
Abstract
Abstract
Background:
No study has compared the effects of hemodialysis on the symptom burden of terminally ill and nonterminally ill end-stage renal disease (ESRD) patients.
Objectives:
This study aimed to examine the effects of hemodialysis on the symptom burden of ESRD patients and compare the terminally ill and nonterminally ill groups.
Design:
This was a quantitative survey; for patients on hemodialysis, the survey was conducted at the beginning and end of the weekly cycle of hemodialysis sessions.
Setting/Subjects:
A total of 211 ESRD patients were recruited in Taiwan, 47 of which were terminally ill (38 on hemodialysis) and 164 nonterminally ill (110 on hemodialysis).
Measurements:
Symptom burden was assessed using the Taiwanese version of the MD Anderson Symptom Inventory for kidney disease.
Results:
Being terminally ill predicted higher symptom severity (B = 0.604, p = 0.017), whereas hemodialysis predicted lower symptom severity (B = −0.614, p = 0.014) in ESRD patients. Nonterminally ill patients who were married or on hemodialysis experienced lower symptom severity (B = −0.604, p = 0.013 and B = −0.665, p = 0.017, respectively). Among terminally ill patients, neither hemodialysis nor other background characteristics predicted symptom severity. When hemodialysis was initiated, no change in symptom severity was observed in terminally ill and nonterminally ill patients.
Conclusions:
The effects of hemodialysis on symptom burden were different between ESRD patients with different disease states. Hemodialysis predicted lower symptom severity only in nonterminally ill ESRD patients. Apart from dialysis, care providers should revisit the palliative approach for treating terminally ill ESRD patients to improve their quality of life.
Introduction
T
Because of waste and extra fluid removal with hemodialysis, ESRD is better controlled, and associated symptoms are expected to be attenuated. However, this is not well supported in the literature. A qualitative study revealed that some patients experienced worse physical symptoms after initiating dialysis, 5 and several studies have uncovered an enormous symptom burden in dialysis-dependent patients, such as fatigue, pain, depression, sleep disturbance, and sexual dysfunction.6–9 However, whether the symptoms are caused by dialysis remains unclear, because most studies did not include nondialysis patients as the comparison group; thus, the symptoms are potentially attributed to conditions coexisting with ESRD or side effects of medication rather than dialysis alone. 10
Some ESRD patients are not usually treated with dialysis because they choose conservative management or do not require dialysis based on their clinical condition. Similar to dialysis patients, nondialysis patients often report substantial symptom burden.9,11–13 Given that symptom experience is a critical determinant of health-related quality of life (HQOL) and HQOL is closely associated with morbidity and mortality in ESRD patients, 14 understanding the differential symptom burden in dialysis and nondialysis groups is important.
In addition, patients with ESRD have a wide spectrum of prognoses. Although some patients with ESRD can survive decades while receiving dialysis or after transplantation, some patients with severe comorbid conditions have a rather short life expectancy. 4 It is debatable whether ESRD patients with very poor prognosis may benefit from dialysis. 15 Patients approaching the end of life can be considered as candidates for a palliative approach to focus on supportive care rather than restorative care, as long as it is aligned with the values and health care goals of patients. 16 However, evidence on the symptom burden of this particular patient population, which may provide important information for considering the role of dialysis in end-of-life care for ESRD patients, is limited. 17
This is the first study to include both hemodialysis and nonhemodialysis patients with the aim to (1) examine the symptom burden of dialysis and nondialysis ESRD patients, (2) compare the symptom burden of dialysis and nondialysis patients in terminally ill and nonterminally ill ESRD subgroups, (3) examine the effects of hemodialysis and other background characteristics on the symptom burden of terminally ill and nonterminally ill ESRD patients, and (4) examine the change in symptom burden from the beginning to the end of a weekly cycle of hemodialysis sessions.
Methods
Study design
The study was a quantitative survey. For hemodialysis patients, the survey was conducted at two time points—at the beginning and end of the weekly cycle of hemodialysis sessions. For nonhemodialysis patients, the cross-sectional survey was used at the time of recruitment.
Sample and settings
The study was conducted in two teaching hospitals in New Taipei City, Taiwan. Hemodialysis patients were recruited from the hemodialysis center, whereas nonhemodialysis patients were recruited from the nephrology outpatient clinic. Participants were ESRD patients (i.e., those with glomerular filtration rate <15 mL/[min ·1.73 m 2 ] with no existing reversible factors to restore kidney function). Patients who communicated in Mandarin or Taiwanese, ≥20 years old, without cognitive impairment were included in the study.
