
Abstract
Abstract
Background:
Self-care systems for early-stage specialist palliative care for cancer patients and their family caregivers have received much attention recently. Resonant breathing is an established method for maximizing heart rate variability (HRV), but it has not been implemented for home self-care.
Objective:
We aimed to examine the usefulness and ease of implementation for family caregivers to administer resonant breathing using a portable device at home.
Design:
We divided caregivers into two groups—a home self-care group and a control group—and we conducted a randomized open-label study, with rate of change in HRV being the primary outcome.
Setting/Subjects:
We administered HRV biofeedback (HRV-BF) using resonant breathing to 54 family caregivers who felt burdened by their nursing care responsibilities.
Results:
Among the self-care group, 92.6% of participants completed the study in their homes; 28 days after intervention initiation, the resonant breathing implementation rate at home was 86.1%. There was an interaction between time course and grouping in our HRV comparisons: the change rate in the home self-care group was higher during HRV-BF than before HRV-BF.
Conclusions:
Because family caregivers in our study learned to quickly administer resonant breathing using a portable device at home, resonant breathing improved rapidly, along with autonomic nerve function and quality of life.
Introduction
B
One study introduced mindfulness-based stress reduction (MBSR) to lung-cancer patients and their family caregivers. 7 They reported that, although psychological distress was alleviated among the patients using MBSR, distress among family caregivers did not improve because caregivers prioritized patients' well-being over their own. 7 Other studies have concluded that caregivers have low motivation to perform self-care because they often experience guilty feelings about caring for themselves.8,9 However, the home is the center of life for not only patients but also their family caregivers; thus, it should be easier for caregivers to balance self-care, including relaxation techniques, with maintaining their patient's well-being at home than at a medical facility. To foster this, a medical system is needed that focuses on mind and body care for caregivers that can be used at home and that can be learned quickly.
Biofeedback (BF) therapy is a method for regulating mind and body by measuring the physiological information that people are normally unaware of and visually feeding back the information to create greater self-awareness and to foster better self-care. A protocol of heart rate variability biofeedback (HRV-BF) using resonant breathing was established 10 and is useful for people with hyperactive autonomic nerve function, mood disorders, or psychosomatic diseases.11,12 HRV measures the fluctuation in the interval between heartbeats and reflects autonomic nerve activity. A low frequency (LF; 0.04–0.15 Hz) component and high frequency (HF; 0.15–0.4 Hz) component are recorded within several minutes of HRV. 13 These components are obtained by frequency domain analysis and reflect parasympathetic activity.
Resonant breathing is a method of breathing to achieve a frequency that maximizes HRV. Resonant breathing gives rise to a resonance between breathing and the baroreceptor reflex involving the LF power of HRV, to increase HRV. 10 In fact, a study reported that resonant breathing enhanced baroreflex sensitivity in patients with chronic heart failure. 14 To learn how to breathe at an appropriate resonant breathing frequency, monitoring at a medical institution is required. 10 Resonant breathing frequency varies from five to seven times per minute depending on individual characteristics (sex and height). 15 Resonant breathing involves taking slow measured breaths in and out. Typically, the in-breath lasts about three seconds, the pause-breath lasts about one second, and the out-breath lasts about six seconds. Individuals who practice resonant breathing report that it helps them relax and gives them a sense of calm.
Because of developments in information and communication technologies, it is possible to administer self-care using a portable breathing training guide at home, where the appropriate resonant breathing frequency is set in the guide; however, such a self-care system has not yet been established, and there have been no studies evaluating its implementation or usefulness. We hypothesized that resonant breathing using a portable device at home can increase family caregivers' motivation to perform self-care. To test this hypothesis, we estimated the implementation rate of resonant breathing for self-care among at-home caregivers, and we assessed its effect on autonomic nerve function and QOL.
