
Abstract
Abstract
Background:
Patients with cancer and palliative care needs frequently use the emergency department (ED). ED-based palliative services may extend the reach of palliative care for these patients.
Objective:
To assess the feasibility and reach of an ED-based palliative intervention (EPI) program.
Design:
A cross-sectional descriptive study of ED patients with active cancer from January 2017 to August 2017.
Subjects:
Patients with palliative care needs were identified using an abbreviated 5-question version of the screen for palliative and end-of-life care needs in the ED (5-SPEED). Patients with palliative care needs were then automatically flagged for an EPI as determined by their identified need.
Measurements:
The primary outcome was the prevalence of palliative care needs among patients with active cancer. Secondary outcomes were the rate of EPI services successfully delivered to ED patients with unmet palliative care needs, ED length of stay (LOS), and repeat ED visits within the next 10 days. Categorical variables were evaluated using chi-squared or Fischer's exact test as appropriate. Continuous variables were evaluated using analysis of variance.
Results:
Of the 1278 patients with active cancer, 817 (63.9%) completed the 5-SPEED screen. Of the patients who completed the screen, 422 patients (51.7%) had one or more unmet palliative care needs and 167 (39.6%) received an EPI. There were no differences in ED LOS or 10-day repeat ED visit rates between patients who did or did not receive an EPI.
Conclusion:
This ED-based intervention successfully screened for palliative needs in cancer patients and improved access to specific palliative services without increasing ED LOS.
Introduction
Up to 80% of cancer patients visit the emergency department (ED) during the last six months of life, with nearly two-thirds presenting more than once.1–3 The ED is a critical point of care for patients with active cancer; oftentimes, these visits are for care that is palliative in nature, including visits for pain, dyspnea, nausea, vomiting, confusion, and anxiety.1,4–6 Many of these visits are potentially avoidable if patients with active cancer had earlier access to outpatient palliative care. 7
Despite recommendations for early implementation of palliative care for patients with cancer by the American Society of Clinical Oncologists (ASCO) and the American Academy of Hospice and Palliative Medicine (AAHPM),8,9 and evidence that palliative care improves patient and family member quality of life and decreases health care costs and hospital resource utilization, long delays between cancer diagnosis and palliative consultation are common.10–18 On average, oncology patients at cancer centers in the United States in 2009 died within one week of inpatient palliative consultation. 19
Because patients with cancer frequently use the ED, and long delays exist between cancer diagnosis and palliative care consultation, the ED may be a key location to expand the reach of palliative care for patients with cancer. However, due to the fast-paced nature of emergency medicine practice, palliative care is not typically part of standard ED care. Previous emergency medicine-palliative care research has largely focused on the development of screening tools to help expedite palliative care consultation rather than address the needs directly.20–22 In addition, the incidence of unmet palliative care needs in ED patients with cancer has not been well characterized.2,20 Finally, there is limited research on ED-based palliative interventions (EPIs) focused on identifying and addressing palliative needs. The existing studies are limited by their retrospective design.23,24 Given the clear benefits of early palliative engagement in oncology care, as well as the regularity with which cancer patients utilize the ED, we sought to enhance patient access to palliative services by delivering ED resources to address unmet palliative needs.
The primary aims of this study are to quantify the unmet palliative care needs of patients with active cancer presenting to an urban academic ED, and to assess the feasibility of using EPIs to address those needs. In addition, a secondary aim is to assess the impact of implementing EPIs on ED operational metrics such as length of stay (LOS) and return visits to the ED.
Methods
Study design
This is a cross-sectional descriptive study of patients with active cancer and palliative care needs from January 20, 2017 to August 18, 2017. This study was reviewed by the Institutional Review Board at Northwestern University and deemed exempt from review.
