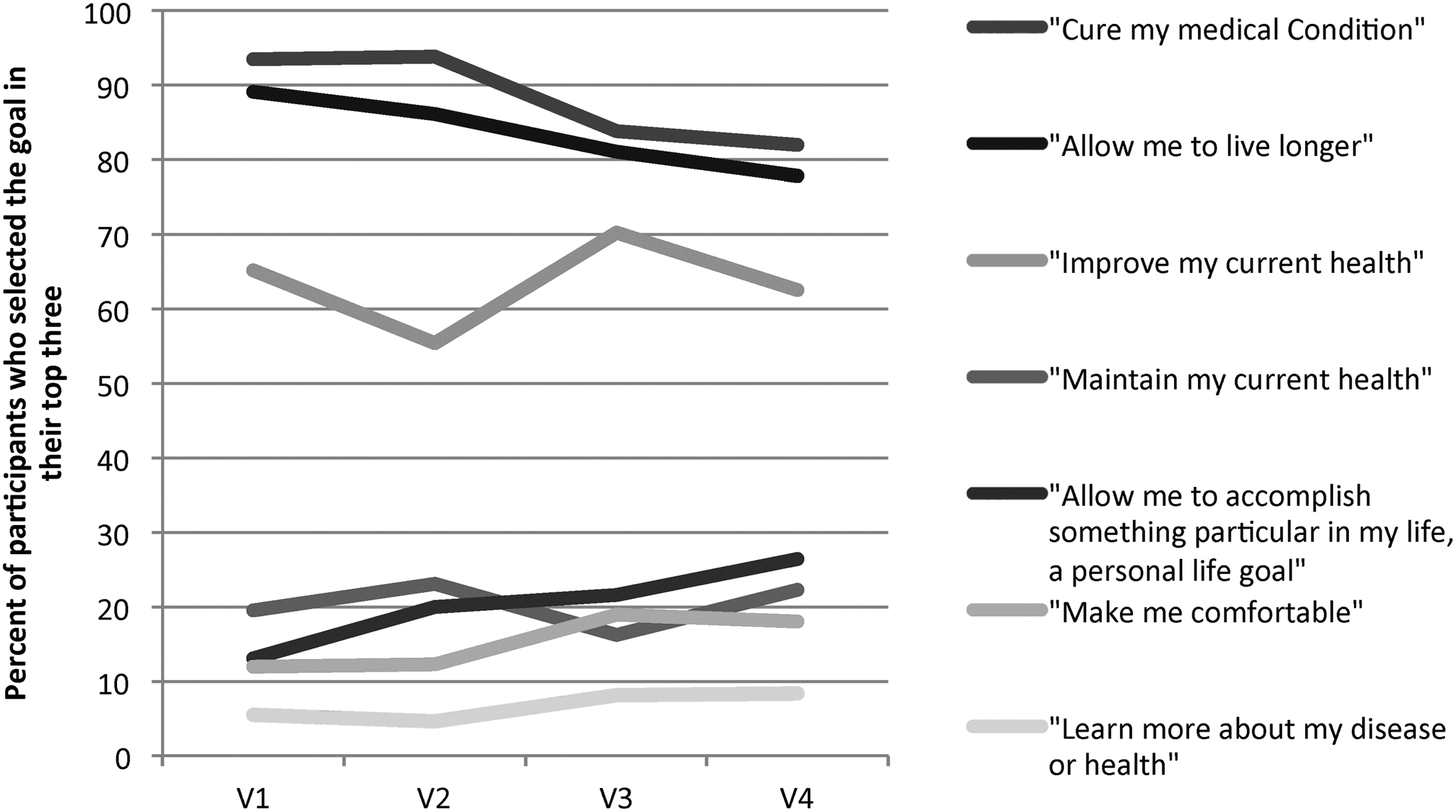
Iowa Goals of Care goal selection variation throughout the clinical trial time period.
Hospital Anxiety and Depression Total Scores Across Study Arms throughout the Study Period
No values are statistically significantly different in this table.
HADS, Hospital Anxiety and Depression Scale.
Helpfulness of the Video Across Study Arms, Collected Immediately after the Audio Recording at the Presurgical Consent Visit (Fisher's Exact p = 0.007)
Approach to missing data
Eighteen enrolled patients did not complete all four study visits and therefore complete longitudinal data were not available for this subset. To examine potential differences among the patients who completed and did not complete the study, bivariate analyses comparing study completion and varied characteristics were assessed and no differences were observed between the two groups in demographics, randomization, surgeon, medical history, companion presence in the visit, or postoperative outcomes. As no differences were observed, all available data were used for analysis.