A total of 211 participants were recruited, 47 of which were considered terminally ill and 164 were nonterminally ill ESRD patients. In this study, the terminally ill ESRD patients were defined, in accordance with the Taiwan Ministry of Health and Welfare of the National Health Insurance Administration, as (1) those with severe uremia and approaching death based on the assessment of a renal specialist team and/or (2) those experiencing any of the following medical conditions: development of other organ dysfunctions with severe comorbidities, on long-term mechanical ventilation, with infectious disease and comorbidities, with cachexia or severe death-causing malnutrition, and with end-stage cancer. The proportion of patients who satisfied each criterion is shown in Table 1.
Distribution of Patients Satisfying the Taiwan National Health Insurance Criteria for Terminal Illness (n = 47)
Among the 47 terminally ill patients, 38 were on hemodialysis. Among the 164 nonterminally ill patients, 110 were on hemodialysis. The total sample was composed of 148 dialysis patients, 137 of which completed the survey at both time points. A recruitment flowchart is shown in Figure 1.
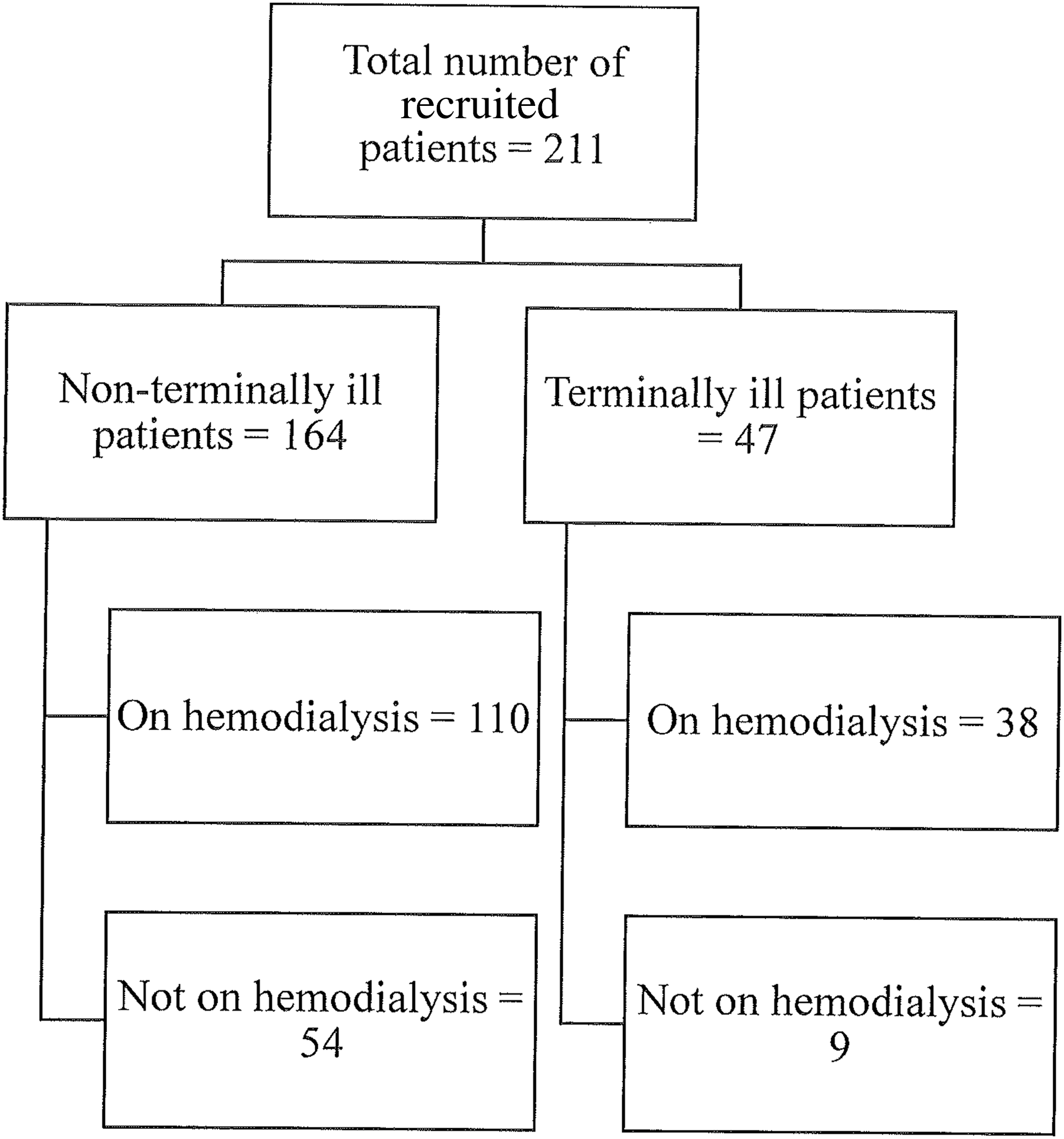
Recruitment flowchart.
