
Abstract
Abstract
Background:
Internationally, use of lidocaine infusions to treat cancer pain varies by center. Existing systematic reviews do not adequately inform use of lidocaine in cancer pain.
Objective:
To assess the effects of systemic sodium channel blockers on cancer pain in adults, review the dose protocols for administration, and assess toxicity.
Design:
Databases CENTRAL, MEDLINE, Embase, LILACS, CareSearch, and OpenGrey were searched from inception to 2016. Conference abstracts and reference lists were handsearched, and the lead investigators of included trials and Australian manufacturers were contacted. Included studies were randomized controlled trials evaluating one or more of lidocaine via intravenous or subcutaneous route, or mexiletine, flecainide, or tocainide via oral route; delivered at a site distant to the pain locus. The methodological quality of studies was assessed using the “risk of bias” domain-based evaluation by Jadad. Protocol is available on PROSPERO:CRD42016047092.
Results:
One positive (n = 50) and three negative (n = 10 each) crossover trials evaluated lidocaine versus placebo, and one trial (n = 16) compared lidocaine with dexmedetomidine. Meta-analysis of pooled data in 60 patients demonstrated a significant benefit of lidocaine infusion of 4–5 mg/kg over 30–80 minutes compared with placebo for >50% reduction in cancer pain. Secondary outcomes did not show a significant difference.
Discussion:
Based on the current available evidence, lidocaine infusion could be considered in refractory cancer pain where agents with level 1 evidence are ineffective. Further research is necessary to understand the protocol and population in which lidocaine may improve cancer pain and capitalize on the promising opportunities identified.
Background
Internationally, use of lidocaine infusions to treat cancer pain differs by center.1,2 There is a wide variation in recommendation for use. The European Society of Medical Oncology Clinical Practice Guidelines 3 and UpToDate, 4 a clinical decision support resource, 5 identify a role for systemic lidocaine to treat cancer pain in selected patients. The National Comprehensive Cancer Network and Australian Cancer Pain guidelines recommend against the use or make no mention.6,7
Existing systematic reviews do not adequately inform use of lidocaine or other sodium channel blockers in cancer pain. Reviews published in 2005 and 1998 on systemic local anesthetic agents in neuropathic and chronic pain, respectively,8,9 concluded there was little or no evidence in cancer pain. Since then, a large positive pilot study 10 of 50 participants has been published. A review of lidocaine in older adults 11 suggested possible benefit for lidocaine infusion, but excluded the three studies contributing to the recommendations in neuropathic and chronic pain.8,9 This systematic review provides an updated summary and analysis of the literature informing use of lidocaine infusions to treat cancer pain.
Improving evidence-based practice in cancer pain is crucial. More than 14 million people develop cancer worldwide each year, with at least two-thirds of those who have advanced cancer experiencing pain.12–14 Despite significant advances, cancer pain remains poorly controlled. The European Pain in Cancer survey found 58% of patients receiving prescription medicine reported inadequate pain relief at least several times a week. 15 A high proportion of patients are not responsive to opioids and require adjuvant analgesics. 16 It is also becoming increasingly recognized that opioid use has limitations particularly as cancer pain becomes more prevalent and more chronic. 17 The most common adjuvant therapies are anticonvulsants and antidepressants, however, the evidence for their efficacy in cancer pain is variable and in many patients not tolerated due to toxicity. 18
Lidocaine is a unique agent that has demonstrated level 1 benefit in nonmalignant pain.8,9 It offers a different toxicity profile to that of opioid analgesics and other adjuvant therapies, is one of the few adjuvant analgesics that can be given parenterally, and is thought to act via different mechanisms to other analgesics, all features that are desirable in some clinical situations.
Objective
The objective was to assess the effects of systemic sodium channel blockers on cancer pain in adults, review the dose protocols for administration, and assess toxicity.
This review included lidocaine, mexiletine, tocainide, and flecainide, however, only studies on lidocaine met the inclusion criteria.