Study site
Northwestern Memorial Hospital (NMH) is an urban academic hospital affiliated with one of only 45 NCI-designated Comprehensive Cancer Centers in the nation. Robert H. Lurie Comprehensive Cancer Center of Northwestern University treats >10,000 new cancer cases annually and is home to a supportive oncology team that includes clinical psychologists and psychiatrists who provide mental health services to cancer patients. The ED has >88,000 adult patient visits per year with ∼2800 visits per year by patients with active cancer. At the time of data collection, the ED operated on an integrated electronic health record (EHR) (Cerner FirstNet). At the time of data collection, the ED had the ancillary care service providers dedicated to and physically present in the ED as follows: social work (five days per week, 08.00–22.00), clinical pharmacist (seven days per week, 07.00–23.00), patient referral services (six days per week, 08.00–18.00), and transitional care nurses (TCNs) (five days per week, 10.00–20.00).
The EPI project was an administrative initiative built on the demonstrated success of the TCN program.25,26 As part of regular operations in the ED, and the TCN program, 2.0 full-time equivalent positions are staffed for each specialty, TCN, social worker, and pharmacy. Before initiation of this project, key stakeholders within the institution, including ED physicians, nursing leadership, and palliative care leadership, were involved throughout its development. Preintervention sessions were conducted with all of the ED resource services to review consultation goals, anticipated workload, and expected challenges. Throughout the EPI project rollout and execution, regular meetings were continued between the team leading the EPI project (four resident physicians and three research faculty members), the ED pharmacy lead, the ED social workers, members of the TCN team, a supportive oncology psychiatrist, and four nurse champions. Operational feedback with rates of intervention consults per eligible patients was provided to each consulting resource service monthly in a continuous process of quality improvement.
Participants and procedures
All adult (>17 years old) ED patients were screened for active cancer and inclusion in this intervention during the initial bedside nursing ED assessment. This screening was a routine part of care before the EPI project was initiated. For the purpose of this study, a patient with active cancer was defined as a patient who (1) was undergoing or in the past 12 months had undergone cancer-directed therapy (radiation/chemotherapy), (2) was known to or found by care providers in the ED to have metastatic disease, or (3) reported directly that he or she had symptoms related to known cancer (pain, fatigue, nausea, etc.).
The screen for palliative and end-of-life care needs in the ED (SPEED) Survey is the first published tool that was derived as an ED-specific palliative care screening tool.20,27,28 SPEED focuses on five key areas of palliative care: pain management, home care, medication management, psychological support, and goals of care. It has since been adapted into a rapid five-question needs assessment named 5-SPEED. 27 In >1500 cancer patients hospitalized through the ED, increasing 5-SPEED score was associated with increased likelihood of inpatient palliative care consultation. 27 A custom 5-SPEED EHR screen was built for the EPI project and automatically inserted into the normal template of the bedside-nursing triage form. Both patients and nurses were able to opt out of screening if the clinical context did not allow for screening or the patient was not interested in answering the questions. Each domain of the 5-SPEED is scored on a 10-point Likert scale. Thresholds for screening “positive” in each domain were previously established by ED and palliative care experts.27,29
For those patients who screened positive by 5-SPEED, an automatic EHR-based consult was placed to the appropriate ED resource service for each positive screen (Fig. 1). Therefore, if a patient had multiple palliative care needs, they would be eligible for multiple EPIs. Pharmacy consultations were initiated for patients with pain and medication reconciliation needs. Social work was consulted for those with unmet home care needs. The TCNs were consulted for those with unmet goals of care needs and an appointment referral was placed to supportive oncology for those with emotional distress.
