
Abstract
Abstract
Background:
End-of-life (EOL) care in neonatal intensive care units (NICUs) can vary depending on religious beliefs of health care providers and families as well as the sociocultural environment. Although guidelines exist for EOL care in NICUs, most are based on Western studies, and little is known about such care in Asian countries, which have different religious and social background.
Objective:
This review synthesized empirical research to reveal the state of the science on infant EOL care in Asian countries.
Design:
This was an integrative review.
Setting/Subjects:
Data were collected from studies identified in CINAHL, Embase, PsycINFO, and PubMed. The search was limited to current empirical studies involving infant EOL care in Asian countries and published in English between 2007 and 2016.
Results:
Of 286 studies initially identified, 11 empirical studies conducted in Hong Kong, India, Israel, Japan, Mongolia, Taiwan, and Turkey were included in the review. Four themes were captured: factors influencing decision making, trends in decision making, practical aspects of EOL care, and health care providers' preparation. In most NICUs, health care providers controlled decisions regarding use of life-sustaining treatment, with parents participating in decision making no more than 60% of the time. Although care decisions were gradually changing from “do everything” for patient survival to a more palliative approach, comfort care at the EOL was chosen no more than 63% of the time.
Conclusion:
While infant EOL care practice and research vary by country, few articles address these matters in Asia. This integrative review characterizes infant EOL care in Asia and explores cultural influences on such care.
Introduction
The World Health Organization has emphasized care for dying children by recognizing it as a key global mandate in the Global Action Plan 2013–2020.1,2 In the last decade, with this emphasis, the number of end-of-life (EOL) care programs and research studies focusing on dying infants and their families has increased dramatically in the United States, as has the amount of position statements of care providers' associations and the publication of suggested guidelines.3–9 Because the concept is value-laden, EOL care for infants and their families can vary according to religious beliefs and the health care providers' attitudes, the families' involvement, hospital policies, societal culture, and a country's laws and economic status.10–12 As Asia (which includes the Middle East and Central, East, and South Asia13,14) is a continent with a wide variety of religions,13,15,16 it is beneficial to review research conducted in Asian countries to learn how EOL care is delivered in neonatal intensive care units (NICUs) to patients and their families.
Despite the number of infant deaths in Asia constituting about 33% of the world's deaths and neonatal deaths constituting about 37% of the world's deaths, 17 few studies of EOL care for dying infants have been conducted in Asian countries and published in the English language. A previous study of EOL care in adult intensive care units (ICUs) in Asian countries indicated that the possible reason for the sparse research in the adult population is that physicians in most Asian countries are less likely to limit life-sustaining treatment (LST) at the patient's EOL than Western physicians. 11 In addition, the possible discomfort associated with having an EOL conversation with families, anticipated legal liability, and unfavorable societal culture that views dying and death as a taboo subject may hinder research being conducted in this region. 18
Although there is little research describing the current status of infant EOL care, effort has been made to develop a standard of EOL care in Asian countries.19,20 Liu et al. 20 reviewed current ethical issues in Western countries' NICUs to determine the fundamental ethical guidelines that should be in place in China. In addition, Al-Alaiyan and Al-Hazzani 19 reviewed current EOL care recommendations to identify cultural barriers to providing neonatal palliative care in Saudi Arabia. However, even though Asian research directly reflects the current status of EOL care, so that health care providers in that region can benefit from using these practices, no synthesis of Asian studies has been performed.
Therefore, this integrative review aimed to synthesize the empirical research into EOL care in NICUs in Asian countries to delineate the current status of EOL care in Asia, including research concerns and issues in this geographical area. The results of this review, which is the first to address this issue in Asia, will enhance understanding of EOL care in Asia and provide important evidence of culturally relevant EOL care practice for dying infants and their families in ICU settings.
