
Abstract
Abstract
Background:
Many of the leading causes of infant mortality are diagnosed prenatally, presenting providers with the ability to present perinatal palliative care planning as an option.
Objective:
Our study adds to the literature both by describing infant interaction with the health care system and by gaining deeper understanding of the maternal experience after being offered perinatal palliative care.
Methods:
The study was conducted at a public university-based medical center in the Midwest. Phase 1 consisted of a retrospective review of electronic medical records of 27 mother–infant pairs offered perinatal palliative care, 18 of whom elected to develop a perinatal palliative care. Phase 2 consisted of a focus group and interviews of seven of the mothers.
Results:
In the initial phase of this study, results revealed differences regarding the infant's end-of-life trajectory, including location of death, number of invasive procedures, and death in the setting of withholding versus withdrawing life-sustaining treatment. Highlighting that without a perinatal palliative care plan in place, the default treatment for infants with prenatally diagnosed life-limiting conditions is likely to be invasive and painful with often times minimal likelihood of long-term survival. Analysis of interview and focus group data revealed three themes: care, choice, and legacy.
Conclusion:
The authors used their experience with the health care system to draw implications for practice from the focus group and interview data, which care can serve to promote women feeling cared for and cared about, as well as promote opportunities for hope during a fragile pregnancy.
Introduction
W
Palliative care for infants was first described in 1982 2 and over the past three decades, the concept has evolved. A 2012 review by Balaguer et al. identified 101 studies on neonatal palliative care, with 25% of those studies focusing on perinatal palliative care. 3 Existing literature focuses primarily on the composition of the palliative care team, 4 illustration of a palliative care plan, 5 or description of the patient population served.6,7 Few studies have described the infant interaction with the health care system after birth6,8 and although there has been a recent increase in literature involving parental viewpoints of perinatal palliative care,9,10 the recent review by Rocha Catania et al. 11 confirms that perinatal palliative care is a growing area of scholarship. Our study adds to the literature both by describing infant interaction with the health care system and by gaining a deeper understanding of the maternal experience among mother's who contemplated perinatal palliative care during pregnancy from which important implications for practice are described.
Methods
The study was conducted at a public university-based medical center in the Midwestern USA. Study approval was obtained from the Institutional Review Board. At our institution, mothers, whose fetus has a prenatally diagnosed life-limiting condition, including, but not limited to, chromosomal abnormalities, renal anomalies, central nervous system anomalies, cardiac malformations, or other severe structural anomalies, receive care through the interprofessional Fetal Diagnosis and Treatment Center (FDTC). Referrals to the perinatal palliative care program (PPCP) are made following FDTC discussion and group consensus. The palliative care plan is entered into the maternal and fetal electronic medical record. During the study period most plans included do not attempt resuscitation (DNAR) orders with plan for exclusively comfort care, which pediatric hospitalists provided on the obstetric ward until either death or discharge to home with hospice care. For families who chose intensive care, the PPC team remained involved to offer concurrent care in the neonatal intensive care unit (NICU).
Phase 1 of this study consisted of a retrospective review of electronic medical records by the principal investigator (P.I.) between 1/2011-9/2014 to determine how many mothers of infants with a life-limiting condition were offered perinatal palliative care. Twenty-seven infants were identified (Fig. 1). Descriptive statistics (i.e., median, percentage) were used to describe the patient populations, continuous data were analyzed using the Mann–Whitney U test, and categorical data were analyzed with Fischer's exact test.