Design
Protocol
This report was completed according to PRISMA guidelines. The full protocol is available from trial registry PROSPERO. 19
Data sources
Eligibility criteria
Randomized controlled studies, including crossover studies, were included for narrative review and meta-analysis. Observational studies, case reports, and case series were excluded. Eligible studies included participants older than 18 years, with a portion of participants having pain from cancer. Studies investigating perioperative and periprocedural pain were excluded, where lidocaine infusion was given only during or immediately after the procedure. Studies considered one or more of lidocaine via intravenous or subcutaneous route, or mexiletine, flecainide, or tocainide via oral route; delivered at a site distant to the pain locus. All comparators, including placebo and active control, were considered. Studies considering regional nerve blockade, topical, tumescent, epidural, and intrathecal administration of lidocaine were excluded. Outcome measures were chosen to reflect guidelines from the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials on reporting chronic pain trials, which recommend that a range of standardized outcomes be included. 20 No similar guidelines exist for cancer pain. The primary outcome measure was substantial benefit (defined as at least 50% pain reduction). Secondary outcomes were moderate benefit (at least 30% pain reduction), 20 mild pain postinfusion (<30/100 mm on VAS), 21 mean change in pain score, patient global impression, quality of life, adverse event withdrawal, and serious adverse events.
Information sources and search strategy
Four electronic databases were searched. The Cochrane Central Register of Controlled Trials (on September 5, 2016), MEDLINE (1946 to September 5, 2016), Embase (1974 to September 2, 2016), LILACS (1982 to September 5, 2016). Gray literature was searched through CareSearch and OpenGrey on September 5, 2016. EAPC congress abstracts from 1990 to 2016 were handsearched. The reference lists of all eligible trials, key textbooks, and previous systematic reviews were searched for additional studies. The lead authors of all included trials were contacted for further information and any unpublished studies. The Australian manufacturer of each intervention was contacted for any unpublished trials. The MEDLINE search strategy is outlined in Table 1 and the authors can be contacted for the full search strategy.
MEDLINE Search Strategy
Data extraction
One author (J.T.L.) ran the electronic database and other searches and excluded duplicates. Two authors (J.T.L., M.A. or C.R.S.) screened results and read the full article of potentially eligible studies to assess for inclusion. Two authors (J.T.L., M.A. or C.R.S.) independently assessed study quality and extracted data using a standard form. Missing data were sought from the lead author. Studies not published in English were evaluated by contacting the lead author or translation of the methods and results sections. Disagreements were resolved by discussion and consultation with a third author.
Data items
The data items about the study collected were eligibility criteria, study design, number and gender of participants, age, setting (inpatient or outpatient), country, diagnostic criteria, study arms, and outcomes. The results collected included the number of participants in each arm, number of missing participants, change in pain score, duration of relief, adverse effects, and whether they were prospectively sought. Where there was more than one time point, the pain scores immediately before and after the infusions were used.
Risk of bias in individual studies
Methodological quality of studies was assessed using the “risk of bias” domain-based evaluation by Jadad. 22 Selection bias, including random sequence generation and allocation concealment, performance bias, detection bias, attrition bias, reporting bias, and risk of carryover were assessed. Each domain was judged low risk, high risk, or unclear risk, with appropriate supporting quotes.
Synthesis of result plan
The primary outcome measure was the relative benefit (risk ratio) with 95% confidence interval of treatment compared with placebo to achieve substantial benefit (at least 50% pain reduction).
Secondary outcomes were based on recommendations in chronic pain studies. 20 Dichotomous data were used to calculate relative benefit (risk ratio) with 95% confidence interval of treatment compared with placebo. This was done for moderate benefit (at least 30% pain reduction) and “mild postinfusion pain” (<30/100 mm on VAS). Continuous data were used to determine the difference in postinfusion pain score between treatment and placebo groups. Data reported as a visual analog scale were converted to a numeric rating scale from 0 to 10, as these have been shown to correlate closely. 23 Crossover trials were treated as though they were parallel groups. Missing standard deviations were imputed by calculating the correlation coefficient of other studies.24,25 Individual patient data available in table and graph form were extracted and analyzed. The I2 statistic was used to quantify heterogeneity. 26 This describes the percentage of variability in effect estimates that is due to heterogeneity rather than sampling error.
Risk of bias across studies and additional analyses
A funnel plot was graphed to assess the risk of publication bias. Sensitivity analysis was performed to consider the effect of choices made in statistical analysis.