Methods
Study participants and eligibility criteria
We administered HRV-BF with resonant breathing to the family caregivers of advanced-cancer patients. At-home caregivers can feel burdened after long-term administration of nursing care. In this study, we defined a family caregiver as a family member who directly provided care to a relative with cancer, including spouses. The level of nursing-care burden felt by the caregiver was evaluated using the Japanese version of the Zarit Caregiver Burden Interview (J-ZBI). Participants with a J-ZBI score ≥24, which is the cutoff value for depression risk, were eligible for this study. 16 Participants were excluded from the study if they: (1) had diseases that affect evaluation of autonomic nerve function, such as diabetes; or (2) had cognitive impairments that made communication difficult.
This study was conducted from 2015 to 2017 at the Kansai Medical University Hospital. During this period, 182 family caregivers of advanced-cancer patients who visited the palliative care department were continuously enrolled in this study. Of the 182 caregivers, 69 satisfied the eligibility criteria according to their J-ZBI score and 4 satisfied the exclusion criteria. We obtained participation consent from 54 family caregivers out of 65, and all 54 were included in the study.
Study design
We conducted a randomized, open-label comparison study between two groups. One group of caregivers performed resonant breathing using a portable breathing training guide device at home (home self-care group). Another group of caregivers did not perform any self-care at home (control group). Figure 1 shows the study flow chart.
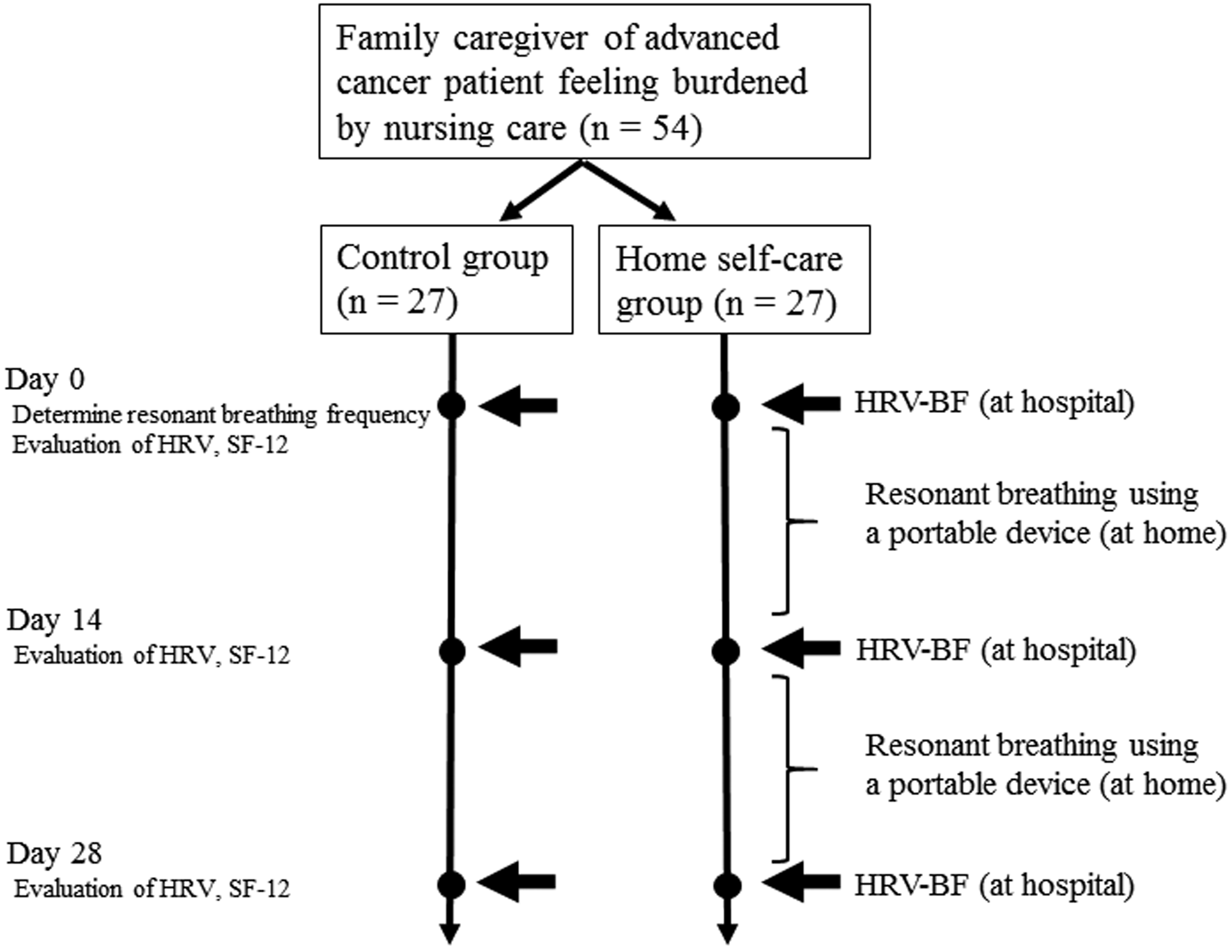
Study flowchart. BF, biofeedback; HRV, heart rate variability; SF-12, 12-item short-form health survey.