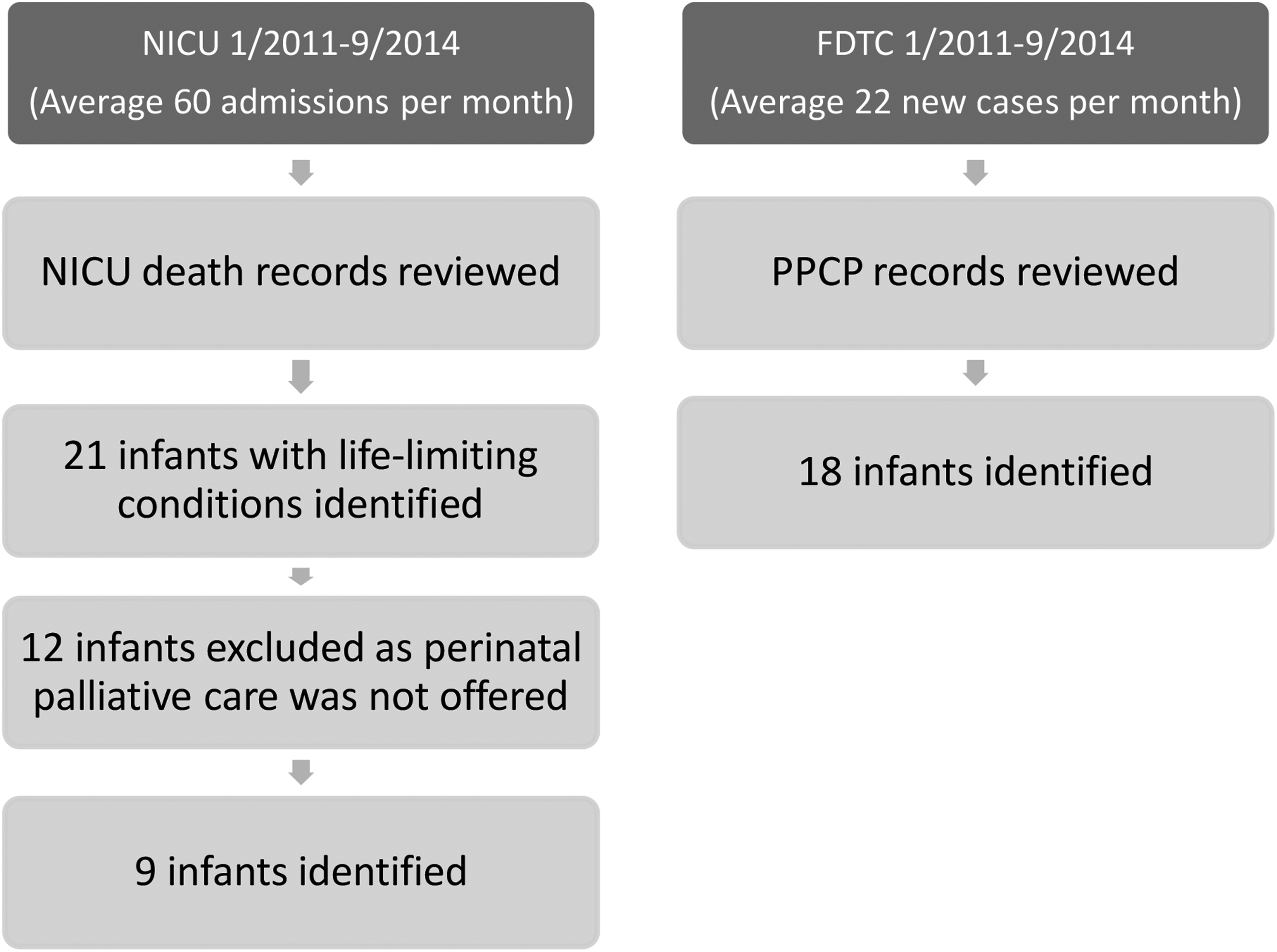
Infant identification and inclusion. FDTC, Fetal Diagnosis and Treatment Center; NICU, neonatal intensive care unit; PPCP, perinatal palliative care program.
Phase 2 of this study were focus group and interviews to gain deeper understanding of maternal experience after being offered PPC (Fig. 2).