Data analysis
RevMan 5.3 software was used for statistical analysis.
Results
Study selection
The PRISMA diagram (Fig. 1) summarizes the study selection process. One study was evaluated by contacting the lead author and the methods and results of six studies were translated to English. One letter 27 described two studies, both excluded. One randomized controlled trial,28,29 which was reported twice, was excluded due to high risk of bias. Another randomized controlled trial published as a conference abstract 30 was excluded due to insufficient information despite efforts to contact the authors.
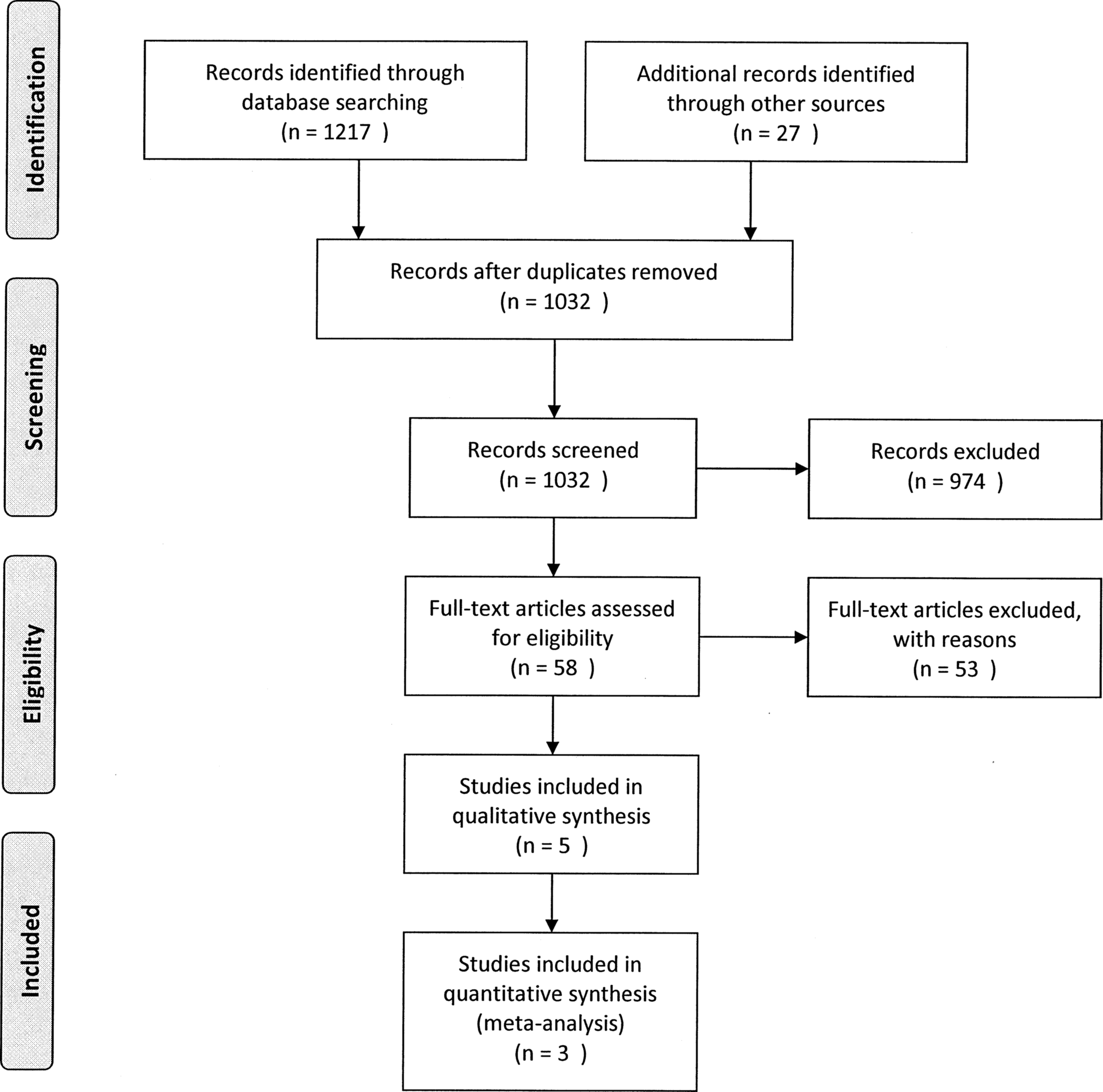
PRISMA evaluable flow diagram.
