
Abstract
Abstract
Background:
Cancer pain remains a difficult problem, for which opioids are often necessary. At present it is difficult to predict the effectiveness of opioid therapy.
Objectives:
We aim to assess the association between patient characteristics and opioid treatment response in cancer patients, and develop a model to predict probability of response.
Subjects:
We used data from two previously published randomized clinical trials, in which patients with head and neck cancer were treated with fentanyl or methadone (total N = 134).
Measurements:
Treatment success was defined as ≥50% pain reduction at one and five weeks. We analyzed patient characteristics (age, sex, depression, and anxiety), treatment characteristics (having had chemotherapy, radiotherapy, surgery, methadone, or fentanyl) and pain characteristics (neuropathic and nociceptive).
Design:
Based on univariable and multivariable regression analyses determinants of therapy success were assessed. Based on these analyses a prediction model was developed.
Results:
Our analyses show that one-week therapy success was associated with methadone (odds ratio [OR] = 5.21), duration of pain in months (OR = 1.12), neuropathic pain (OR = 3.36), and age of the patient in years (OR = 0.95). Inclusion of these four characteristics into our prediction model resulted in an area under the curve of 81.6%.
Conclusions:
Careful analyses of patient attributes, treatment, and pain type of patients with head and neck cancer resulted in a prediction model that allowed to predict short-term pain relief and the opioid treatment response in neuropathic and nociceptive pain owing to cancer.
Introduction
Pain continues to be a major cause of distress in cancer patients. 1 Despite an increased awareness of pain in cancer patients, the prevalence of cancer pain has not changed significantly when comparing the period 2005–2014 with the period 1966–2005. 2 An important algorithm used to treat cancer pain is the World Health Organization pain ladder, 3 which has proven to provide significant pain relief in most patients.4,5 This algorithm suggests treatment of cancer pain using strong opioids at a relatively early stage. Therefore we can say that opioids are the cornerstone of cancer pain management.
Although opioids are highly effective at providing pain relief, some patients do not experience this pain reduction. 6 Despite centuries of experience with opioids, 7 it remains difficult to predict which patient will show a good response, and which patient will show a poor response or needs an incremental dose of opioids. A recent study revealed an association between the presence of liver metastases, breakthrough pain, and nonresponsiveness to opioids. 8 Other studies showed associations between genetic markers such as the mu-opioid receptor (OPRM1) allele, postoperative opioid consumption, and pain relief. 9 Interestingly an association between genetic sensitivity to opioid analgesics and opioid effect in postoperative pain patients was only noted for the first 24 hours. Moreover, the inability to predict an opioid's clinical effectiveness can be a problem when a patient wants to know how effective the pain relief will be.
To address this problem it is important to identify factors that are associated with effectiveness of pain therapy. This could result in more effective treatment of cancer pain using opioid therapy tailored to a patient's profile. Furthermore, a clinician can use these predictors to provide patients with reasonable expectations of pharmacological pain therapy. A retrospective study in patients with neuropathic pain showed that those patients with realistic expectations had lower levels of disability and psychological distress than patients with unrealistic expectations. Patients with optimistic expectations showed lower levels of disability than those patients with realistic assumptions. Patients with pessimistic expectations were characterized by higher levels of catastrophizing and psychological distress. 10
To provide the patient and clinician with the most accurate information about the chance of opioid therapy success, we performed this analysis. We assessed the associations between patient and cancer treatment characteristics and the probability of achieving pain relief with either methadone or fentanyl. In addition, we combined these predictors of pain relief into one model to be able to predict short-term pain relief within one week.
Methods
Source of data
Patient data from two randomized clinical trials were used for this study.11,12 In short, strong opioid-naive patients (i.e., patients had only been prescribed weak opioids such as codeine and tramadol, or no opioids at all) with head and neck cancer and pain (Numeric Rating Scale [NRS] >4) were stratified into two groups. One with a neuropathic pain component, defined as a Douleur Neuropathique 4 (DN4) score of ≥4, and the other with nociceptive pain after radiotherapy-induced mucositis (shortly after the start of radiotherapy). After informed consent was obtained, patients were randomly assigned to either the fentanyl or the methadone group. The randomization was stratified by surgery, chemotherapy, and radiotherapy, and performed using the web-based program TENALEA (Trans European Network for Clinical Trials Services).