Methods
Search strategy
This review was guided by the integrative review methodology recommended by Whittemore and Knafl. 21 An online search of four electronic databases (CINAHL, Embase, PsycINFO, and PubMed) was performed using a combination of keywords and subject headings. These were related to the type of care practice (terminal care, hospice care, EOL care, and death or dying), the care location or population (NICU, neonates, newborns, and infants), and the continent containing the countries of interest (Asia, which is the physical geographic location that includes the Middle East and Central, East, and South Asia).13,14 In addition, an ancestry search and journal hand search were performed to avoid potential publication bias. 22
Selection of studies
Following PRISMA's guidelines, 23 the review included empirical studies of any design that were published in English and involved EOL care in Asian countries in NICUs for infants less than 12 months of age and their families. After deleting duplicates and non-English publications, the search was limited to scientific articles and other documents published in the last decade (2007–2016). These years were selected because this review's goal was to explore current issues in EOL care in Asia.
After abstract screening, the studies that did not focus on care for dying infants, that focused only on older children, that focused only on time after death, that did not reflect the current status of an Asian country, or that focused only on mortality or epidemiology rather than the patient's care were excluded. After screening of the full text, 11 articles (10 quantitative and 1 qualitative) were included in this review. Figure 1 illustrates the study selection process.
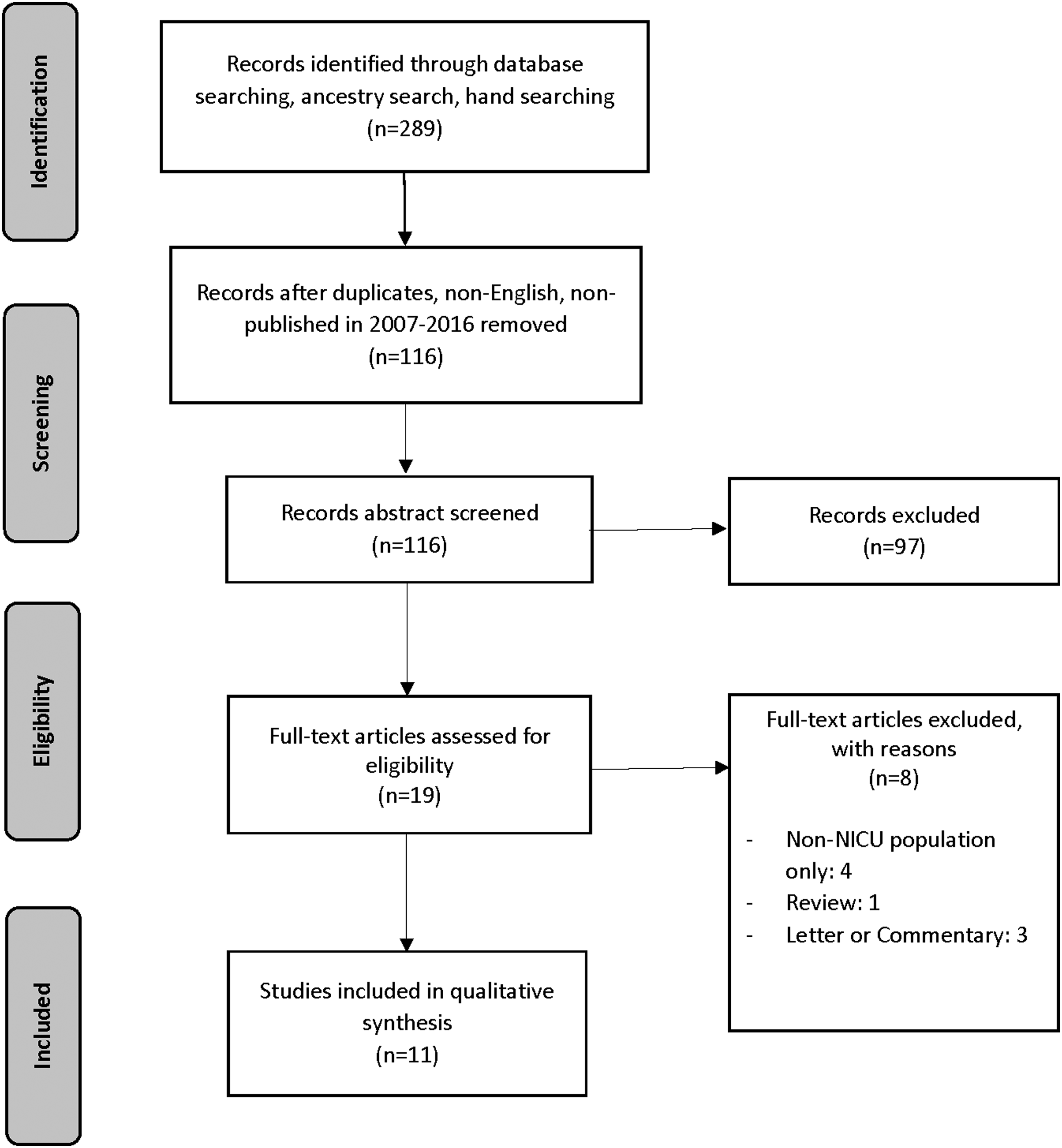
PRISMA flow diagram for selection of review articles.