Study characteristics
The five randomized controlled trials found were of intravenous lidocaine and are described in Table 2.10,31–34 Four were crossover trials of intravenous lidocaine compared with placebo. The fifth trial 34 compared intravenous lidocaine infusion with dexmedetomidine infusion in palliative care patients with neuropathic pain refractory to opioids. A total of 80 participants were included in the placebo comparator and 16 in the dexmedetomidine comparator groups.
Included Randomized Controlled Trials
One not evaluable.
IBW, ideal body weight; iv, intravenous; NAS, numeric analogue scale; PGIC, patient global impression of change; RCT, randomized controlled trial; VAS, visual analog scale; vs, versus.
The reported primary outcome measure was visual analog scale (VAS) on a scale of 0–100 mm in four studies,32–35 and numeric analog scale on a scale of 0–10 in one study. 10 It was measured immediately before and after infusion in all studies. It was also measured at a number of other time points before and during the infusion and for up to 14 days after. Other outcome measures included patient global impression of change,10,31 number of rescue analgesic medications,10,31,34 duration of pain relief, 10 reduction of more than 15 mm on VAS, 32 and sedation. 34
Risk of bias within studies
In the placebo comparator group, the risk of bias was not clearly documented in several domains, particularly selection,32,33 performance,31–33 detection,31–33 and attrition 10 bias (Table 3). As four trials were of crossover design, the risk of carryover bias was added to the assessment tool. In the dexmedetomidine comparator trial, 34 there was a high risk of attrition bias and an unclear risk of selection bias. It was attempted to contact authors to clarify data.
Risk of Bias
 Low risk of bias;
Low risk of bias;  Unclear risk of bias;
Unclear risk of bias;  High risk of bias (labeled).
High risk of bias (labeled).
Publication bias
An asymmetric funnel plot was found due to two studies lying outside the 95% confidence interval (Fig. 2).
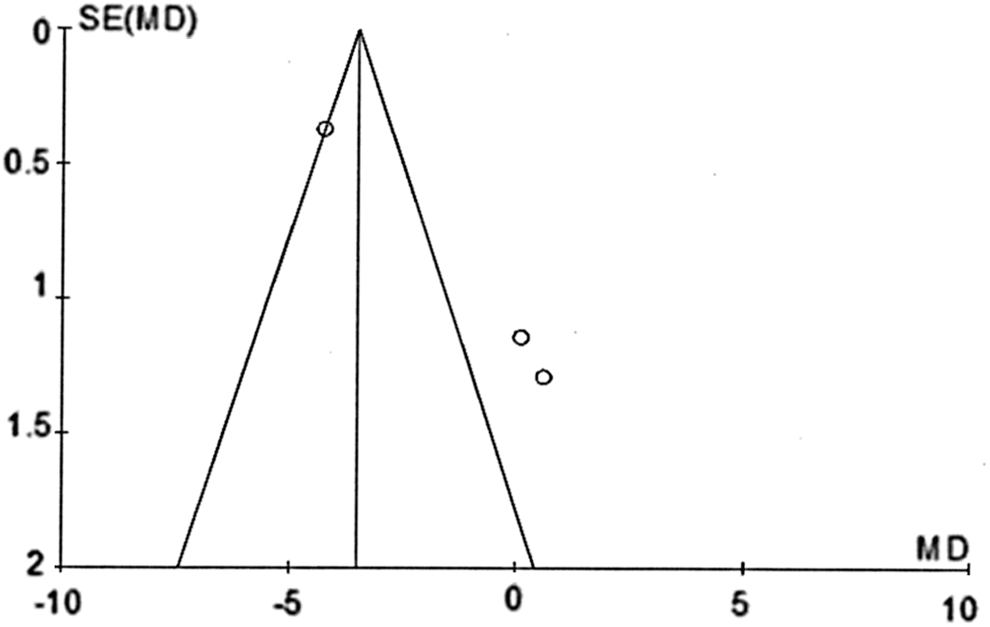
Funnel plot for publication bias.
