
Abstract
Abstract
Background:
Patients with end-stage liver disease (ESLD) have high mortality, but low utilization of palliative care. A transitional care liver clinic (TCLC), bridging inpatient hepatology care to outpatient clinics, should offer the ideal setting for advance care planning (ACP).
Objective:
To examine ACP and related outcomes for TCLC patients who died within one year of the initial TCLC visit.
Design:
Retrospective chart review.
Setting:
Nontransplant eligible ESLD patients, seen in TCLC postdischarge from an inpatient liver unit.
Measurements:
Charts were reviewed for demographics, clinical data, ACP discussions, code status, location of death, and palliative care consultations.
Results:
Of the 58 patients who showed for the initial TCLC visit, 18 (31%) died within one year. Most patients were men (67%) with alcoholic cirrhosis (72%), Child-Pugh class C (55.5%) and median age of 56 years (37–72 years). There were no ACP discussions in any TCLC visits even after subsequent hospitalizations. Until their terminal hospitalization, 17 patients (94%) remained full code. Palliative care was consulted for 10 patients (56%). Despite late initiation, within two weeks of death for 6 of those 10 patients, palliative care consultation facilitated arrangements for out-of-hospital death: at home or inpatient hospice (70% vs. 12%, p = 0.01).
Conclusions:
Despite a structured program for ESLD patients, there were no ACP discussions until the terminal hospitalization. These findings support the need to integrate palliative care interventions in the management of ESLD patients, especially taking advantage of postdischarge visits.
Introduction
End-stage liver disease (ESLD) is defined as irreversible decompensated cirrhosis and is associated with frequent hospitalizations and high mortality,1,2 but advance care planning (ACP) and palliative care consultation are underutilized for ESLD patients. 3 A national retrospective study of an inpatient database observed that 30% of patients terminally hospitalized with decompensated cirrhosis had palliative care involvement. 4 Historically implemented in the care of cancer patients, palliative care has become more integrated in the management of end-stage chronic diseases, such as congestive heart failure. 5 Palliative care and hospice interventions in patients with decompensated cirrhosis have led to reduced health care utilization, and have influenced end-of-life care. 6 However, there are multiple barriers to integration of palliative care in ESLD management, including limited availability of resources, lack of physician and patient awareness, discomfort in discussing ACP, unpredictable course of liver disease, and the hope of liver transplantation. 7
Our transitional care liver clinic (TCLC) is a structured program that bridges care from an inpatient hepatology service to an outpatient nontransplant hepatology clinic and should provide a unique opportunity for ACP discussions. This clinic was staffed by a hepatology-trained physician assistant who met the patients before hospital discharge, allowing for better continuity of hepatology care postdischarge. The goal of this retrospective chart review was to examine the use of ACP during TCLC visits and related end-of-life outcomes (code status and locations of death) among TCLC patients who died within one year of the first TCLC visit.
Methods
This was a retrospective chart review of discharged patients scheduled in TCLC from March 2015 to December 2015, with follow-up through December 2016 at a single tertiary academic center. Patients were included if they had ESLD, were nontransplant eligible, were discharged from the inpatient liver service, and were not followed by an outpatient hepatologist or gastroenterologist at another institution. Patients were excluded if they had received a liver transplant previously or within 90 days of discharge.
Given that TCLC was focused on bridging inpatient to outpatient hepatology care, our goal was to assess whether ACP discussions occurred during TCLC visits and if there was any impact on end-of-life care. The primary outcome was documentation of ACP discussions among patients who died within one year of the initial TCLC visit. Secondary outcomes were code status before death, place of death (inpatient, outpatient, and hospice), and palliative care consultations.
Charts were reviewed for demographics, clinical data, palliative care consultation, ACP discussions during TCLC visits, code status, and location of death. Palliative care consultation was available during any inpatient admission and was provided by palliative care physicians. Statistical analyses were performed using chi-square test for categorical data. The statistical software package SPSS for Windows (version 25; SPSS, Inc.) was used to analyze the data, and p < 0.05 was considered a significant difference. This study was approved by the Yale University Institutional Review Board.
Results
Among the 58 patients who showed to the first TCLC visit, 18 (31%) died within one year. The majority were men (n = 12, 67%), with alcoholic cirrhosis (n = 13, 71%), Child Pugh class C (n = 10, 56%), and median age of 56 (range 36–74). These patients were not considered transplant candidates because of active alcohol or substance use (n = 11, 61%), poor social support (n = 2, 11%), untreatable malignancy (n = 2, 11%), advanced age (n = 2, 11%), and irreversible comorbidities (n = 1, 5.5%) (Table 1). The median number of days from the initial TCLC visit to death was 181 days (range 21–356).