Data analysis
Each included study's quality was appraised using a quantitative or qualitative tool, as appropriate.21,24 For the quantitative studies, the National Institutes of Health's tool for observational cohort and cross-sectional studies was used. 25 This tool uses a quality rating based on 14 items, whereby a score of 0–4 points is viewed as poor, 5–9 points as fair, and 10–14 points as good quality. 25 For the qualitative study, the Critical Skills Appraisal Programme was used. 26 This tool uses a quality rating based on 10 items, whereby a score of 0–4 is determined to be not valuable and a score of 5–10 is valuable. Garrard's 27 matrix method was used to facilitate the analyses of the study data. The matrix in Table 1 includes information about each article included in the review. Based on the matrix method, a constant comparison approach was used for the data analysis in this review.21,27
Included Articles Describing Neonatal End-of-Life Care in Asian Countries
AR, active resuscitation; DNR, do not resuscitate; EOL, end of life; HCP, health care provider; LST, life-sustaining treatment; NICU, neonatal intensive care unit; NRP, neonatal resuscitation program; WD, withdrawal; WH, withholding.
Results
A total of 11 empirical studies conducted in 7 Asian countries were identified for inclusion in this review (Table 1). Of these 11, 5 were conducted in Taiwan28–32 and 1 each in India, 33 Hong Kong, 34 Japan, 35 Israel, 36 Mongolia, 37 and Turkey. 38 Ten were quantitative and one was qualitative. Regarding the quality appraisal of each study, 9 of the 10 quantitative studies were appraised as fair and 1 was appraised as good quality. 25 The one qualitative study achieved 7 points out of 10. 26 Table 1 includes a summary of the 11 studies' quality appraisal characteristics.
Overall, 11 themes were derived from the analysis, which were grouped into four categories of neonatal EOL care: (1) factors influencing EOL care decision making, (2) trends in EOL care decision making, (3) practical aspects of EOL care, and (4) health care providers' preparation. Table 2 describes these categories and themes.
Captured Themes and Categories
Factors influencing EOL care decision making
The most common themes observed among the studies involved factors influencing decision making regarding LST or resuscitation at the infants' EOL. Four groups of factors influencing EOL care and related decision making were described: (1) infant, (2) family, (3) health care provider, and (4) cultural and societal factors.
Infant factors
In three studies, gestational age, future harm, infant condition, and “preciousness” were identified as infant factors influencing EOL care decision making. While health care providers tended to initiate resuscitation if an infant was born after 28 weeks of gestation,33,37 they also considered the possible long-term pain resulting from the resuscitation. 37 In addition, the infant's condition at the time of the counseling for EOL care influenced the parents' decisions toward LST withdrawal. 34 If the parents had a history of infertility, recurring losses of fetuses, or babies conceived through in vitro fertilization, the infant was considered “precious,” and health care providers considered more aggressive ways of saving these babies' lives. 33
Family factors
In Asian countries, the impact of the extended family and intrafamilial dynamics were significant.32,33 In a Taiwanese study, 38% of do not resuscitate (DNR) consents were provided through the collective decision making of family members, 32 and in an Indian study, extended family elders were the primary decision makers. 33 In India, the families' financial status was also a consideration of the health care providers for avoiding potential financial risks. 33 A Taiwanese study emphasized the influence of the parents' religious beliefs on the infants' dying by performing their religious ritual at the EOL. 32
Health care provider factors
The health care providers' personal or religious beliefs toward EOL care and attitudes about death were factors influencing EOL care decisions.28,29,37,38 Their religion commonly influenced their decision for EOL care in the Mongolian study, 37 and in another study conducted in Taiwan, the providers' attitudes were an influencing factor on EOL care. 28 Furthermore, the nurses' work experience and personal attitudes about death were identified as factors influencing their attitudes toward EOL care. 28 In addition, physicians expressed their discomfort in communicating with family members about DNR decisions and the need for help from a clinical ethics committee with the EOL care decision-making process. 29
Cultural and societal factors
In most studies, health care providers and family members were influenced by cultural and societal perspectives toward EOL care. In particular, specific cultural and societal perspectives were described as being interwoven with ethical considerations. 33 In an Indian study, the health care providers could not overcome the society's gender discrimination; they decided to withdraw LST for female infants, even if there was hope of recovery. In a study in Israel, 36 the authors described increased acceptance of intensifying treatment by Jewish religious authorities. In three studies, the need for organizational and regulatory guidelines28,33 and ethical committees' policies for EOL care 38 was emphasized.