Results of individual studies
Sharma et al. 10 demonstrated the benefit of intravenous lidocaine infusion, 2 mg/kg over 20 minutes and then 2 mg/kg over 60 minutes, for opioid refractory cancer pain. This was a crossover trial of 50 participants. The groups had similar pain scores at baseline (mean lidocaine 8.48, placebo 8.68). The mean duration of pain was nine months. They found significant (p < 0.0001) reduction in pain score after lidocaine infusion (6.34 ± 1.73) compared with placebo (2.30 ± 2.40). The mean time to onset of maximum analgesic effect after initiating the infusion was earlier after lidocaine (40 ± 16.28 minutes) than placebo (74.80 ± 33.39 minutes, p < 0.001) and the duration of pain relief longer (9.34 ± 2.58 days after lidocaine vs. 3.82 ± 1.87 days after placebo). More patients had substantial pain relief (>50%) in the lidocaine (82%) than the placebo arm (16%). Significantly, more patients reported a subjective decrease in analgesic requirements (64% vs. 30%, p = 0.0012) and an objective reduction in rescue medications used (1.45 ± 0.20 vs. 1.76 ± 0.25 per day, p = 0.01) after lidocaine compared with placebo.
Three studies demonstrated no significant difference in pain score after lidocaine and placebo infusions.31–33 These studies evaluated lidocaine infusion, 5 mg/kg over 30 minutes.
Bruera et al. 31 evaluated 10 participants with neuropathic cancer pain. Pain intensity at baseline was 37/100 before lidocaine infusion and 39/100 before placebo. There was no difference in pain intensity at any time point from 10 minutes after infusion start to day 2.
Ellemann et al. 32 evaluated 10 participants with cutaneous allodynia in cancer. The mean pain score at baseline was 43/100 before lidocaine and 42/100 before placebo. Pain had been present for a mean of 38 months (median 23.5, range 11–120 months). Two participants had a reduction in allodynia immediately after lidocaine, defined as >15 mm on 100 mm VAS. Three participants had a partial reduction after placebo.
Sjogren et al. 33 evaluated 10 participants with bone metastases and pain. Mean pain score over one week at baseline was 54/100. There was no significant difference in the change in average pain during the week before and after infusion. Five patients experienced more than 10 mm pain relief one hour after the infusion of lidocaine and two experienced more than 10 mm pain relief after placebo.
The study comparing lidocaine 3 mg/kg over 60 minutes with dexmedetomidine 34 found no significant difference between the two arms in the visual analog score during infusion.
Meta-analysis of results
Three of the studies evaluated a similar intervention; all compared with placebo and published data pertaining to the outcomes of this review. Individual patient pain score data were provided for two of these studies, allowing manipulation to address the outcomes of this review. The random-effects model was used to estimate the effect size, because although the populations and trials were considered similar enough for meta-analysis, they were not homogeneous. 35
Primary outcome: substantial (at least 50%) pain relief
Meta-analysis of the primary outcome was possible in two crossover trials of lidocaine infusion compared with placebo with a total of 60 participants. It demonstrated significant improvement in the number of participants who gained substantial pain relief with lidocaine (Fig. 3), defined as ≥50% reduction in pain in the postinfusion score compared with the preinfusion score. The risk ratio was 3.29 with a 95% confidence interval of 1.41–7.70 (p = 0.006, I2 = 33%). The quality of the evidence for substantial pain relief is moderate because there were only two studies with a small number of participants. 36

Substantial pain relief.
Secondary efficacy outcomes
Four secondary outcomes were analyzed: the proportion of participants with moderate or better pain relief (Fig. 4), with mild pain after the infusion (Fig. 5), the global impression of change (Fig. 6), and the postinfusion pain score (Fig. 7). These did not demonstrate any significant difference between lidocaine and placebo. Quality of life was not measured in any study.

Moderate or better pain relief.

Mild pain postinfusion.

Patient global impression of change.

Postinfusion pain score.
