
Abstract
Abstract
Background:
To promote better care at the end stage of life in long-term care facilities, a culturally appropriate tool for identifying residents at the end of life is crucial.
Objective:
This study aimed to develop and validate a prognostic tool, the increased risk of death (IRD) scale, based on the minimum data set (MDS).
Design:
A retrospective study using data between 2005 and 2013 from six nursing homes in Hong Kong.
Setting/Subjects:
A total of 2380 individuals were randomly divided into two equal-sized subsamples: Sample 1 was used for the development of the IRD scale and Sample 2 for validation.
Measurements:
The measures were MDS 2.0 items and mortality data from the discharge tracking forms. The nine items in the IRD scale (decline in cognitive status, decline in activities of daily living, cancer, renal failure, congestive heart failure, emphysema/chronic obstructive pulmonary disease, edema, shortness of breath, and loss of weight), were selected based on bivariate Cox proportional hazards regression.
Results:
The IRD scale was a strong predictor of mortality in both Sample 1 (HRsample1 = 1.50, 95% confidence interval [CI]: 1.37–1.65) and Sample 2 (HRsample2 = 1.31, 1.19–1.43), after adjusting for covariates. Hazard ratios (HRs) for residents who had an IRD score of 3 or above for Sample 1 and Sample 2 were 3.32 (2.12–5.21) and 2.00 (1.30–3.09), respectively.
Conclusions:
The IRD scale is a promising tool for identifying nursing home residents at increased risk of death. We recommend the tool to be incorporated into the care protocol of long-term care facilities in Hong Kong.
Introduction
T
As defined by the World Health Organization, necessary means for preventing and relieving suffering of patients and their families include the early identification of palliative care patitents. 5 Hence, a tool for identifying individuals at the end of life functions as an important building block of a national/regional palliative care policy framework. As each region has its unique characteristics, the tool needs to be customized and locally verified to address the issues of cultural diversity in addition to regulatory and resource restraints.
In Hong Kong, ∼6.4% of older persons reside in long-term care facilities and, in 2012, deaths of residents in care homes accounted for 33.5% of all deaths.6–8 To enhance palliative care services in Hong Kong, substantial effort and resources need to be expended in long-term care settings.9,10 A scientifically validated tool that can efficiently identify long-term care residents who are at the end of life and may benefit from palliative care needs to be available.
The minimum data set (MDS) is a clinical assessment tool commonly used worldwide. 11 In Hong Kong, the Chinese version of MDS instruments has been validated and widely used in various care settings since 2000. 12 A prognostic tool based on readily available MDS items have the advantage of better integration into daily practice and not requiring additional resources. The MDS offers a comprehensive toolkit with a rich collection of summary scales serving various purposes. 13 Among these, three scales can be used for identifying residents who are in their final days of life, including the MDS-Changes in Health, End-stage disease, and Symptoms and Signs (CHESS) score, the MDS mortality rating index (MMRI), and the MMRI-R.14–16 The applicability of these tools in populations with different clinical and cultural characteristics remains unknown.
The CHESS score was developed in 2003 to identify individuals at risk of serious decline and has been shown to be a valid predictor of mortality in North America and Europe.14,17–21 However, a study in Hong Kong found that although the CHESS was an independent predictor of lower survival, its hazard ratio (HR) from the survival analysis was smaller than MDS activities of daily living (ADL) Self-Performance Hierarchy (ADLH) scale. 22 After critically reviewing the items in CHESS, we identified one potential contributing factor, the prognosis item “clinician ratings of a prognosis of less than six months.” In Chinese societies, death is a sensitive topic and public knowledge regarding palliative care issues is generally lacking. Discussion of death is considered taboo as it is believed that such talk may bring bad luck to the person and hasten his/her death. 23 These taboos may have unintentionally permeated into medical practice to an extent that health professionals are expected to tell a “white lie” by avoiding giving a poor prognosis. 23
The MMRI was proposed in 2005 by a team of palliative care researchers and was later simplified to a 12-item MMRI(-R) scale for use in clinical practice.15,16 However, the MMRI(-R) index adopts different scoring standards and includes items that are absent from the Hong Kong version of the MDS. These incompatibilities lead to difficulties in directly applying these scales to the local population.