Measurements
Symptom burden
The symptom burden of ESRD patients was assessed using the Taiwanese version of the MD Anderson Symptom Inventory for kidney disease (MDASI-T-K). MDASI was primarily developed to measure multiple symptoms in patients with cancer and contains a set of common symptoms that can be rated by all cancer patients from the time they begin treatment throughout the course of their disease. 18 The MDASI comprises 13 items rated based on the level of symptom severity within the last 24 hours. Each symptom is rated on an 11-point Likert scale (0–10) to indicate severity, with 0 denoting “not present” and 10 denoting “as bad as you can imagine.” In addition, the inventory consists of six items that are rated based on the extent to which symptoms interfere with general activities. Responses on these items are also rated on a 0–10 numerical rating scale, ranging from “did not interfere” to “completely interfered.”
The Taiwanese version (MDASI-T) was validated in a sample of 556 Taiwanese patients with multiple diagnoses of cancer. 19 The internal consistency of the MDASI-T was 0.89 for the symptom severity subscale and 0.94 for the interference subscale. For the MDASI-T-K, two more items on symptom severity, which were found in more than half of ESRD patients, were added: pruritus 20 and lower limb weakness. 21 The content of the MDASI-T-K was assessed and verified by an expert panel consisting of six nephrologists and six senior nurses specialized in nephrology. The ratings in the MDASI-T-K were averaged into the following subscale scores: mean total symptom severity (15 symptom severity items) and mean total interference (6 interference items).
Severity of comorbidities
The severity of comorbidities of ESRD patients was measured using the Charlson comorbidity index (CCI). The CCI consists of 19 categories of comorbidity, and each condition carries a score of 1, 2, 3, or 6. The total scores range from 0 to 37, with higher CCI scores indicating greater comorbidity and associated with poorer outcomes and overall survival. 22 CCI is considered a valid tool to assess comorbidity and predict survival in patients with ESRD. 23 In this study, the CCI scores were adjusted with age. For each decade after the age of 40 years, one point was added to the CCI score until a total of four points. 24
Demographic characteristics
A demographic questionnaire was designed to elicit information on patients' background, including age, years of education, marital status, religious affiliation, employment status, and duration of hemodialysis.
Procedures
Data were collected from January 2010 to December 2011. Convenience sampling was used for recruitment. Eligible participants were first referred from physicians of the study sites. Subsequently, potential participants were individually approached by trained research assistants to confirm eligibility. Study details were explained to eligible participants. After obtaining a written informed consent, the MDASI-T-K and demographic questionnaire were administered. The medical record of the participants was reviewed by the research assistants to complete the CCI.
For patients on hemodialysis, data collection time points were specially chosen, that is, at the beginning and end of the weekly cycle of their hemodialysis sessions. For those not on hemodialysis, the questionnaires were administered at the time of recruitment.
Statistical analyses
Descriptive statistics were used to illustrate the background characteristics and MDASI-T-K scores of participants. Independent t-tests were performed to compare the MDASI-T-K scores of dialysis and nondialysis patients and those of terminally ill and nonterminally ill patients. To determine factors associated with symptom severity, a linear regression analysis was performed. The MDASI-T-K total symptom severity scores were used as the dependent variable in the regression models, whereas hemodialysis and background characteristics were used as independent variables.
In addition, a paired t-test was used to examine the change in MDASI-T-K scores at the beginning and end of the weekly cycle of hemodialysis sessions. For dialysis patients, the MDASI-T-K scores obtained from the first time undertaking the survey were used to represent symptom severity in all analyses except for the paired t-test. All statistical analyses were conducted using the SPSS software, and all tests involved a two-sided significance level of p = 0.05.
Results
Background characteristics of samples
The background characteristics of the participants are shown in Table 2. Of the 211 participants, almost half were women (48.8%). The mean age was 63.45 years. Most participants received more than nine years of education (61.6%), were married (78.7%), were not employed (72.5%), and had religious beliefs (73.5%). More than two-thirds of the participants were on hemodialysis (70.1%) and not terminally ill (77.7%). With regard to clinical indices, the blood urea nitrogen level, serum creatinine level, and estimated glomerular filtration rate were 76.50 ± 25.00 mg/dL, 9.54 ± 3.28 mg/dL, and 6.17 ± 2.97 mL/(min ·1.73 m 2 ), respectively. The total CCI score was 5.70 ± 2.28. Among those receiving hemodialysis, the mean duration of hemodialysis was 54.5 months.