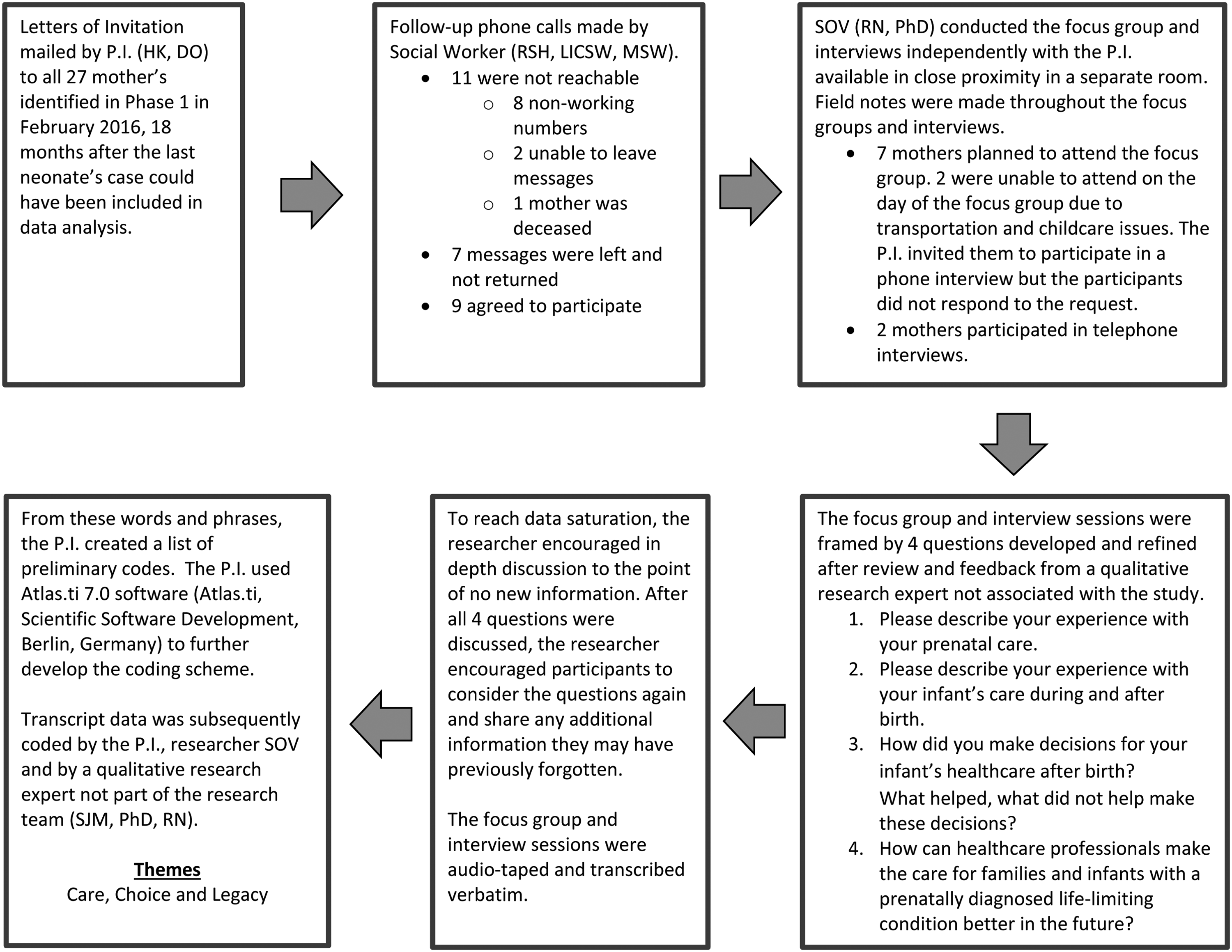
Focus group flowchart. P.I., principal investigator.
Researcher S.O.V. led the focus groups and interviews. She is currently Associate Professor in the School of Nursing at her home institution. She has extensive experience in qualitative research and is published in numerous peer-reviewed journals.12–14 To begin the focus group and interview sessions, the consent form was thoroughly reviewed by the researcher allowing time for questions. Each participant received a folder, which included a consent form, demographic form, Complicated Grief Questionnaire, 15 mental health resources, and an honorarium.
The focus group and interview text analysis were simultaneous and continuous. Each member of the research team independently read through the typed transcripts to get a sense of the whole. Following this review, members of the research team met to discuss the coding scheme, extract common themes, and identify relevant quotations. From this analysis, researchers used an inductive approach to combine the codes into three major themes related to the maternal experience of receiving a life-limiting diagnosis during pregnancy.
Results
Data from the initial phase of this study were obtained from maternal and infant electronic medical records and are summarized in Tables 1 and 2. For mothers, there was a statistically significant difference between the groups in the proportion of mothers who were receiving medical assistance. There were no statistically significant differences between the infant groups. Results revealed differences regarding the infant's health care system interaction after birth, summarized in Table 3. Thirty-three percent of those invited agreed to participate in the focus group/interviews. Analysis of the focus group/interview data revealed that five study participants completed the Complicated Grief Questionnaire, 12 none of whom met criteria for a complicated grief diagnosis. Qualitative data analysis revealed three themes: care, choice, and legacy.
PPCP, perinatal palliative care program.
Data for one of the mothers were not available.