At the start of the intervention (day 0), we monitored breathing among participants in both groups at our hospital, using a multichannel BF system (ProComp Infiniti™/BioGraph Infiniti; Thought Technology Ltd., New York), to determine the resonant breathing frequency of caregivers in both groups. Participants breathed for two minutes at 5, 5.5, 6, 6.5, and 7 breaths per minute while we measured breathing frequency and heart rate. We calculated the resonant breathing frequency as the number of breaths that maximized the LF and low-frequency spectrum peak.
HRV-BF using resonant breathing was administered to caregivers in both groups at our medical institution for up to 30 minutes (on days 0, 14, and 28 from the start of the intervention period). During HRV-BF, caregivers used the Breath Pacer application (ProComp Infiniti/BioGraph Infiniti; Thought Technology Ltd.) to maximize the HRV waveform displayed on their tablet's monitor screen. We connected the HRV components (myBeat WHS-2; Union Tool Co., Tokyo, Japan) to a special electrode pad attached directly to the participant's chest. The HRV waveform was thus displayed on the monitor screen in real time.
We measured HRV among all family caregivers before administering HRV-BF. Caregivers in both groups performed resonant breathing for five minutes and then rested for five minutes before and after resonant breathing. We measured the LF and HF power of HRV continuously for 15 minutes; we recorded these measurements on days 0, 14, and 28. We used a HRV analysis software (Kubios HRV version 3.1; Kubios Oy, Kuopio, Finland) that is considered highly reliable for short-term recording.17,18 The primary outcome of this study was the change in HRV 28 days after day 0, based on a comparison between the home self-care group and the control group. Furthermore, we evaluated the health-related QOL of family caregivers using the 12-Item Short-Form Health Survey (SF-12), which is a self-report questionnaire that we administered on days 0, 14, and 28.
We instructed caregivers in the home self-care group to perform resonant breathing every day for up to 20 minutes (or a minimum of 5 minutes) before going to bed, according to the pace set by their portable device (iPad mini; Apple, Cupertino, CA) and the Breath Pacer application. We downloaded Breath Pacer, a breath self-training guide, onto the tablet for the caregivers to use (Fig. 2). Data entry on Breath Pacer was carried out based on frequency, once the user's resonant breathing frequency had been determined. Caregivers in the control group did not perform any special techniques, such as resonant breathing, at home.
Breath pacer.
Measurements
Resonant breathing implementation rate at home
We calculated this rate by dividing the number of days in which at-home family caregivers in the self-care group performed resonant breathing at home over the intervention period (28 days). Each day, the caregiver performed resonant breathing at home according to the Breath Pacer application for at least five minutes before going to bed.
12-item short-form health survey
The SF-12 is a health-related QOL scale, which is not limited to assessment of patients with specific diseases. Its reliability and validity have been established. 19 We obtained three summary scores: a physical component summary (PCS), a mental component summary (MCS), and a role/social component summary (RCS) from participants' responses to the 12 questions. Based on national standard values, we translated each summary score into a rating score (0–100 points). We determined participants' health-related QOL by comparing their score with the national standard value (national standard value = 50 points; standard deviation = 10 points).