The total duration of follow-up was five weeks, and patients were seen four times after informed consent was obtained. At baseline patients provided demographic data, and completed the Brief Pain Inventory (BPI), side effect questionnaires, Hospital Anxiety and Depression Scale (HADS), and Quality of Life (EuroQoL 5D). Methadone 2.5 mg twice daily or fentanyl patch 12 μg/hour was prescribed as well as fentanyl nose spray 50 μg or fentanyl sublingual 100 μg as necessary up to six times per day for breakthrough pain. Because of delivery problems with the methadone 2.5 mg tablets, the starting dose was altered to 2 mg twice daily later in the study.
At one, three and five weeks patients completed the BPI, side effect questionnaires, and global perceived effect (Patient Global Impression of Change [PGIC]). If necessary the strong opioid dose was increased by 50%. As the fentanyl patch has 12 μg/hour as the lowest dose this could only be doubled the first time. If deemed possible the strong opioid dose was decreased by 30% (or stopped if medication was at starting dose). Therapy discontinuation because of side effects was assessed at every visit.
Outcome
The primary outcome parameter used was treatment success, defined as a change in pain score from baseline pain of at least 50%. Pain was measured using an 11-point NRS. For this study, pain measures of one and five weeks after treatment were used to quantify short- and long-term treatment success, respectively.
Determinants of treatment success
In our analyses we measured associations between treatment success and several patient characteristics such as, sex, age, HADS depression score, HADS anxiety score, and HADS total score. Treatment characteristics and pain characteristics were analyzed as well using methadone or fentanyl, having had chemotherapy, having had radiotherapy, having had surgery, pain duration, and pain type (nociceptive [radiation-induced mucositis] or neuropathic [pain with a neuropathic pain component as measured with the DN4]).
Statistical analyses
Before univariable and multivariable analysis, we imputed missing characteristics using multiple imputations. The number of imputations was set to 10, and the imputed values were drawn using predictive mean matching. Compared with the use of completed cases only for the analysis, the use of imputation provides more precision as all subjects will be included for the analysis. In addition, multiple imputations are less prone to yield biased coefficients compared with complete case analysis. 13
We used logistic regression analyses to compute the univariable, or unadjusted, associations between determinants of treatment success and actual treatment success at one and five weeks after opioid treatment initiation. In a subsequent analysis, all parameters were included in a multivariable logistic regression model to correct for other determinants.
To develop a model to predict short-term treatment success, we entered all determinants in a logistic regression model and used backward stepwise elimination to arrive at a more parsimonious model. As suggested by prediction modeling guidelines, we used a less stringent alpha for statistical testing of 0.30. Variables that were selected in over half of the 10 imputed datasets were selected for the prediction model.14–16
The performance of the prediction model was quantified by measures of discriminative ability and calibration. The discriminative ability of the model pertains to the ability of the models to distinguish between patients who will experience treatment success, and those who will not. It is quantified as the area under the receiver-operating characteristic curve (AUC). The AUC ranges between 50% (no discriminative ability at all, like flipping a coin) and 100% (perfect separation between success and no success). Calibration of the model compares predicted probabilities of treatment success to actual probabilities. We visually assessed the calibration plot to assess calibration over the whole range of predicted probabilities. The prediction model was internally validated using bootstrapping techniques.
All analyses were performed using R version 3.3.3.
Results
In total, 134 patients were included in both randomized clinical trials. Because of the imputation step, all patients were included in the analysis. Of all patients, 30 (22.2%) patients reported short-term pain decrease of 50% or more. Baseline characteristics of all patients are given in Table 1.
Baseline Characteristics
Unless otherwise specified.
Gabapentin, pregabalin, or amitriptyline.
BPI, Brief Pain Inventory; Eqol5, EuroQoL 5; HADS, Hospital Anxiety and Depression Scale, depression/anxiety no, 0–7 points; borderline, 8–10; yes, 11–21; SD, standard deviation.