The present study aimed to develop and validate a brief screening tool for identifying residents with increased risk of death, the IRD scale, by using local data from nursing homes in Hong Kong. Using the CHESS as a reference, we also wished to explore whether differences in culture and the health care system play a role in the applicability of clinical scales that originated in western societies. Residents who are identified as being at high risk of death can then be recommended to receive a more in-depth review such as the interRAI Palliative Care assessment. 24
Methods
Settings and participants
The present study is a retrospective study based on clinical records. Data were obtained from MDS 2.0 assessments of long-term care residents in six nursing homes in Hong Kong between 2005 and 2013. These nursing homes are funded by the Hong Kong government but managed by a nongovernmental organization. Only residents 65 years of age or older at the time of their first full assessment were included in this study. The assessments were performed annually by a multidisciplinary team, which included physical therapists, occupational therapists, social workers, nurses, and health workers who have received standardized training. Health worker, in this study, refers to any person holding a health worker certificate awarded by a training course approved by the Director of Social Welfare under the Residential Care Homes (Elderly Persons) Regulation. 25 Tracking forms were used to document mortality and discharge information. Ethical approval was obtained from the Review Board of the Human Research Ethics Committee for Nonclinical Faculties at the University of Hong Kong.
Measures
In the process of developing the original CHESS scale, the analysis began with “an examination of data on clinical indicators that suggested that the individual might be undergoing change in health status.” 14 Items from three domains were considered, including changes in health status, end-stage disease, and symptoms and signs of medical problems. Following this approach, we identified all possible MDS items from the three domains. Since retrospective data of this study were collected using MDS Version 2.0, whereas interRAI Long-Term Care Facilities Version 9.1 is likely to be adopted in the near future, we restricted our collection of items to those that are shared by both versions to ensure a smoother transition. 26
In the “changes in critical health status” domain, two items, changes in cognitive status and changes in ADL, were examined. Both items were coded as 0 = no change, 1 = improved, or 2 = deteriorated. Residents coded as 2 in the original item were coded as 1 point for this analysis, indicating worsening health, and those coded as 0 and 1 in the original item were coded as 0 points, indicating no worsening health. In the original CHESS study, end-stage disease is measured by a single item documenting whether the resident has a prognosis of having end-stage disease with six or fewer months to live. A preliminary analysis of our sample showed that fewer than 1% of residents had such a prognosis. This domain is then replaced by critical illnesses in which we examine the mortality risk of 11 major diseases with diagnosis records available in the MDS (Table 1 for diseases included). Measures of symptoms and signs of medical problems were 15 items covering health conditions and oral/nutritional status (also shown in Table 1). All 15 items were coded as 0 = absent and 1 = present.
Recurrent lung aspirations in the past 90 days.
Conditions/diseases causing unstable cognition, ADL, mood or behavior patterns.
Experiencing an acute episode or a flare-up of a recurrent or chronic problem.
End-stage disease with six or fewer months to live.
Weight loss of 5% or more in the past 30 days.
ADL, activities of daily living; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratios.
The survival time was measured as the number of days survived between the date entering the study (typically recorded as the date of the first MDS assessment) and date of death documented in the tracking form.
Control variables were gender, age, education level, cognitive performance, mood status, and functional activities. The four categories of education level were illiterate, less than primary school, primary school graduate, and higher than primary school. Cognitive performance was assessed by the MDS cognitive performance scale (CPS) scored from 0 (intact) to 6 (very severe impairment).27,28 Mood status was assessed by the MDS depression rating scale (DRS), with higher scores indicating a higher likelihood of depression. 29 ADL was measured by the MDS Activity of Daily Living Hierarchy scale scored from 0 to 6, with higher scores indicating greater dependence. 30
Data analyses
There were 2380 residents in the dataset. We randomly allocated half the residents into Sample 1 (n = 1190) used to develop the scale and half into Sample 2 (n = 1190) used to validate the scale. Demographic and clinical characteristics of the two groups were compared using independent sample t-tests for continuous variables, Chi-square tests for categorical variables, and independent sample Mann–Whitney U tests for ordinal variables.