Heart rate variability
We estimated the standard deviation of the normal-to-normal interval (SDNN) in addition to LF and HF. The SDNN is the standard deviation of the R-R intervals in an electrocardiogram and is obtained through time domain analysis. The SDNN is used to measure cardiovascular compatibility. A decrease in SDNN indicates a decrease in parasympathetic activity. The mean values for resting HRV in adults are HF = 657 ms 2 , LF = 519 ms 2 , and SDNN = 50 ms. 20
Statistical analyses
All data are reported as means with standard deviations, 95% confidence intervals, ranges, or frequencies (%), as appropriate. We used an unpaired t test for the dependent variables: age, sex, resonant frequency, SF-12 score, and HRV score. When a participant withdrew from the study, we used their SF-12 score and HRV score that was most recently submitted before withdrawal. We analyzed the change in SF-12 and HRV scores using one-way repeated measures analysis of variance (ANOVA) for each group. For comparisons between groups, we used time course as the within-participant factor and grouping as the between-participant factor in two-way repeated measures ANOVA.
A p-value <0.05 was considered statistically significant. Statistical analyses were conducted using SPSS version 18.0J for Macintosh (SPSS, Inc., Chicago, IL).
Results
Table 1 shows the demographics and clinical characteristics of both study groups. One family caregiver in each group withdrew from the study during days 14–28 (92.6% completion rate) because their patients experienced a decline in physical condition. In the home self-care group, the implementation rate of resonant breathing was 86.1%. The number of implementation days was 24.1 (SD 4.8), with 12.4 days (SD 2.1) and 11.7 days (SD 3.4) during days 0–13 and 14–28, respectively.
Comparison of Clinical Characteristics between the Home Self-Care and Control Groups
BF, biofeedback; HRV, heart rate variability; J-ZBI, Japanese version of Zarit Caregiver Burden Interview; LF, low frequency; MCS, mental component summary; PCS, physical component summary; RCS, role/social component summary; SD, standard deviation; SF-12, 12-item short-form health survey.
There was a significant interaction between time course and grouping (p = 0.021) in LF between the study groups. There was also a significant difference in time course between the groups (day 0, p = 0.322; day 14, p = 0.107; day 28, p = 0.004; Fig. 3). Even when we compared SDNN between the groups, there was significant interaction between time course and grouping (p = 0.022), and there was a significant difference in time course between the groups (day 0, p = 0.646; day 14, p = 0.004; day 28, p = 0.004) (Fig. 3). We found no significant difference in HF change between the two groups, indicating that there was no interaction between time course and grouping (p = 0.974). When we compared LF before and during resonant breathing, we found no interaction between time for HRV-BF and grouping on day 14 (p = 0.304). For grouping, we found a main effect among the home self-care group (p = 0.040; Fig. 4). When we compared the groups on day 28, we found a significant interaction between time course and grouping (p = 0.042), and the LF change rate among the home self-care group was higher than in the control group.

Change in HRV before resonant breathing. HF, high frequency; LF, low frequency; n.s., not significant; SDNN, standard deviation of the normal-to-normal interval.