Determinants of treatment effect
Univariable analysis for short-term (one week) and long-term (five weeks) treatment success revealed that only at one week a significant (positive or negative) association with treatment success was noted for (1) having had surgery, (2) baseline pain, (3) neuropathic pain, and (4) treatment with methadone. In the univariable analysis having had surgery was associated with a decreased chance of treatment success. Baseline pain, neuropathic pain, and treatment with methadone were associated with an increased chance of therapy success. Univariable analysis did not show a correlation between age and treatment success (Table 2).
Univariable Associations between Patient Characteristics and Short-Term (One Week) and Long-Term (Five Weeks) Treatment Success
CI, confidence interval; NRS, Numeric Rating Scale; OR, odds ratio.
At five weeks 55 patients were lost to follow-up (7 side effects, 4 deceased, 17 pain free, 8 patients stopped because of other reasons, 16 intercurrent disease, 3 medication stopped by other physician). This loss to follow-up was corrected for by using imputation methods. At five weeks 47% of patients experienced pain reduction of 50% or more; no factor was significantly associated with treatment success.
Predicting short-term treatment effect
The backward stepwise elimination procedure in each of the 10 imputed datasets yielded four predictors for the prediction model for short-term treatment success: age, methadone (compared with fentanyl), duration of pain (in months), and neuropathic pain (compared with nociceptive pain). Age was negatively associated with the probability of short-term treatment success; all other predictors were positively associated. Table 3 comprises all regression coefficients and odds ratios after penalization of the prediction model because of overfitting. The shrinkage factor that was used for penalization was based on our data, which was 0.85.
Prediction Model for the Probability of Short-Term Pain Treatment Success after Opioid Intake
An individual's probability of short-term pain treatment success can be calculated as: 1/(1 + e−LP), in which LP (i.e., linear predictor) = −0.18 − 0.05 × age +1.65 × methadone +0.12 × duration of pain +1.30 × neuropathic pain. For example, a 65-year-old patient who reports experiencing pain for five months, classified as neuropathic pain, who will be treated with methadone has a probability of treatment success of:
LP = −0.18 − 0.05 × 65 + 1.65 × 1 + 0.12 × 5 + 1.30 × 1 = 0.12
Probability = 1/(1 + e0.12) = 0.47 = 47%.
The prediction model discriminated well between patients with and without short-term pain treatment success. The AUC of the prediction model was 81.6% (95% confidence interval: 73.8–81.6). The calibration plot revealed that the model was well calibrated. All subgroups of patients based on similar predicted risk clustered around the 45° line of perfect calibration (Fig. 1).
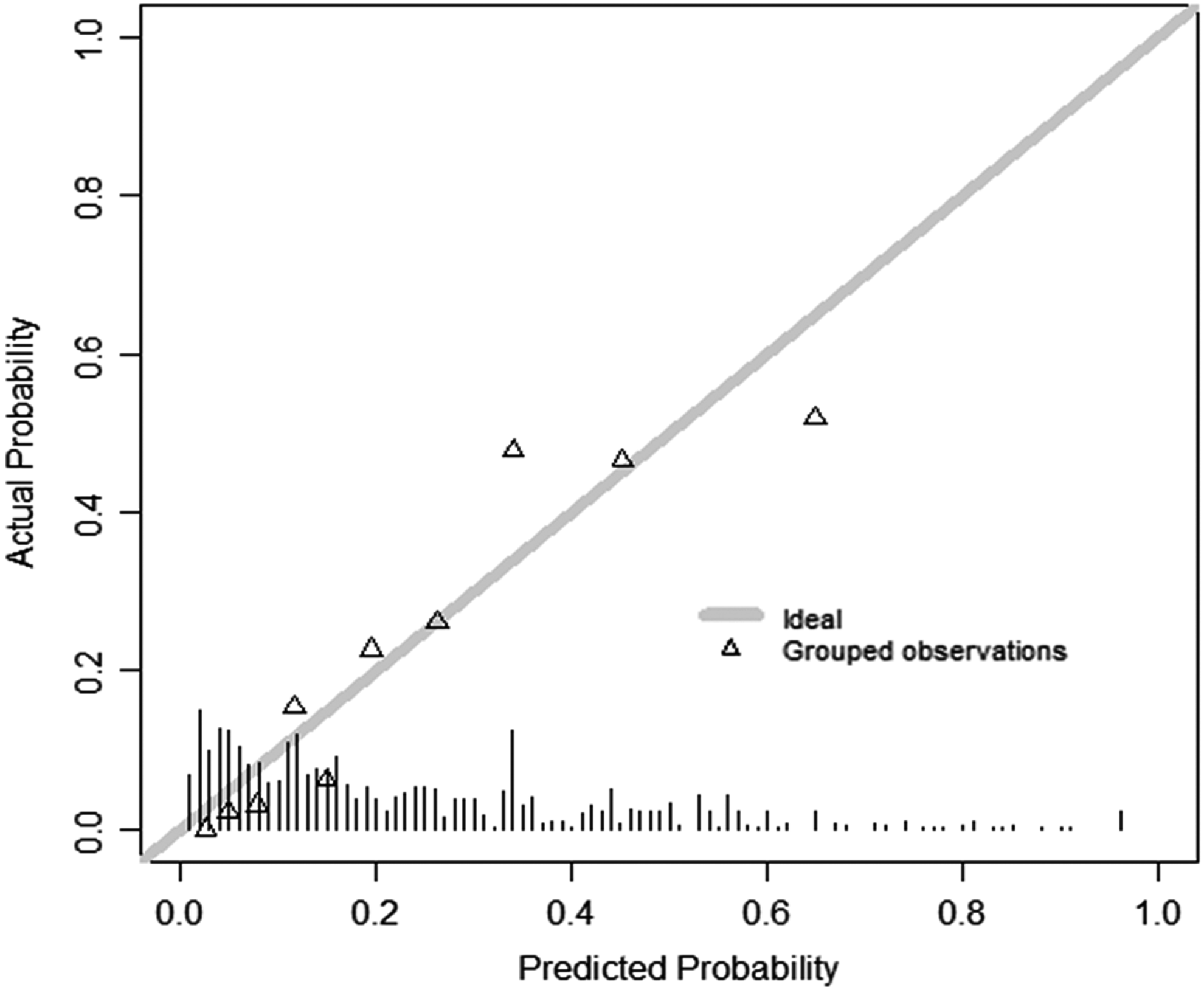
Calibration plot of the prediction model for short-term pain treatment success.
Discussion
In this study we identified multiple predictors of opioid therapy success in head and neck cancer pain, and used these to create a prediction model. This results in an effective model that may be used to predict the chance of therapy success. Although this prediction model needs to be validated, our results suggest that it will be of help for doctors and cancer pain patients to improve the informed, shared decision making around pain medication (i.e., to start opioid therapy, or to try alternative pain medications such as nonsteroidal anti-inflammatory drugs, antidepressants, and gabapentinoids before).
Predictors
The possible predictors as used in this study were chosen based on clinical reasoning and available evidence as prescribed by current guidelines on reporting about prognostic modeling.14–16 Each possible predictor will be discussed separately.
Age
Based on various studies it is suggested that elderly patients respond as well as or even better than younger age groups to opioid therapy, in chronic and in acute postoperative pain.17–19 Hence we expected that age might have a beneficial effect on therapy success (i.e., higher age could result in higher percentage of clinical success). However, in our population we noticed the opposite. Possible reasons for this difference could be related to the fact that there was a limited spread in our population's age (see Table 1), and we did not dichotomize the patient population into a group younger than and a group older than 65 years compared with the abovementioned studies.