Discussion
Study results support that an ACP video can be safely and feasibly integrated into preoperative surgical oncologic care and that the video was thought to be helpful by participants, although the ACP video did not change the ACP content, nor the nature of surgeon–patient conversation. All patients had worse mood symptoms one week following cancer surgery compared with baseline, and nearly all participants were pursuing surgery primarily with the goal of seeking a cure for their cancer.
When we initially proposed this study in 2012, there was no ACP research completed in surgical oncologic populations, and this topic was considered novel (if not antithetical).16–21 Since then, ACP and palliative care have become more accepted and prevalent in medical environments 70 as well as in the lay public, including the best-selling books written by cancer surgeons, Being Mortal and When Breath Becomes Air.71,72 A recent research agenda specifically calls for more research regarding ACP and palliative care in surgical populations.22,73
From study inception, the dose of ACP in the video was controversial. During video development, the majority of patients and family members advocated for a stronger ACP dose than was felt acceptable by many of the surgical oncologists who advised us. Ultimately, we noted surgical oncologists to be the gatekeepers whose approval was essential for video success and dissemination; patients were unlikely to see the video if it was not recommended by their surgeon. Consequently, we worked closely with our surgeon partners on the final video. 74
The video's ACP dose included the sentiment—conveyed three ways—that while surgery is overall safe, risks still exist and patients should
contemplate their goals and beliefs about health states such as having a stroke or being dependent on machines for activities such as breathing and eating;
designate a friend or a family member who can speak for them in those rare circumstances and to tell that person their wishes; and
tell their surgeon about who would make decisions for them if they cannot by themselves and continue this conversation with their surgeon and surgical team.
In light of study results, one could argue that perhaps this ACP dose should have been more explicit or that the ACP should have been discussed more than once; evidence suggests that increased dose frequency of palliative care visits, which include ACP, improves effectiveness. 75 Also of interest, some cancer patients may think it important to discuss ACP with a physician, but they may not want that physician to be their oncologist. 76
In February 2017, we convened a stakeholder summit to discuss study results with 13 engaged cancer surgeons, palliative care clinicians, patients, family members, and ACP experts; 9 were involved in video development and 4 were new to the project. These participants felt the video ACP dose to be sufficient and suggested other approaches to increase ACP dose, including
ACP-related communication skills training and/or tools for cancer surgeons and other surgical providers to better enable them to facilitate goal-related ACP conversations;
move emphatic introductory framing by cancer surgeons or members of the surgical team to recommend the ACP video; and/or
exploring other systems where a nononcologist—a communication facilitator and/or palliative care expert, instead of the cancer surgeon, would have the ACP conversation(s) with the patient and then, if needed, include the cancer surgeon and surgical team for further discussion.
We believe each approach has benefits and drawbacks and that cancer surgeons, palliative care clinicians, surgical teams, and patients and their family members should have multiple evidence-supported options. We encourage and await future studies testing ways to improve surgeon–patient communication surrounding ACP 77 ; our team recently received funding for a multicenter trial comparing surgeon-alone management versus surgeon–palliative care team comanagement of patients pursuing surgery for upper gastrointestinal cancers. 78
Study limitations
Several study limitations should be noted. First, study outcomes and time frame may not fully capture the intervention effect; for example, other studies have shown ACP discussion benefits for up to 12 months after hospitalization and/or patient death. 79 Second, participant surgeons may be biased in their preexisting support for ACP and/or may have had unconscious selection biases when referring study patients. Aware of patient participation in the trial, surgeons may also have altered their ACP communication, although study results still support low prevalence (<24%) of ACP discussions between surgeons and patients, particularly in the control arm (<10%). Third, while 92 patients were enrolled in the trial, only 61 had audio recordings, fewer than the 72 designated in the sample size calculation. This discrepancy was due to a lack of audio recording if the patient experienced unpredictable changes in surgery scheduling and/or patient disease, or if the study would delay surgery; technical or human error; or patient withdrawal of audio recording consent. While slightly underpowered, study results did not signal that more audio recordings would yield statistically significant results. A final study limitation is our inability to control the effects of a patient's medical course on study outcomes that postsurgical (i.e., surgical course or change in prognosis) factors might contribute.
Conclusions
Study results support the feasibility and safety of preoperative ACP among surgical oncologic patients. While patients thought the ACP video was more helpful and it was associated with increased surgeon–patient ACP discussion, the ACP video did not substantially change patient–surgeon communication. Secondary outcomes also support worse mood symptoms among patients one week following cancer surgery and that nearly all patients pursued cancer surgery with cure-related goals. Future studies could increase ACP dose by modifying video content or frequency and/or how or who presents that content.
Footnotes
Acknowledgment
Research reported in this article was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (CD–12–11–4362). The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or Methodology Committee.
Author Disclosure Statement
No competing financial interests exist.