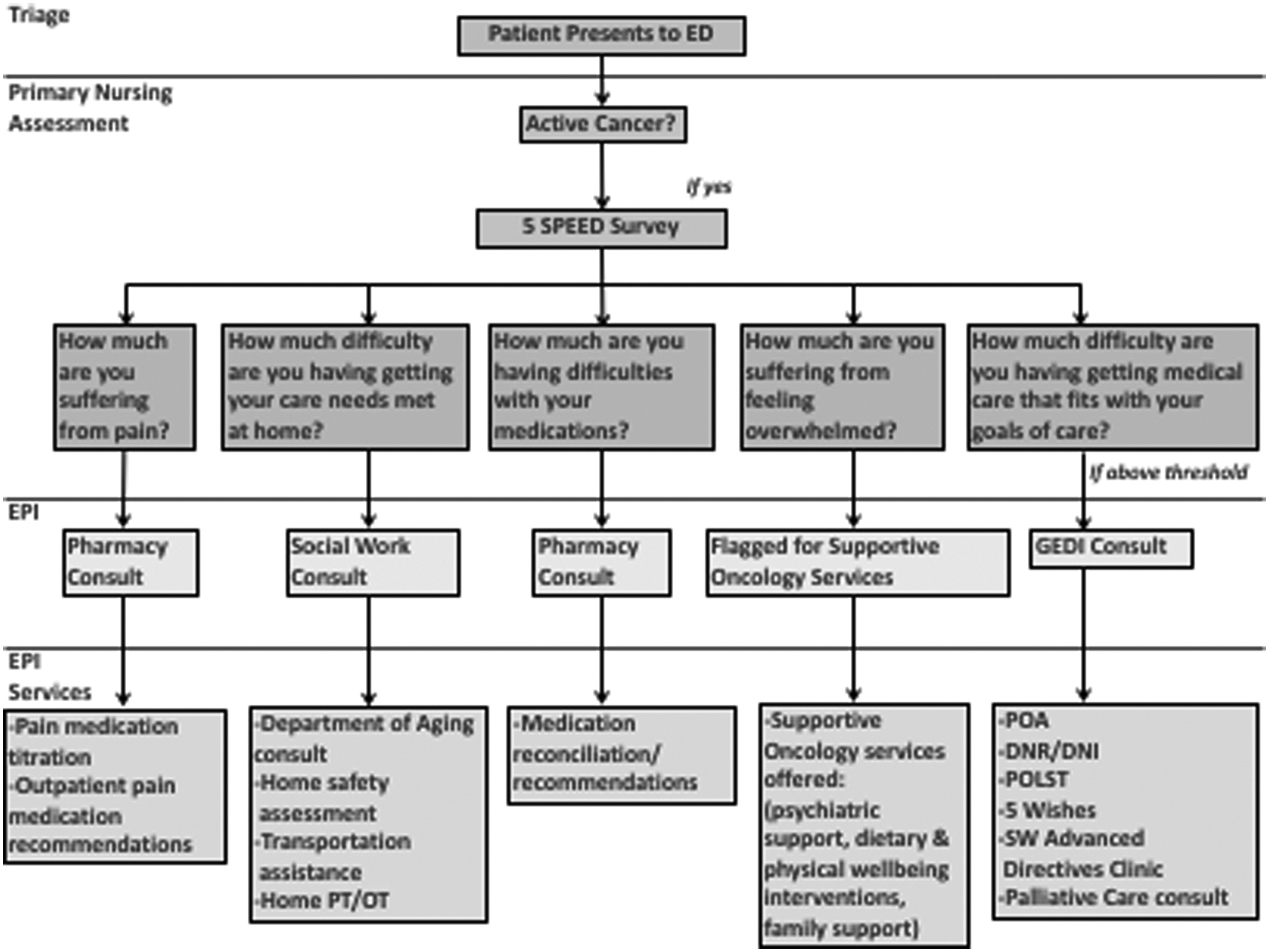
The Emergency-Department-based Palliative Intervention Algorithm (ED, emergency department; 5-SPEED, Screen for Palliative and End-of-Life Care Needs in the Emergency Department-5; GEDI, geriatric emergency department innovations).