Demographic Characteristics (n = 211)
Patients receiving hemodialysis only.
SD, standard deviation.
Comparison of symptom burden between hemodialysis and nonhemodialysis patients
Table 3 shows the mean MDASI-T-K scores of terminally ill and nonterminally ill patients. Generally, the most severe symptom was fatigue (mean: 2.91 ± 2.84), followed by disturbed sleep and lower limb weakness. The least severe symptom was vomiting (mean: 0.31 ± 1.12).
Symptom Severity and Symptom Interference of End-Stage Renal Disease Patients
*p-Value obtained by independent t-test (patients receiving hemodialysis vs. patients not receiving hemodialysis).
When we compared the terminally ill hemodialysis and nonhemodialysis participants, the nondialysis patients scored higher on severity of fatigue (hemodialysis: 2.81 ± 1.84 vs. nonhemodialysis: 5.89 ± 3.51, p = 0.009; Table 3) and lack of appetite (hemodialysis: 1.95 ± 2.75 vs. nonhemodialysis: 5.00 ± 3.20, p = 0.006) than the dialysis patients. In terms of mean total symptom severity and interference, hemodialysis patients had scores comparable with those not on hemodialysis.
In nonterminally ill patients, nondialysis patients scored significantly higher on both total symptom severity (hemodialysis: 1.40 ± 1.06 vs. nonhemodialysis: 2.27 ± 1.15, p < 0.01) and symptom interference (hemodialysis: 1.18 ± 1.47 vs. nonhemodialysis: 2.44 ± 2.13, p < 0.01), as well as eight individual severity items (fatigue, nausea, distress, shortness of breath, drowsiness, sadness, vomiting, and lower limb weakness).
Predictors of symptom severity in terminally ill and nonterminally ill ESRD patients
As shown in the regression analysis (Table 4), overall, terminally ill patients were more likely to report higher symptom burden (B = 0.604, p = 0.017), whereas those on hemodialysis tended to report lower symptom severity (B = −0.614, p = 0.014). In nonterminally ill patients, those who were married or on hemodialysis were more likely to experience lower symptom severity (B = −0.604, p = 0.013 and B = −0.665, p = 0.017, respectively). However, the use of hemodialysis and other background characteristics did not predict the total symptom severity in terminally ill patients.
Predictors of Symptom Severity of End-Stage Renal Disease Patients
Notes: Ref, reference categories; SE, standard error.
Changes in symptom severity over the weekly cycle of hemodialysis
With regard to changes in the MDASI-T-K total symptom severity and interference scores from the beginning until end of the weekly cycle of hemodialysis sessions, no significant change was found in both terminally ill and nonterminally ill patients (Table 5).
Comparison of Symptom Severity and Interference Before and After Hemodialysis
Discussion
The study demonstrated the differential effects of hemodialysis on the symptom burden of terminally ill and nonterminally ill ESRD patients. An association between hemodialysis and lower symptom burden was only manifested in the nonterminally ill group, but not in the terminally ill group. Although no predictors of symptom severity could be found in terminally ill patients, nonterminally ill patients who were on hemodialysis or married tended to experience lower symptom severity. Dialysis patients, in both the terminally ill and nonterminally ill groups, still experienced similar levels of symptom severity and interference from the beginning until the end of a weekly cycle of hemodialysis sessions.
Researchers have suggested that for near-the-end-of-life ESRD patients under maintenance dialysis, much of the symptom burden may be attributable to dialysis therapy itself and the burden of dialysis may outweigh its merit.16,25 In this study, hemodialysis did not deteriorate the symptom burden of patients, including those who were terminally ill. Although hemodialysis was not associated with higher symptom burden in terminally ill patients, the absence of hemodialysis' beneficial effect on symptom relief underscores the importance of reevaluating dialysis care for those in the terminal phase. This is because hemodialysis often imposes additional burden to patients, such as invasive procedures and time commitment, which are important factors affecting patient preferences for conservative care versus dialysis. 26
To minimize the burden of dialysis imposed on terminally ill patients, the emphasis of care may be shifted toward minimizing the physical and psychological burden of dialysis. 16 For example, “palliative dialysis” would allow patients to receive as-needed dialysis treatments on a less regular schedule to alleviate the symptoms of uremia and fluid overload. 27 If conservative therapy is chosen over dialysis, adequate symptom control and palliative care should be provided. Previous studies showed that ESRD patients wished to be aware of all treatment choices; however, information regarding these choices was not often accessible. 28 Therefore, it is important to provide patients with sufficient information and establish a shared decision-making relationship with regard to treatment options.