For Sample 1, we used bivariate analyses to examine each item's predictive power for mortality using Cox proportional hazards regression. Items that achieved a HR greater than 1.5 and p-values less than 0.005 were kept for further analysis. A variety of configurations for the IRD scale were considered and compared. The resulting scale was formed according to the parsimonious principle. The IRD scale's distribution and predictive power for mortality were compared using the CHESS scale as a reference. Multivariate Cox proportional hazards model were used to examine the performance of the IRD scale, adjusting for demographic characteristics, cognitive performance, mood status, and ADL. We used the listwise deletion technique to handle missing data, which only accounted for less than 1% (n = 23) of the total sample. All analyses were conducted using Stata 13.1 software. 31
Results
Sample characteristics
A total of 1066 residents entered the study in 2005. In subsequent years, on average, a further 164 (standard deviation [SD] = 15.14) elderly residents moved into care facilities annually. Within the study period, 1317 residents (55.34%) died and 163 (6.85%) moved out of the care homes. Excluding residents who moved into facilities for less than one year (n = 232), 1826 out of 2147 participants lived longer than one year (85.05%), 132 died between 7 and 12 months (6.15%), and 189 died within 6 months (8.80%).
At baseline, the average age of the sample was 82.8 (SD = 8.1) years, with the oldest resident being 112 years old. Female residents accounted for 67.6% of the total sample. Approximately half of the sample (47.0%) did not receive any formal education. The mean CPS, DRS, and ADL scores were 2.4 (SD = 2.1), 0.3 (SD = 0.8), and 0.6 (SD = 0.5), respectively. The demographic and clinical characteristics of Sample 1 and Sample 2 are summarized in Table 2.
Depression rating scale.
Wilcoxon rank-sum (Mann–Whitney) test.
Activities of daily living.
Cognitive performance scale.
The MDS-CHESS score.
CHESS, changes in health, end-stage disease and symptoms and signs; CPS, cognitive performance scale; DRS, depression rating scale; MDS, minimum data set; SD, standard deviation.
Development of the IRD scale
The distribution of candidate items and their respective HRs calculated from bivariate proportional hazards model are summarized in Table 1. We found that declines in both cognitive status and ADL were associated with more than 50% higher mortality risk. Renal failure had the highest HR (HR = 2.55; 95% confidence interval [CI]: 1.61–4.03) among the 11 critical illnesses. Cancer, congestive heart failure, emphysema/COPD, shortness of breath, weight loss, and edema also had highly significant HRs in excess of 1.5. The IRD score was formed by summarizing the scores of these nine items. The unadjusted HR of IRD in Sample 1 was 1.54 (1.41–1.69) (Table 3). The HR after controlling for covariates was 1.50 (1.37–1.65) (Table 4). The Kaplan–Meier survival curves for IRD scores in Sample 1 after controlling for covariates are shown in Figure 1.
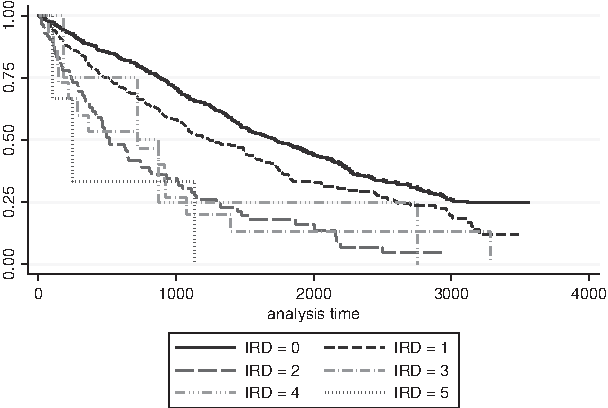
The Kaplan–Meier survival curves for IRD scores in Sample 1, controlling for covariates. IRD, increased risk of death.