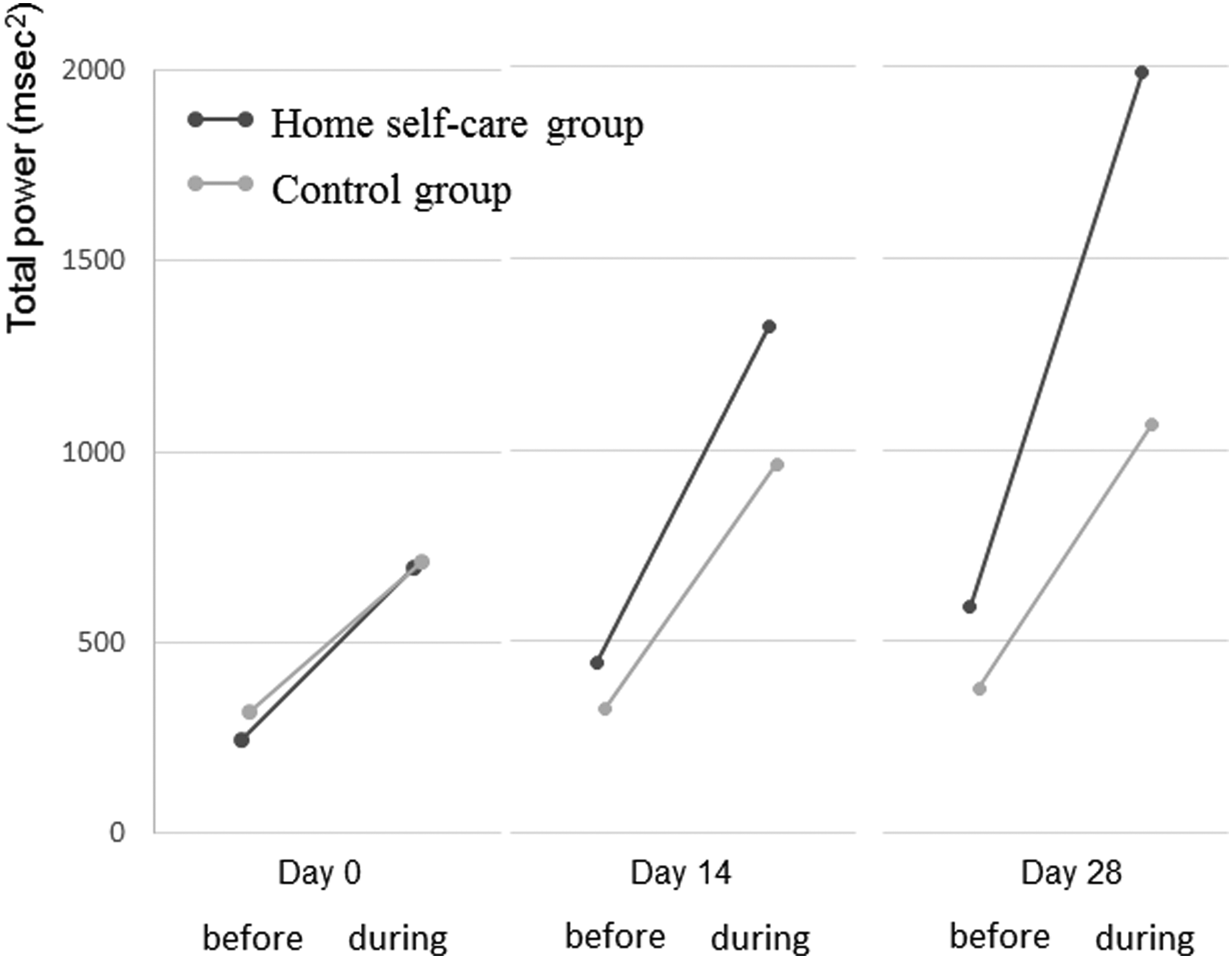
Change in the low-frequency power of HRV before and during resonant breathing.
Scores for the PCS and MCS of health-related QOL scores among the home self-care group were significantly higher on days 14 and 28 compared with day 0 (Fig. 5). PCS scores of caregivers in the control group increased over time, but not significantly. MCS scores increased over time, and the difference between days 28 and 0 was significant. Regarding RCS, we observed no significant change in either group. In a comparison between the groups, there was no significant interaction in time course and grouping among any of the three scales (PCS, p = 0.804; MCS, p = 0.183; RCS: p = 0.960).