Trends in EOL care decision making
A number of studies described trends in EOL care decision making, including trends in the changes in, or the current status of, EOL care decision making31,32,34,36,38 and parental roles in decision making and related counseling.31–34,36–38 Overall, the decision-making trend in Asian countries has changed from “do everything” for dying infants to withdrawal or withholding of LST. Two studies34,36 described a rising trend of withdrawal in Hong Kong and a decreasing trend of aggressive care in Israel. Investigators in the study in Turkey 38 reported that 40% of health care providers had experienced LST withdrawal or withholding cases. In two Taiwanese studies, high numbers of infants had a DNR order before death.31,32 However, the extubation rate of an endotracheal tube or cessation of mechanical ventilation was not high in a Taiwanese study and the Hong Kong study.32,34
The Israeli study 36 reported increased parental discussion, parent requests, and parent considerations by the medical team in decision making, and the Hong Kong study described the increased participation of parents in making EOL care decisions. 34 However, although there were efforts to facilitate interdisciplinary meetings with parents, family counseling for EOL care decision making still had low rates of occurrence in Hong Kong and Taiwan.32,34 The family counseling content involved anticipated financial costs, prognoses, expected lengths of hospital stays, 33 and plan for postnatal resuscitation. 37
Practical aspects of EOL care
Several studies described various practical aspects of EOL care. A Taiwanese study indicated that there was limited EOL care practice by reporting that a small number of infants received analgesics or comfort intervention, but that there was a high intubation rate at the EOL. 31 In addition, another Taiwanese study stated that nurses' perceived barriers to providing EOL care were insufficient education and counseling for staff, inability to express personal thoughts about EOL care, insufficient staffing, lack of policies/guidelines, technological imperatives (the belief that because technology is available, it must be used to save the infant), parental demands, and previous experience of caring for dying infants. 28 Conversely, another Taiwanese study described NICU nurses' efforts to deliver EOL care. In that study, families were given time to talk to, hold, breastfeed, and touch dying infants, and nursing EOL care practice included offering a quiet place for grieving, providing emotional support for parents, and bathing and dressing dead infants. 32
Health care providers' preparation
Two studies conducted in Taiwan and Japan addressed health care providers' preparation for EOL care.30,35 Peng et al. 30 described a lack of education among Taiwanese neonatal nurses, even though they frequently experienced infants' dying and deaths. The education most needed involved infant pain management and communication with family members. 30 The Japanese study evaluated an EOL care educational program that they had developed. The program was effective for enhancing clinical understanding and knowledge of EOL care, improving the ability to support families and neonates, and giving nurses the ability to self-appraise so that they could learn by identifying their weaknesses.
Discussion
Key concepts of infant EOL care in Asia
In this integrative review, we identified four key categories of themes of infant EOL care in Asian countries: (1) factors influencing EOL care decision making, (2) trends in EOL care decision making, (3) practical aspects of EOL care, and (4) health care providers' preparation. Although these themes bear similarities to those identified in the United States, studies differing emphases were also observed. While the U.S. studies tend to focus on actual EOL care practice and its quality improvement,39,40 most Asian studies focus on attempting to shift paradigms in EOL care decision making. For example, in a previous review of North American neonatal EOL care, four care categories were revealed: (1) practices of withdrawing or withholding LST, (2) pain management during ventilator withdrawal, (3) parents and the decision-making process, and (4) the dying process. 40 In addition, the American College of Critical Care Medicine 39 has recommended practical guidelines in six domains: (1) patient and family-centered care and decision making, (2) ethical principles relating to the LST withdrawal, (3) practical aspects of withdrawing LST in the ICU, (4) symptom management in EOL care, (5) considerations at the time of death, and (6) research, quality improvement, and education.