Adverse events
Adverse events were prospectively sought in only two trials.10,34 In Sharma et al., 11 side effects noted were perioral numbness, sedation, light-headedness, tinnitus, and headache. There was a nonsignificant (p < 0.2) increase in the number of patients experiencing at least one side effect after lidocaine (52% vs. 36%). There were significantly more patients experiencing two or more side effects after lidocaine (24% vs. 4%, p = 0.006). One patient required termination of infusion due to tinnitus, sedation, and perioral numbness. The severity of side effects was not documented. Torres et al. 35 found that the dexmedetomidine group had greater sedation. The remaining trials did not clearly document the rate of adverse effects in the placebo group. One trial 33 reported that 4 patients out of 10 had transient adverse events after lidocaine infusion, including drowsiness, nausea, circumoral paresthesia, euphoria, and confusion. One trial 32 reported that one patient experienced mild but transient drowsiness during and immediately after infusion. 32
Conclusions
Meta-analysis of pooled data in 60 patients identifies that there may be a benefit for lidocaine infusion of 4–5 mg/kg over 30–80 minutes compared with placebo for >50% reduction in cancer pain. However, there are limited data contributing to this comparison, and contrasting with the lack of significance found in secondary outcomes. Based on the current available evidence, lidocaine infusion could be considered in refractory cancer pain where agents with level 1 evidence are ineffective. In many centers, this may require a change in practice. Current guidelines should reflect this. Further research into this promising, potentially opioid sparing therapy is crucial.
Use of the random-effects model gives a relatively greater weighting to the data from Bruera et al. 31 and Sjogren et al., 33 and less weighting to data from Sharma et al. 10 compared with a fixed-effects model. This contributed to the lack of significance in secondary outcomes. This has an impact in the analysis of results in this study because only three studies are suitable for meta-analysis, and the largest study gives opposite results to the other smaller studies. This approach was chosen because the populations in the studies are heterogeneous. It is widely accepted as the statistical model most likely to reflect the true effect in a heterogeneous population. 35 However, it is important to recognize that this choice affects interpretation of data. An alternative approach is to provide only descriptive data of individual studies; however, this is problematic because readers are still prone to draw conclusions about the summary effect, which may be erroneous. In this case, a narrative review would lead many readers to assume a stronger level of evidence for lidocaine, based on the largest, most recent, positive study. This may have underpinned current recommendations for lidocaine, highlighting the importance of this review and the need for more evidence to determine the true effect.
Use of systemic lidocaine infusion in other situations may inform research and clinical practice in cancer pain. There is level 1 evidence for lidocaine in all-cause neuropathic pain, acute renal colic, and critical limb ischemia.8,11,37 The evidence base for intraoperative lidocaine infusion is rapidly changing.38,39 Its use in cancer is a specific type of intervention for which the outcomes are different and warrant studies designed specifically to evaluate these outcomes of interest. In addition, these trials should consider looking at the impact of intraoperative lidocaine on longer term outcomes of chronic pain.
In examining details in this systematic review, preliminary opportunities to further explore lidocaine infusion for cancer pain are identified. The study by Sharma et al. 10 included participants with significantly higher baseline pain scores than the other studies (8.6 vs. 3.7–5.4/10). Lidocaine preferentially blocks nerves with a higher frequency of stimulation and may be more effective in severe pain. Participants in a study by Sharma et al. 10 had had pain for a shorter period than those in a study by Ellemann et al., 32 and the pain types in all the studies were different. The duration of infusion was longer in Sharma et al. 10 than the other protocols. This could provide time for lidocaine to change the neurological structure. 40 However, it still provided analgesic benefit for only nine days. Could a different infusion protocol provide more lasting benefit? Identified randomized controlled trials test only a short infusion up to 80 minutes. No randomized controlled studies evaluate a continuous infusion, which observational studies2,41,42 strongly suggest has benefit and is used in clinical practice. 43
Adverse effects were more common in the lidocaine group than placebo, but there were no serious adverse events due to lidocaine. One participant required cessation of the infusion, with resolution of symptoms. Thus, it appears that lidocaine infusion is relatively safe; however, a comprehensive prospective assessment for adverse effects should be an integral feature of future trials.
Meta-analysis of included trials challenges common interpretations of the evidence base. Given the high proportion of people suffering unrelieved cancer pain, further research is urgently needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.