Patient Characteristics
HCV, hepatitis C virus; MELD, model for end-stage liver disease; NASH, nonalcoholic steatohepatitis; PBC, primary biliary cholangitis; TCLC, transitional care liver clinic.
ACP, code status, and location of death
There were no discussions of ACP for those 18 patients during any TCLC visits even after readmissions. During the initial TCLC visit, 17 patients (94.4%) were full code and did not have any code status reassessment during subsequent TCLC visits or nonterminal hospitalizations (Fig. 1). The majority of patients died in the hospital (n = 10, 56%) rather than at home or inpatient hospice (n = 8, 44%). Those who received palliative care consultation were more likely to have out-of-hospital death. By the time of death, 14 patients (78%) were comfort measures only (CMO). Among the remaining four patients who were full code by the time of death, three (75%) died in the emergency room after receiving cardiopulmonary resuscitation (CPR).
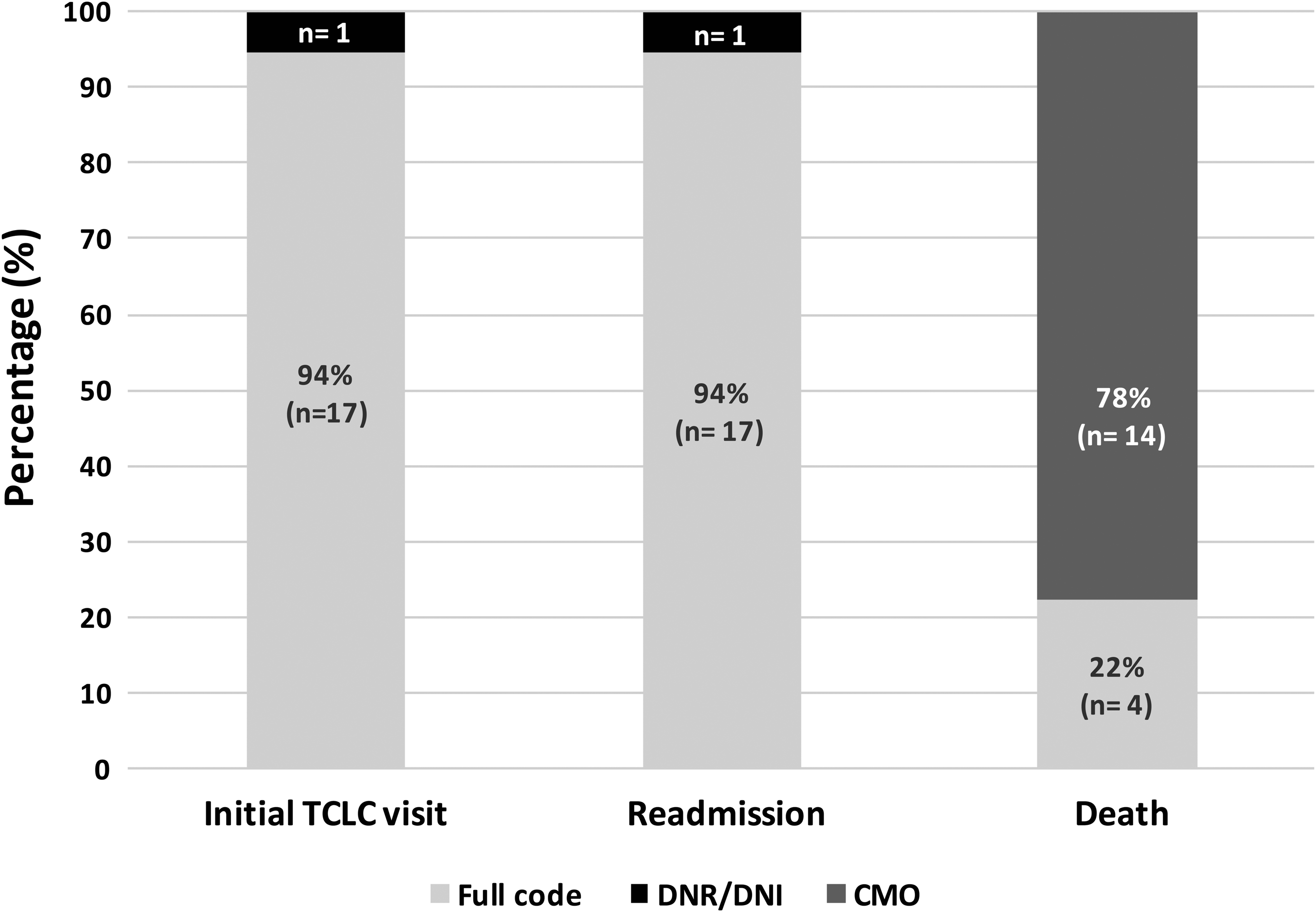
Code status at initial TCLC visit, at subsequent hospital readmission, and at death. CMO, comfort measures only; DNI, do-not-intubate order; DNR, do-not-resuscitate order; TCLC, transitional care liver clinic.