An aged population is likely to be at a higher risk for side effects of opioids. This is caused by the increased frailty of this population, and also the higher likeliness of comorbidity and comedication that can result in different interactions. 20 Methadone elimination depends on several cytochrome reduction pathways and on renal filtration. 21 Different pharmaceuticals can interact with the CYP2D6 or CYP 3A4 pathway and cause a decrease or increase of the methadone plasma levels. 22 Fentanyl elimination depends on CYP 3A4, and medication influencing CYP 3A4 activity can influence plasma levels of fentanyl. 23 The transdermal fentanyl patch reduces the first pass effect, and increases bioavailability to ∼90%. However, large variations in plasma level have been measured in different patients, and it has been shown that patients at a higher age absorb less fentanyl than patients at a lower age. 24
The possible unpredictable opioid plasma levels could be a reason to be more careful with opioid therapy in an aged population. Our model shows that an aged population is less likely to benefit from opioids in general.
Anxiety and depression
Anxiety and depression, as measured with the HADS questionnaire, have previously been associated with chronic pain. In chronic pain a higher HADS score has been reported to decrease effectiveness of nonpharmacological pain therapy.25,26 Despite previously reported association between HADS and pain therapy success in chronic pain patients, we were not able to confirm this with our data.
Surgery, chemotherapy, and radiotherapy
We included previous surgery, chemotherapy, and radiotherapy treatment in our analyses as this might affect pain in several ways. It can be argued that surgery, chemotherapy, and radiotherapy might be beneficial to pain treatment, as these therapies might help to reduce or remove the cancer and thus the accompanying pain. However, as these treatments can also cause pain they might also worsen the pain. In our patient population we noted no association between surgery, radiotherapy or chemotherapy, and opioid treatment response. Although surgery seems to be associated with opioid treatment success (with a risk ratio of 0.33, it seems to be associated with a lower success rate), this association was not noticed in the multivariate analysis.
Pain type
The European Federation of Neurological Societies (EFNS) guidelines mention opioids as a second- or third-line therapy for neuropathic pain. 27 In addition, guidelines for cancer pain do advice the use of gabapentinoids, tricyclic antidepressants, or selective serotonin and noradrenaline reuptake inhibitors (SNRI) for neuropathic pain. 28
An important reason for being prudent with opioids in a population with neuropathic pain is the side effect profile and the dependence-producing nature of opioids. Finnerup et al. have shown that opioids do provide good pain relief in a patient population with neuropathic pain, with a number needed to treat (NNT) of 4.3 to provide one patient with 50% pain relief. The maximum effectiveness was noticed at doses of 180 mg morphine or equivalent. 29 This dose and NNT is higher compared with opioids given for acute postoperative pain that can be classified as nociceptive pain. In the latter patient population Moore calculated that oxycodone 10 mg has an NNT of 1.8 or 2.7, depending on the accompanying dose of paracetamol (650 and 1000 mg, respectively). There is no reliable NNT for oxycodone alone. 30
Because the NNT is lower in the nociceptive patient population, combined with a much lower dose we expected that neuropathic pain would have a negative impact on pain therapy success. We were surprised to notice that in our patient population neuropathic pain was associated with a higher chance of opioid therapy success. A possible explanation is the fact that we used methadone that could have effect on neuropathic pain through the N-methyl-
Baseline pain
The univariate analysis showed that a high baseline pain is associated with a higher treatment success, but this was not noticed in the multivariate analysis. We did not expect that the initial pain score would be correlated with opioid treatment success, because we scored success as 50% pain reduction. Patients were not treated differently if they had higher pain scores compared with patients with lower pain scores. Therefore it would be unlikely that baseline pain would be associated with opioid therapy success.
Pain duration
Longer duration of pain is associated with reduced treatment success in pain syndromes such as shoulder and neck pain, radicular pain, and coccygodynia,33–35 but was not associated with therapy success in other pain syndromes.36,37 As there might be an association between opioid therapy success and duration of pain, we included this in our study. Our results show that with pain caused by cancer in the pharyngeal region no association between pain duration and opioid therapy success was noted. A possible explanation is the completely different pain mechanism involved in our population compared with the studies mentioned previously. Furthermore, it is important to note that the average duration of pain in our patient population is much shorter compared with those studies showing an association between duration of pain and lack of treatment success.33–35
Methadone or fentanyl
As the original studies11,12 compared methadone with fentanyl in neuropathic and nociceptive pain in patients with head and neck cancer, we included these medications in our analyses. In the neuropathic pain population methadone proved to be superior to fentanyl on short-term pain treatment. 11 In the nociceptive pain population methadone was not inferior to fentanyl. 12 Because these results showed that overall methadone seems to have a higher success rate, we included these predictors in our analyses. Overall methadone is associated with a better short-term treatment success. Therefore, methadone is a good treatment for cancer pain, as long as the clinician is familiar with methadone and has knowledge of its complex pharmacokinetics.