Measures
In addition to being used to qualify for inclusion in the EPI pathway, the 5-SPEED was also used to quantify our primary outcome: the prevalence of unmet palliative care needs in the five domains among patients with active cancer. Secondary outcomes of interest included the rate of successful consultation by an ED resource service, ED LOS, rate of discharge from the ED, and return ED visits within 10 days of discharge from the ED. Additional data, including patient and visit characteristics related to both screening and delivery of EPI services, were collected, including the Emergency Severity Index (ESI). ESI is a five-level ED triage algorithm that provides clinically relevant stratification of patients into five groups from one (most urgent) to five (least urgent) on the basis of acuity and resource needs. 30
All data were obtained from the EHR. Data related to the rate of active cancer, completion of 5-SPEED screen, 5-SPEED score and positive domains, ED revisit rates, patient and visit characteristics were obtained from the Electronic Data Warehouse, an internal EHR data storage service. The successful completion of a consultation by an ED resource service was obtained based on documentation completed by the consulting service in the EHR that links the consultation specifically to the positive 5-SPEED screen.
Analysis
For the primary outcome of interest, we report the percentage of active cancer patients with unmet needs in each palliative domain. To evaluate the reach of the EHR-integrated screening and intervention effort, we report the rate of completed consultations. For additional secondary outcomes of interest related to the operational metrics, patients were divided into four groups: (1) Cancer patients not screened, (2) 5-SPEED screen negative, (3) 5-SPEED screen positive, but with no EPI delivered, and (4) 5-SPEED screen positive with EPI delivered. Descriptive statistics were used to describe the characteristics of each of these groups. Analysis of variance was used to compare the ED LOS between groups, and chi-squared tests were used to evaluate difference between groups for all categorical variables, including repeat ED visits within 10 days. All analyses were performed using STATA 13.1 (StataCorp LP, College Station, TX). As our primary outcome was descriptive, we did not perform an ad hoc power analysis. Subsequent effect size analysis determined we had power to detect a 9.2% change in ED LOS, and a 4.8% change in return visits to the ED.
Results
For the seven-month study period, 1278 patients with active cancer presented to the study site ED. Of these, 817 completed the 5-SPEED screen. Demographic characteristics such as age, gender, ethnicity, and insurance coverage were largely similar between cancer patients not screened with 5-SPEED, 5-SPEED negative patients, and 5-SPEED positive patients. Patients with an ESI triage level of 1 and patients with public insurance (Medicare and Medicaid) were less likely to be screened. 5-SPEED negative patients had a slightly higher likelihood of being discharged from the ED (30.9%) compared with patients with one or more palliative care needs identified by 5-SPEED (p = 0.004) (Table 1). Palliative care needs were identified in 422 (51.7%) by the 5-SPEED screen. Many patients had more than one unmet palliative care need: 163 (19.6%) had one unmet need, 107 (13.1%) patients had two unmet needs, 85 (10.4%) had three unmet needs, 27 (3.3%) had four unmet needs, and 35 (4.3%) had five unmet needs. Among cancer patients screened, 289 (35.4%) had an unmet pain need, 130 (15.9%) had home care needs, 131 (16%) had medication challenges, 235 (28.8%) had emotional distress, and 130 (15.9%) had issues with their goals of care (Table 2).
Demographics, Emergency Severity Index Level, and Emergency Department Disposition
ED, emergency department; EPI, ED-based palliative intervention; ESI, Emergency Severity Index; SPEED, screen for palliative and end-of-life care needs in the ED.
Cancer Patients Screened with 5-Screen for Palliative and End-of-Life Care Needs in the Emergency Department (n = 817)
Of the 422 patients with an unmet palliative care need, 167 (39.6%) received an EPI during their ED stay. Of these patients in need, 75 (26.0%—pain) and 36 (27.5%—medication reconciliation) received a pharmacy consultation, 32 (24.6%) had a social work consultation to address home care needs, and 32 (26.2%) received a TCN consultation to address issues with goals of care (Table 2). Of the 167 patients receiving an intervention, 97 (58.1%) received one intervention, 54 (32.3%) received two, 15 (9.0%) received three, and 1 (0.5%) received four. There was no statistically significant difference in LOS between these groups. The initial plan for an automated referral to supportive oncology through the in-ED Physician Referral Service (PRS) staff was unsuccessful due to high PRS staff turnover, and the increased complexity with performing this referral compared with usual referrals in the ED. There was no statistical difference in ED LOS and 10-day ED revisit rates between cancer patients not screened, 5-SPEED negative patients, 5-SPEED positive patients who did not receive an intervention, and 5-SPEED positive patients who received one or more interventions (Table 3).