Estimated from multivariate Cox proportional hazards model without adjustment of covariates.
Increased risk of death (IRD) scale.
The MDS-CHESS score.
Estimated from multivariate Cox proportional hazards model with or without adjustment of demographic characteristics, cognitive performance, depressive symptoms, and functioning status.
Increased risk of death scale.
The MDS-CHESS score.
Depression rating scale.
Activities of daily living.
Cognitive performance scale.
We tested the effect of different cutoff points by examining the corresponding HRs associated with different risk levels of death. Because 90.9% of residents had IRD scores of 0 or 1, we examined cutoff values of 2 and 3, which resulted in 9.1% and 1.9% of residents classified as at high risk of death, respectively. After conducting the sensitivity analysis, residents with an IRD score greater than or equal to 3 were classified as at high risk of death. This small group of individuals had a median survival of 289 days and 3.3 times higher mortality risk compared with individuals in the robust group. The results from the multivariate proportional hazards model for raw scores of IRD, CHESS, and categorized IRD levels, as defined by different cutoff values in Sample 1, are summarized in Table 4.
The final version of the IRD scale
To summarize, the IRD scale is a nine-item scale formed by summarizing the scores on (1) decline in cognitive status, (2) decline in ADL, (3) cancer, (4) renal failure, (5) congestive heart failure, (6) emphysema/COPD, (7) edema, (8) shortness of breath, and (9) weight loss, ranging from 0 (no instability) to 9 (very high health instability). The raw score is then categorized into three levels: 0 = robust, 1 or 2 = at moderate risk of death, and 3 or more = at high risk of death.
The correlations between IRD and CPS, DRS, and ADL as measured by Spearman rank-order correlation were −0.05 (p = 0.066), 0.03 (p = 0.297), and 0.09 (p = 0.001), respectively. The low degree of association among covariates indicated that the measure of palliative care needs addressed different domains from that of other primary MDS scales.
Validation of the IRD scale
Sample 2 was used to validate the IRD score for predicting mortality. The estimates from the regression models for the IRD and CHESS raw scores, as well as the three levels of risk of death classified using both IRD and CHESS are shown in Table 5. The Kaplan–Meier survival curves for IRD scores in Sample 2 after adjusting for covariates are shown in Figure 2. After controlling for covariates, the IRD raw score was associated with a 31% higher risk of mortality per one point increase, indicating much greater predictive power than the other scales. Residents who were classified as having moderate and high risk of death had HRs of 1.52 (1.28–1.80) and 2.00 (1.30–3.09), respectively. The HR associated with a one point increase in the CHESS score was not significant in Sample 2.
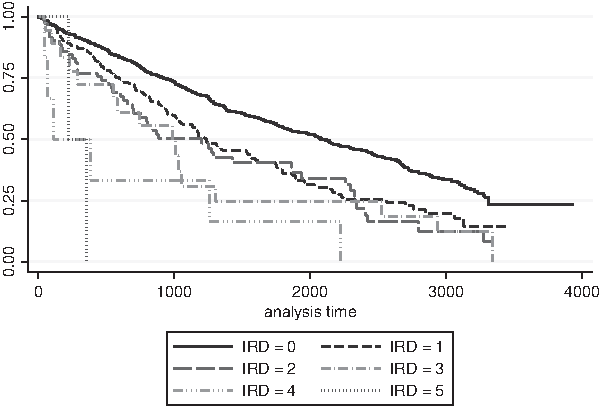
The Kaplan–Meier survival curves for IRD scores in Sample 2, controlling for covariates.
Estimated from multivariate Cox proportional hazards model with or without adjustment of demographic characteristics, cognitive performance, depressive symptoms, and functioning status.
Increased risk of death scale.
The MDS-CHESS score.
Depression rating scale.