Although EOL practice can be accompanied and facilitated by decision making about EOL care, our review revealed limited overall discussion of decision making about withdrawal and withholding of LST. Depending on the country, we found a large variation in the level of discussion of decision making about matters ranging from decreasing aggressive care to increasing withdrawal and withholding of LST. Although Hong Kong, Israel, and Turkey showed an increasing trend of favoring LST withdrawal and withholding by up to 63%, the percentages were much lower than in Europe (up to −90%) 41 and in the United States (97%–99%). 12 In addition, although the results showed an increasing parental role in infant EOL care decision making, it was apparent that EOL decisions were still made solely by health care providers in many Asian countries.32,34 Future research that examines Asian parents' perspectives of shared decision making with health care providers would provide much needed knowledge for shaping EOL care.
Interestingly, many Asian studies mentioned cultural, religious, and societal influences on EOL care and decision making. For example, in Taiwan, parents tended to express their religious beliefs in songs during the time of their infant's death, as Buddhists believe that the circumstances of one's death can affect one's situation in the next stage of reincarnation. 32 In addition, physicians reported religious influences on their decision making, and gender discrimination, consideration of the families' financial status, and the religious authority's position were described as societal factors in the reviewed studies.33,36,37
Comparatively few Asian studies have examined the actual practice of infant EOL care and the related education among care providers; only two Taiwanese studies and one Japanese study addressed these concepts.30,32,35 Because physicians' and other health care providers' education about EOL care is crucial to improving the quality of care practice, more studies and educational efforts at the institutional level should be performed for health care providers.
Amount and quality of research into infant EOL care in Asia
Relatively few empirical studies published in English address the current status of infant EOL care in Asian countries. This lack of studies focusing on infant EOL care in Asia may be caused by ethical challenges, lack of EOL practice, and lack of English articles. The lack of research is not necessarily surprising, as EOL care research encounters both practical and ethical challenges. 42 As evidence of these challenges, many of the studies reviewed were conducted using chart reviews or surveys of health care providers. Although the perspectives of the care recipients themselves are of greatest interest, it is very difficult to collect data directly from infants who are not able to communicate or from family members who are greatly affected by their children's dying and death.
The reviewed studies' qualities also revealed challenges. The majority of reviewed studies received a score of “fair” on the quality-rating tool. A study's quality can be rated as high if multiple assessments were performed with a large number of participants, or if it was designed to examine causal relationships among variables. 25 However, because of the difficulty of collecting the data for EOL care research in the NICU population, most studies were one-time assessments with small numbers of participants. As a result, the quality of most reviewed studies was fair.
Our review had limitations that should be acknowledged. First, although this review aimed to comprehensively reflect the current status of neonatal EOL care in Asian countries, only articles written in English were included and fully reviewed. Therefore, articles written in other languages may offer relevant information beyond that presented in this study. In addition, our study's results have limited generalizability. Because we only reviewed research that focused on the NICU environment, this review does not fully reflect all infant EOL care in Asian countries. In particular, countries that do not have fully furnished NICU settings were not considered. Although this review aimed to synthesize research studies that examine EOL care in Asian NICUs, a variety of issues based on the countries, health care system, and culture prevented a more synthesized integration. However, this review provides a better understanding of the current issues in this region, including the increasing interest and understanding of the patients' families in decision making and their participation in EOL care.
Conclusion
Our review is the first integrative review to address the current status of NICU EOL care in Asia. We identified variability in the decision making for EOL care and practice as well as the limitations of the care and research in this region. In the future, high-quality studies are needed that further examine the reasons for the lack of practice and research or that enhance the quality of EOL care by educating health care providers and gaining a better understanding of the affected parents' perspectives.
Footnotes
Author Disclosure Statement
No competing financial interests exist.