Emergency Department Length of Stay and 10-Day Repeat Emergency Department Visits
LOS, length of stay.
Discussion
This article describes a novel care pathway, the EPI project, which identified cancer patients with unmet palliative care needs and addressed those needs through existing ED resources at an urban academic medical center. The care pathway utilized EHR-embedded screening and automated EHR-triggered consultation that delivered palliative services to ED cancer patients while not affecting ED LOS.
This is the first study to our knowledge to detail the rate of palliative care needs for patients with cancer in the ED. We found that >50% of active cancer patients presenting to the ED during the study period had one or more unmet palliative care needs. In a recent systematic review, Wong et al. were unable to determine the incidence of patients with palliative care needs in the ED due to limitations in available data. 2 Our study shows not only the feasibility of screening in the ED for palliative care needs but also demonstrates high prevalence of unmet care needs in the population sampled. The data from this study may also serve to further support recent calls for prospective interdisciplinary study of ED-based palliative services given the high prevalence of unmet need that was found in this sample.31,32
Using existing ED resources, we were able to deliver specialized care to nearly 40% of the cancer patients with unmet palliative care needs. The inability to address a higher proportion of patients in need was multifactorial. In part, this rate of EPI delivery was due to staffing; as noted earlier, many of the ED consultation resources are unavailable during evening and overnight hours. During weekday, daytime hours, the workload already placed on these ED services is extensive and limited their ability to evaluate every cancer patient with a palliative need. Furthermore, it was also a central goal of developing the pathway such that it did not affect ED operational metrics negatively, namely ED LOS. As such, normal care delivery was not delayed for EPI consultation, and many patients with unmet needs may have been already admitted or discharged before an EPI team member could address their palliative care needs. Furthermore, the intervention rate calculation included patients with emotional distress, and although the initial PRS-driven intervention was unsuccessful, the chart review approach captured all patients with emotional distress after June 2017 and forwarded their information to supportive oncology. Unfortunately, we were unable to capture this data in our EMR data query. As such, the overall intervention rates appear lower than the true proportion of patients receiving an EPI for their palliative care need. Finally, while completing chart reviews we found consults often contained improper documentation resulting in an inability of our data query to capture these EPI consults.
Although we had modest success in addressing the needs of those for whom screening was completed, only 64% of cancer patients presenting during the study period received a 5-SPEED screen. In discussing the screening process with nurses, there are several reasons for this suboptimal rate of screening. First, some patients are too ill, too distressed, or unwilling to participate in the 5-SPEED screen. As seen in Table 1, those patients categorized as ESI level one or two, those thought to need the most expedient emergency care in the ED, were the vast majority of those cancer patients not screened. This finding suggests the acuity of presentation may have been a limiting factor in screening rates within this group in comparison with those with less urgent ESI levels. Although the 5-SPEED screen was rarely used in these critical situations, emergency physicians frequently perform a brief informal evaluation of goals of care and treatment preferences for critically ill patients.
In addition, discussing topics such as emotional distress and goals of care are difficult issues to address and quantify in a bedside screen, especially one taking place in the ED with nurses who have just met the patient and their families for the first time. Nurses commented that when they first attempted screening, they encountered tearful and anxious patients when discussing emotional distress and goals of care and felt uncomfortable asking these questions. These negative experiences made the nurses reticent to perform the screening with future patients for fear of being in similarly emotion-laden conversations. Despite frequent nursing education, it was difficult to reach a high rate of successful screening due to these challenging issues.