The additional effect of methadone on the NMDA receptor31,38 is most likely the underlying mechanism that explains the better response of cancer pain patients with a neuropathic pain component to methadone. The NMDA receptor is involved in different pain conditions such as neuropathic pain, pain caused by inflammation, ischemic pain, and allodynia.39–42 Additional blockade of the NMDA receptor by methadone and combined with its opioid qualities can therefore result in further pain reduction and in particular in those pain states associated with central sensitization and NMDA receptor opening such as neuropathic pain and massive nociception.
Long term
The results led us to conclude that the association between patient characteristics and opioid treatment response only exists in the first week (short term), and not at five weeks (long term). In this context it is important to note that our patient population decreased because of loss to follow-up. Although the loss to follow-up is well accounted for, it does reduce the strength of the data. This reduction cannot be compensated completely with imputation methods and might explain the loss of an association at five weeks.
Limitations
This study produced a robust prediction model. However, it should be taken into account that the data are from two specific patient populations: the nociceptive and the neuropathic pain group. This makes it difficult to extrapolate if the prediction model will adequately predict treatment success in other populations. It is important to note that the nociceptive pain population suffered from radiotherapy-induced mucositis. This might affect the effect of radiation therapy and success of pain relief.
Another limitation of this study is that no data were available on how long before study inclusion the patients underwent surgery, chemotherapy, or radiotherapy (except for the patients suffering from radiation-induced mucositis). A further specification of current ongoing therapy might then provide better insights into the possibility of (effective) treatment of the underlying disease or not.
Evaluating factors associated with pain therapy success
Recent data suggest that the presence of liver metastases and breakthrough pain in a mixed patient population were determinants of opioid therapy failure. 8 Differences in patient population and in treatment protocol as used in this study 8 compared with our study might be important reasons for the contrasting results. Our study focused on therapy success, whereas the aforementioned study 8 evaluated therapy failure. The determinants of both therapy success and therapy failure need to be studied in more detail to provide clinicians with relevant data to determine the best possible treatment for the cancer pain patient.
Other characteristics such as genetic variations in the patient population have been shown to be associated with opioid therapy success in postoperative pain. However, the OPRM1 gene is only associated with pain therapy success at 24 hours, and this association is no longer significant after 48 hours. 9 The use of a prediction model can be of great help for the clinician. Different prediction models are in use and help doctors predict the likelihood of correct diagnosis or chance of successful therapy. It is important to note that an AUC of 0.82 is a good prediction model for the chance of therapy success. A diagnostic model should have a higher AUC, such as the model predicting the chance of appendicitis in children with an AUC of 0.91. 43 However, in a predictive model for achieving pathologic complete response in patients with breast cancer, an AUC of 0.77 is considered good. 44
Although we do have a good prediction model for therapy success, it is necessary to validate this model in another patient population. This model still needs external validation, therefore we did no add a specific normogram. We hope that more studies will focus on characteristics associated with pain therapy success to improve our model. Possible characteristics to include in an improved model could be genetics and proteomics.
Conclusion
This study shows that age, type of pain (neuropathic pain component vs. nociceptive pain), pain treatment (methadone vs. fentanyl), and pain duration are important determinants of opioid therapy success in patients with pain as a result of head and neck cancer. Using these determinants in a prediction model results in an effective model that may be used to predict the chance of therapy success, but only after external validation. This model can help the clinician to provide accurate information to the patient and improve shared decision making in a vulnerable patient population.
Footnotes
Acknowledgment
The authors thank Jaap Hol for his support.
Author Disclosure Statement
The authors have nothing to disclose, this research was performed without funding.