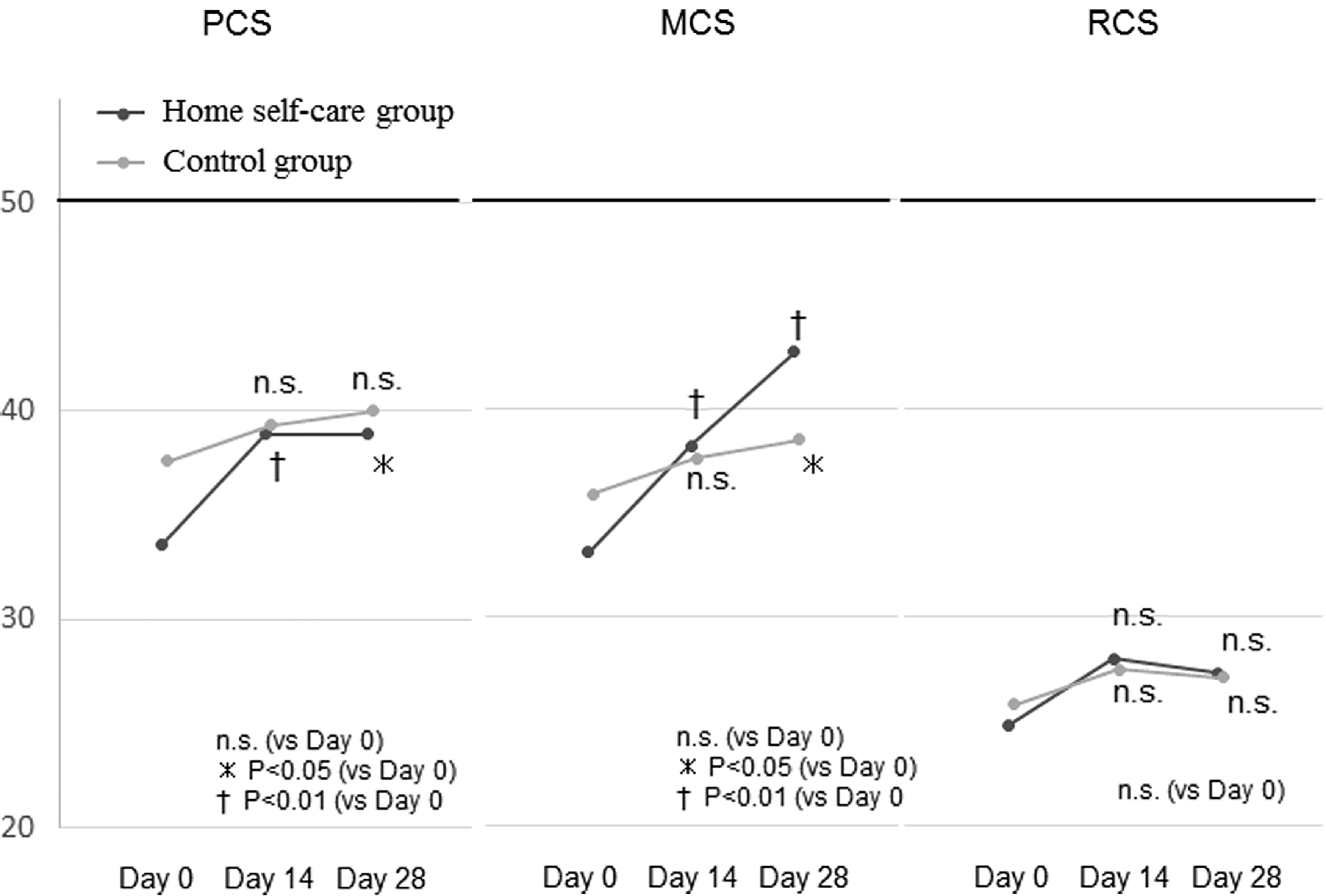
Change in 12-item short-form health survey values. MCS, mental component summary; PCS, physical component summary; RCS, role/social component summary.
Discussion
To the best of our knowledge, this is the first study to evaluate a self-care system for family caregivers of cancer patients using resonant breathing and a portable device at home.