Activities of daily living.
Cognitive performance scale.
Discussion
In this study, we developed and validated a prognostic tool to assess the risk level of death for residents in long-term care settings in Hong Kong based on nine MDS items. Results showed that the IRD scale was a reliable tool for identifying residents with increased risk of death and who could, therefore, benefit from end-of-life care.
Residents in long-term care facilities deserve high-quality palliative care. Without timely identification of residents who are already at the end of life, residents would experience frequent hospitalization, unnecessary medical treatment, and potential distress associated with unfinished business. 32 Screening tools, developed in a Western context that emphasize the gold standard “surprise question” to predict six-month mortality, appear to be less effective and sensitive among Chinese populations such as in Hong Kong. As seen in our sample, only 0.08% of residents had a prognosis of less than six months to live as certified by a physician. The IRD scale appeared to be a culturally sensitive and feasible alternative.
The CHESS scale has not been thoroughly validated in a Chinese context. Unlike other scales that have been designed using relatively culture-neutral items, the prognosis item in CHESS relies on the physicians' judgment. Well-documented disease diagnosis and deteriorating clinical course are required to substantiate this judgment. 33 Alternatively, one might argue that although there are visiting physicians for all the subvented nursing homes in Hong Kong, they are not involved in conducting MDS assessments. There is potentially a mismatch between physician's clinical records and the MDS assessment.
We conducted this study to tackle the question of whether cultural differences in norms and attitudes toward death and dying could affect the applicability of clinical measures that were developed and validated in western societies. Our findings showed differences in some indicators compared with previous western studies. CHESS scores of 3 or more were reported in 6% to 13% of residents in Canadian nursing homes21,34–37 compared with 1% in our sample. Several factors may be attributable to this nonignorable discrepancy. First, in the Canadian sample, about 13% of patients were rated as having end-stage disease, whereas in our sample this rate was less than 1%. 14 Second, our study sample might be from a population requiring less intense care compared with the Canadian nursing home population. Finally, this may have uncovered a general problem of coding practice that leads to the underdetection of issues like dehydration. Further investigations are needed to examine these hypotheses.
Findings from this study suggest that the cancer item is a good predictor of mortality. However, no consensus was reached on whether cancer can be viewed as a sensitive predictor. 38 Although in some previous studies, cancer has been shown to be related to the mortality of nursing home residents, some recent research also found that survival did not differ between residents with or without cancer.16,39–41 In Hong Kong, participation rates in cancer screening programs have remained low.42,43 Cancer remains the leading cause of death in Hong Kong accounting for 31% of all deaths in 2015. 44 It should be noted that this result was generated during a specific stage in the development of the medical system in Hong Kong, hence, it may need further revision as the system progresses.
There were some limitations in the current study that should be considered when interpreting the findings. Although our study included 2380 residents, the sample was substantially smaller than the sample sizes used to develop the CHESS and MMRI scales in North America. Given the reported low rates of various indicators, it is possible that this study was underpowered to fully test the hypotheses within Chinese care settings. Because the sample was obtained from six nursing homes, any direct generalization to other care settings in Hong Kong or in other Chinese populations should be made with caution.
Conclusions
The IRD scale has been shown to be a promising prognostic tool for identifying residents with increased risk of death in Hong Kong and is potentially useful for other Chinese societies. It is worth noting that the IRD scale should not be used to make final judgments on the eligibility of access to end-of-life care or to predict life expectancy. Rather, it should be viewed as a preliminary screening tool for identifying individuals who may benefit from palliative care. The final decisions should be made based on comprehensive assessments and the judgment of health professionals. More research is needed regarding the organization and implementation of the IRD scale as a preliminary screening tool, the choice or design of the follow-up assessments for service matching, and possible interventions.
Footnotes
Acknowledgment
The authors would like to thank colleagues from Hong Kong Sheng Kung Hui Welfare Council. Without their help and support, this study could not have been carried out successfully.
Author Disclosure Statement
No competing financial interests exist.