Includes: intubation, umbilical catheter placement, needle decompression, chest tube placement, percutaneously inserted central catheter line placement, therapeutic hypothermia, pericardial tap, extracorporeal membrane oxygenation, ex utero intrapartum treatment procedure. Does not include peripheral venous catheter, nasogastric/orogastric tube placement.
DNAR; ICU, intensive care unit; NICU, neonatal intensive care unit.
Theme: Care
The participants in our study appreciated expert and personalized care from the interprofessional team. This level of care requires excellent team communication and comprehensive care for women who are offered perinatal palliative care planning. Medical providers should encourage the “normal” within the extraordinary for these patients and families and should advocate for memory making whenever possible. The participants in our study objected strongly to the language “incompatible with life” as a descriptor for their infant's condition. Certainly there are many ways to convey the likely death of a newborn without using terminology, which evokes such a negative response.
Theme: Choice
Participants also identified the lack of provided resources as a deficit in otherwise generally positive care experience. Many participants described learning of options for their child's care through online organizations, which were ultimately able to be supported by the medical team. It would be prudent for organizations providing high-risk obstetric care and/or neonatal consultation to have a list of resources available for families to reference. Medical teams should provide all medically appropriate options available, including termination, palliative care, and aggressive care early to support informed maternal decision making and autonomy.
Theme: Legacy
Interprofessional perinatal palliative care teams should promote legacy formation with focus on the infant, family, and larger community. These legacy opportunities are present from diagnosis, through pregnancy as well as after birth. It is beholden on us as the care team to identify and anticipate these opportunities for families, especially for those families who find meaning through opportunities, such as organ donation or research. Ultimately, the care these mothers received, the choices they made, and the experiences/memories come together to form a lasting legacy no matter how close together hello and goodbye might be.
The authors used their experience with the health care system to draw implications for practice from the focus group and interview data, presented in Table 4 along with selected supporting quotations.
Quotations are attributed to the participant in parenthesis after the quotation. For example, (P1) indicates the comment was made by participant 1.
Discussion and Conclusion
Perinatal palliative care is a recent advancement in the field of palliative care medicine. In this sample, 67% of participants offered perinatal palliative care developed a care plan. Perhaps most striking is that for those families that developed a PPCP, 89% of deaths occurred in the setting of with-holding life-sustaining intervention. For those who did not, 72% ultimately chose to withdraw life-sustaining treatment for their infant, but the remaining 28% died in the setting of cardiopulmonary resuscitation. This study highlights that without a perinatal palliative care plan in place, the default treatment for infants with prenatally diagnosed life-limiting conditions is likely to be invasive. Despite routine comfort measures, including nonpharmacological, oral sucrose, and pain medications as needed, there are aspects of intensive care that are painful with often minimal likelihood of long-term survival. For those diagnoses where survival is not expected, PPCP should be an integral part of comprehensive prenatal collaboration, an approach to care, which is supported by the American Academy of Pediatrics policy statement: Noninitiation or Withdrawal of Intensive Care for High-Risk Newborns. 16
Thus far, literature in this field has primarily focused on perinatal palliative care team composition, implementation, and scope. Our study adds important insight from those most intimately affected by the diagnosis of a fetal life-limiting diagnosis, the pregnant mother. Limitations of this study include that it is a single-center study with retrospective demographic data, which are limited due to inconsistency in documentation of ethnicity, religion, and education. Only mother–infant pairs with a perinatal palliative care plan or whose infant died in the NICU were included. This study does not include mother–infant pairs without a prenatal diagnosis or mother–infant pairs who declined perinatal palliative care where the infant survived to discharge. Additionally, we do not present data from significant others regarding their experience.
Empathic interprofessional care can serve to promote women feeling cared for and cared about as well as promote opportunities for hope during a fragile pregnancy. Decision making can be supported by care teams who are open minded, provide comprehensive choices, are able to anticipate memory making opportunities, and importantly avoid use of the term “incompatible with life.” Ultimately, the care and choices during pregnancy develop into a legacy these mothers have created for their child, a legacy which lasts beyond the final heartbeat.
Footnotes
Acknowledgments
This research was partially supported by a grant from the Benjamin Walker Hanson Neonatology Fund, part of the University of Minnesota Foundation. The authors would like to thank Sonja J. Meiers PhD, RN who provided expertise on focus group text analysis.
Funding Source: Ben's Buddies, Roseville, MN.
Author Disclosure Statement
No competing financial interests exist.