Implementation of resonant breathing with a portable at-home device was successful. The completion rate, 92.6%, was the same among the home self-care group and the control group. The implementation rate of resonant breathing in the home self-care group was high, at 86.8%. There are no previous reports on self-care among at-home family caregivers of cancer patients; thus, we were unable to compare resonant breathing implementation in our study with other studies. There are only two reports investigating the use of resonant breathing with an at-home portable device. In one report, five healthy individuals performed resonant breathing for four days. In the other, an insomnia patient performed resonant breathing for seven days.21,22 We monitored our participants for 28 days, which is a relatively long study period. Interestingly, the implementation rate of resonant breathing during days 14–28 was nearly the same as that during days 0–14. Previous research suggests that longer implementation leads to better outcomes. For example, one study suggested a link between the implementation rate and motivation to perform self-care among patients with type-2 diabetes. 23 Another study pointed to an association between decreased implementation rates for self-care and distress among family caregivers. 24
We offer three explanations for the high implementation rate of self-care by family caregivers in our study. First, the device may have improved motivation to perform resonant breathing. A previous study reported that use of wearable devices at home, such as activity trackers, improved motivation to remain active among breast cancer survivors. 25 Second, the caregivers in our study may have been aware of the effect of resonant breathing when accurately performed. In a subjective evaluation, scores for health-related QOL among caregivers in the home self-care group were significantly higher than among controls, indicating that these caregivers experienced an effect of home self-care. Third, the device may have been easy to operate. Because the average age of participants in this study was 63 years old, these relatively younger adults were skilled at using such devices.
Resonant breathing using an at-home portable device could improve autonomic nerve function and QOL among caregivers in the home self-care group over a shorter period than among participants in the control group. In this study, the LF and SDNN values of HRV on day 28 were significantly different between the two groups. In addition, there was no significant difference in the day-14 values between the groups. Although the HRV in the control group did not change over time, that of the home self-care group increased greatly. A previous study that evaluated the usefulness of HRV-BF performed their first evaluation four weeks after study initiation.10,11,26 They may have assumed that a two-week study period was too short to assess HRV-BF administered at a medical institution. In many cases, caregivers' distress increases with progression of their patients' advanced-stage cancer. Thus, an intervention method that can yield early improvements in a short time frame would be valuable. 27 We also found that HRV and SF-12 values were lower than the basic data and national standard values,19,20 and it is important that caregivers with severe distress improve their HRV and SF-12 scores in a short time frame.
We compared the LF of HRV before and during HRV-BF; the LF change rate on day 28 among the home self-care group was higher than in the control group. This suggests that caregivers quickly learned resonant breathing at home. Furthermore, the LF and SDNN values of HRV in the intervention group increased significantly over time, indicating that practicing resonant breathing at home has a sustained, rather than transient, effect. Because resonant breathing efficiently stimulates the baroreceptor reflex, continual practice may enhance autonomous homeostasis functions. 9
This study has some limitations. First, we were unable to conduct long-term evaluations. Another study with a two-year follow-up period that used a wearable activity-tracking device showed that self-care in the intervention group was not sufficiently different from self-care in the control group that did not use a device because intervention participants found the devices uncomfortable to wear. 28 Second, although we demonstrated benefits of resonant breathing at home, we were unable to fully evaluate the effect of using a portable device to prompt resonant breathing practice.
Conclusion
Family caregivers in this study were able to quickly learn resonant breathing using a portable device at home, and our findings show that their autonomic nerve function and QOL improved rapidly. Our results also show that caregivers were able to maintain resonant breathing as an at-home self-care system, especially when performed with cooperation from their medical institution. Based on these findings, healthcare providers should consider recommending resonant breathing to caregivers of seriously ill patients as a feasibly easy-to-implement strategy.
Footnotes
Acknowledgments
The authors thank Analisa Avila, ELS, of Edanz Group (![]() ) for editing a draft of this article. Ashley Hazel, PhD, of Edanz Group (www.edanzediting.com/ac) edited a second draft of this article.
) for editing a draft of this article. Ashley Hazel, PhD, of Edanz Group (www.edanzediting.com/ac) edited a second draft of this article.
Author Disclosure Statement
This work was supported by the following grant: Yuumi Memorial Foundation for Home Health Care.
No competing financial interests exist.