To our knowledge, this is the first published work attempting to address palliative care needs with ED-specific interventions.23,24 To date, emergency medicine/palliative care research has largely focused on the development of screening tools to help expedite palliative care consultation.20,21 A recent study by Gruzden and colleagues in 2016 showed that ED-initiated palliative care consultation improved quality of life in patients with advanced cancer and had no detrimental effect on one year survival. The finding that using ED-based resources did not negatively impact patient LOS may support other programs in garnering administrative support for similar pathways. The EPI care pathway ultimately seeks to extend the reach of palliative care services to communities that currently do not have sufficient access, including minority populations, smaller communities, and rural centers by utilizing the ED as both a novel arena for the delivery of multidimensional palliative interventions and a palliative care safety net. We note that EPI may require the addition of ED resources, which smaller EDs may not currently have; however, access to these services are all recommended in the geriatric ED guidelines. 33 As EDs work to meet the GED guidelines and geriatric ED accreditation, access to these services for patients with palliative care needs should be considered. 34
This initial description of a unique EPI project has some limitations. The outcomes reported are process and operational outcomes, rather than clinical and patient-centered outcomes, which were not measured. Future work will focus on quantifying the impact of the intervention on patient's quality of life, reassessment of the 5-SPEED palliative care needs, the rates of subsequent palliative care involvement, patient survival, ongoing functional status, and days spent in hospital and ICU. Only two-thirds of patients with active cancer were screened. If nurses were selectively screening patients in whom they anticipated a need, the prevalence of need estimate may be falsely elevated. However, even if all unscreened patients were 5-SPEED negative, the unmet need in this sample would still be 33% (422/1278).
This was a single site study and external generalizability is limited as many resources may not be readily available at smaller, nonacademic institutions. Specifically, the TCNs, who have received specialized training through the Education in Palliative and End-of-Life Care for Emergency Medicine (EPEC™-EM) course, are a unique resource in the NMH ED. However, the EPEC-EM course is widely available and nurses and ED staff could be trained to conduct these challenging conversations with cancer patients. The supportive oncology department is also a highly specialized resource dedicated to addressing the well-being of cancer patients and their families, and may not be available at other hospitals. Nevertheless, many oncology departments have social workers who provide similar support for cancer patients and many psychologists who help to manage anxiety and depression within the cancer populations, making this intervention potentially feasible at a wide variety of health care systems. In addition, supportive oncology follow-up was unsuccessful as initially planned; therefore, in June 2017 the EPI Team personally forwarded patients' contact information for supportive oncology follow-up. The initial PRS process had a low rate of success with only two total patients having their information forwarded in the first five months of the study period. After the change in process all patients with emotional distress had their information forwarded; however, this is unlikely to be a sustainable long-term solution.
Conclusions
The EPI pathway provides a novel approach to delivering palliative care services to oncology patients by utilizing the unconventional setting of the ED. These data demonstrate that the need for such services is great with a majority of screened patients with active cancer reporting unmet needs. This EHR-enabled solution streamlined nursing screening and auto-triggered consults thereby requiring no manual consult entry or extra work from ED physicians. By leveraging existing ED resources, we not only effectively screened for palliative needs, but also enhanced patients' access to palliative services without increasing ED LOS. The EPI pathway holds promise for extending the reach of palliative care services in many diverse ED settings.
Footnotes
Acknowledgments
The GEDI Team: Alicia Salgado-Lau, RN, Emily Ruben, RN, Dorelen Cieciel, RN, Rebecca Zakem, RN, Elizabeth Zdyb, RN, Lisa Lui-Popelka, RN, Catherine Wilk, RN, Jacline Barrett, RN, Dwayne Dobschuetz, RN, Suzie Condon-Paskiewicz, LCSW, Ashley Yoke, LCSW, Patricia Marchman, LCSW, Katie Allen, PharmD, Eileen Brassil, RN, Joshua Hauser, MD, Timothy Pearman, PhD, Sanjeev Malik, MD, James Adams, MD.
Author Disclosure Statement
No competing financial interests exist.