Palliative care consultation
Palliative care was consulted for 10 patients (56%), but it was initiated late, within two weeks of death for 6 patients (60%). There were several missed opportunities for these patients to receive palliative care within their last year of life: 14 patients (77%) were readmitted within one year, 11 (61%) had at least 2 readmissions, and 9 (50%) were readmitted within 30 days of discharge (Table 1). Many of these patients also had follow-up TCLC visits, with a median of 2.5 visits (0–15). There was a trend toward more palliative care consultation among those with malignancy (lymphoma, hepatocellular, renal, and oral cancers): 80% versus 46%, p = 0.31. Despite late initiation, palliative care consultation facilitated arrangements for out-of-hospital death, with more patients expiring at home or hospice (70% vs. 12%, p = 0.01).
Discussion
This study revealed missed opportunities to discuss ACP with ESLD patients who died within one year of their initial TCLC visit. There were no ACP discussions during TCLC visits or nonterminal readmissions for any of the 18 patients. Most patients were full code at the time of admission for their terminal hospitalization. Many of those patients were transitioned to CMO by the time of death, but three patients who remained full code received futile CPR. Palliative care was consulted only during the terminal hospitalization. Even though palliative care consultation occurred late, it significantly affected the location of death by avoiding in-hospital death.
Our findings are similar to a previous study examining outcomes of ESLD patients who were not considered liver transplant eligible. 8 For that cohort, 91% of patients died within one year of ineligibility, and few were referred to palliative care (11%), had do-not-resuscitate orders (28%), and died in hospice or at home (29%). That study, as ours, highlights deficits in end-of-life care and poor utilization of palliative care. Our study shows in more detail where and when code status discussions and palliative care consultation occurred, which was during the terminal hospitalization. As many patients in our study had frequent readmissions, we propose that ESLD patients with recurrent hospitalizations should be prioritized for ACP discussions, either at their postdischarge visit or during their hospital admission. Earlier implementation of ACP can help address short- and long-term goals and lay the framework to tailor treatment modalities as the disease progresses. 9 These initiatives could lead to less invasive medical care, such as hospital admission and CPR.
There are several barriers to earlier implementation of ACP. In many institutions, palliative care consultation for nonmalignant conditions is only available inpatient. Given these constraints, hepatology providers should consider initiating ACP discussions for their ESLD patients. The postdischarge visit, even if not integrated in a TCLC, is an optimal setting in which providers and patients can reflect on prior hospitalizations and re-establish goals going forward. Introduction and continuation of ACP should be one of the priorities of these postdischarge encounters. However, our data suggest potential barriers to these discussions. Out of 18 patients who died within one year of TCLC, 12 (66%) had hepatic encephalopathy and 10 (56%) were not accompanied to the initial TCLC by a family member or caregiver. Patients with decompensated cirrhosis may have significant encephalopathy and limited ability to fully comprehend and navigate conversations and decision making without familial support. Thus, it may be necessary to schedule an additional focused visit with family members to address ACP, given the importance of involving and supporting family members and caregivers.
Limitations of this study include a small sample size and a predominance of middle-aged male patients with alcoholic cirrhosis, which impact the generalizability of our findings. Expanding the study population to evaluate the use of ACP in all postdischarge appointments, including primary care clinics and any gastroenterology or hepatology clinics, could have been a solution to mitigate these limitations, but it was not feasible for our study.
In conclusion, by analyzing data from a structured hepatology program bridging inpatient to outpatient care in ESLD patients, we identified an unmet need for ACP discussions. We suggest that postdischarge clinic visits and hospital readmissions are invaluable opportunities for introducing ACP, discussing advance directives, and initiating palliative care interventions. Future research is needed to evaluate the feasibility and outcomes of integrating a structured approach to ACP for ESLD patients, in both outpatient and inpatient settings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.