This study supported that dialysis patients generally experienced less severe symptoms than nondialysis patients and the difference is significant in the nonterminally ill group. To our knowledge, two surveys conducted in Australia and Hong Kong have compared the symptom burden of dialysis patients against nondialysis patients and both found a lower symptom burden in the latter group.7,9
There can be a few plausible explanations for the aforementioned discrepancy. First, hemodialysis practices, particularly the point at which dialysis is initiated (which should neither be too early nor too late) and symptom management strategies, vary across countries 29 and may have contributed to the occurrence of different symptoms in the dialysis group. Second, some patients did not receive hemodialysis possibly due to reasons related to their advanced condition that leads to withdrawal of dialysis or unsuitability to initiate dialysis. Therefore, they may experience higher symptom burden than dialysis patients. Similarly, some dialysis patients may have symptoms secondary to fluid retention (such as shortness of breath) relieved by hemodialysis. Thus, they may report lower symptom severity than nondialysis patients. Third, a comprehensive national health insurance program has been implemented in Taiwan since 1995, under which ESRD patients are eligible for any type of renal replacement therapy free of charge. 30 The national dialysis surveillance program initiated in 1987 in Taiwan has improved the quality of dialysis therapy. 31 This may also have minimized provider unawareness of symptom management, which has been considered a barrier to symptom control related to hemodialysis in the United States.32,33 These factors may have collectively contributed to the improvement in symptom experience of dialysis patients in Taiwan. However, more research is required to examine the difference in hemodialysis practices, the influence of universal coverage of dialysis, and the symptom management relevant to dialysis care in different settings.
Hemodialysis and marital status were associated with lower symptom burden in nonterminally ill patients in our study, whereas hemodialysis, older age, and female gender predicted greater symptom burden in a previous study. 9 These inconsistent findings regarding hemodialysis may be explained by variations in patient composition and hemodialysis practices. Of note, in Almutary's study, marital status was not included in their regression model. 9 In addition, given that no predictors of symptom severity could be identified in terminally ill patients, qualitative studies should be conducted in the future to explore factors that may affect symptom severity, such as effectiveness of various symptom management strategies.
Our study has important implications. It demonstrated the beneficial effects of dialysis in reducing the overall symptom burden of nonterminally ill patients and the absence of such beneficial effect in terminally ill patients. Therefore, it is essential for dialysis care providers to discuss available dialysis options with terminally ill patients (such as initiate or not, continue or discontinue dialysis, and provide optimal medical management and palliative treatment accordingly). Patients and families should be well informed about the potential benefits and burdens of different options and should be actively involved in decision making. In addition, for nonterminally ill patients, health professionals should identify those patients who tend to experience higher symptom burden (i.e., those not married and/or not on hemodialysis) and provide appropriate symptom assessment and management.
However, our study had some limitations. First, convenience sampling was adopted, and the number of terminally ill patients was small. This may limit the generalizability of the entire ESRD population. Second, our data lack the following information: reasons for not undergoing hemodialysis, whether the decision of starting dialysis was based on patients' symptoms, and symptom management strategies employed accompanying dialysis. Further research should utilize this type of data, which may be useful in explaining the inconsistent effects of hemodialysis observed in our and previous studies. Third, although the study involved two data collection points with a one-week interval to study the change in symptom burden in patients undergoing hemodialysis, the short follow-up period was not adequate to reflect the trajectory of symptom burden over the course of hemodialysis. In addition, symptom severity was not assessed immediately after the hemodialysis session. Hence, future research should include the immediate postdialysis time point and adopt a longitudinal design to follow up patients undergoing dialysis for a longer period of time.
In conclusion, our findings demonstrated that hemodialysis had differential effects on the symptom burden of terminally ill and nonterminally ill ESRD patients. Hemodialysis only predicted the lower symptom burden in nonterminally ill patients, but not in terminally ill patients. The need to revisit and discuss palliative treatment options, in addition to dialysis, with patients approaching the end of life and their families to maximize patient outcomes should be addressed.
Footnotes
Acknowledgments
The authors thank all study participants. This research did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.
The study was approved by the ethical committee of Taipei Tzu Chi Hospital and the institutional review board of Taipei Medical University Hospital.