
Abstract
Abstract
Background:
End-stage renal disease (ESRD) is a life-limiting condition that is often complicated by acute abdominal emergency. Palliative care (PC) has been shown to improve the quality of life in patients with serious illness and yet is underutilized. We hypothesize that ESRD patients with abdominal emergency have high unmet PC needs.
Objective:
To characterize the outcomes of ESRD patients with acute surgical abdomen, define PC utilization patterns, and identify areas of unmet PC needs.
Design:
Retrospective study querying the National Inpatient Sample database (2009–2013).
Setting and Subjects:
Subjects were identified using ICD-9 codes for those aged ≥50 with preexisting diagnosis of ESRD with an acute abdominal emergency diagnosis of gastrointestinal perforation, obstruction, or ischemia.
Measurements:
Outcomes included PC rate, in-hospital mortality, discharge disposition, and intensity of care. Multivariable logistic regression analysis was used to identify predictors of PC.
Results:
A total of 9363 patients met the inclusion criteria; 24% underwent surgery, 16% died in hospital, and 43% were discharged to dependent living. Among in-hospital deaths, 23% received PC. Only 4% of survivors with dependent discharge received PC. Surgical mortality was 26%. PC was less utilized in surgical patients than nonsurgical patients. PC was associated with shorter hospital stay. Predictors of PC included increasing age, severity of underlying illness, white race, teaching hospitals, and the Western region.
Conclusions:
Patients with ESRD admitted for acute abdominal emergency have high risk for mortality and functional dependence. Despite this, few receive PC and have a high utilization of nonbeneficial life support at the end of life.
Background
More than 700,000
The ability to accurately prognosticate surgical outcomes, especially in emergent settings, is critical to ensuring that treatments are aligned with patient values. Palliative care (PC) centers around achieving this goal-concordant care, and it has been shown to result in better and earlier control of symptoms, shorter hospital stays, and fewer invasive interventions in patients with serious and life-limiting illnesses.7,8 Research suggests that patients who clearly understand their prognosis are less likely to choose invasive treatments that prolong suffering and time away from home. 9 PC can also assist with decision making in patients with acute abdominal emergency, regardless of whether surgical intervention is pursued. 10 Although patients with ESRD have been identified as appropriate candidates for PC from the time of diagnosis or initiation of dialysis,11,12 few are referred.
One of the barriers to PC in the emergency surgical setting is perceived uncertainty regarding prognosis. For patients with ESRD and acute abdominal surgical emergency, improving goal concordance and patient-centered care must, therefore, begin with a better understanding of expected outcomes to formulate treatment plans that best benefit the individual patient. However, surgical outcomes specifically related to acute abdominal emergencies in patients with ESRD remain poorly characterized. In addition, the extent of PC utilization in patients with ESRD and acute abdominal emergency is not yet defined. In this study, we sought to study the outcomes of ESRD patients with acute abdominal emergency and patterns of PC utilization.
Objective
The purpose of this study is (1) to characterize the outcomes of ESRD patients with acute surgical abdomen, (2) to define patterns of PC utilization, and (3) to identify specific areas of unmet PC needs in this population. We hypothesized that patients with ESRD who develop acute abdomen have poor outcomes yet rarely receive PC.
Design
This is a retrospective study that queried the National Inpatient Sample (NIS) from 2009 to 2013. NIS encapsulates nearly 20% of all hospitalizations in the United States, gathering information from 44 states and 4378 hospitals.13,14
Setting and Study Population
Study subjects were identified using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Patients aged 50 or older with preexisting ICD-9 diagnosis of ESRD who present emergently or urgently with an acute abdominal emergency diagnosis of gastrointestinal perforation, obstruction, or ischemia were included. Cases with acute renal failure or kidney transplant were excluded. Cases were excluded if they had incomplete or missing data on patient or hospital characteristics (Fig. 1). See Appendix Tables A1–A4 for pertinent ICD-9 codes.
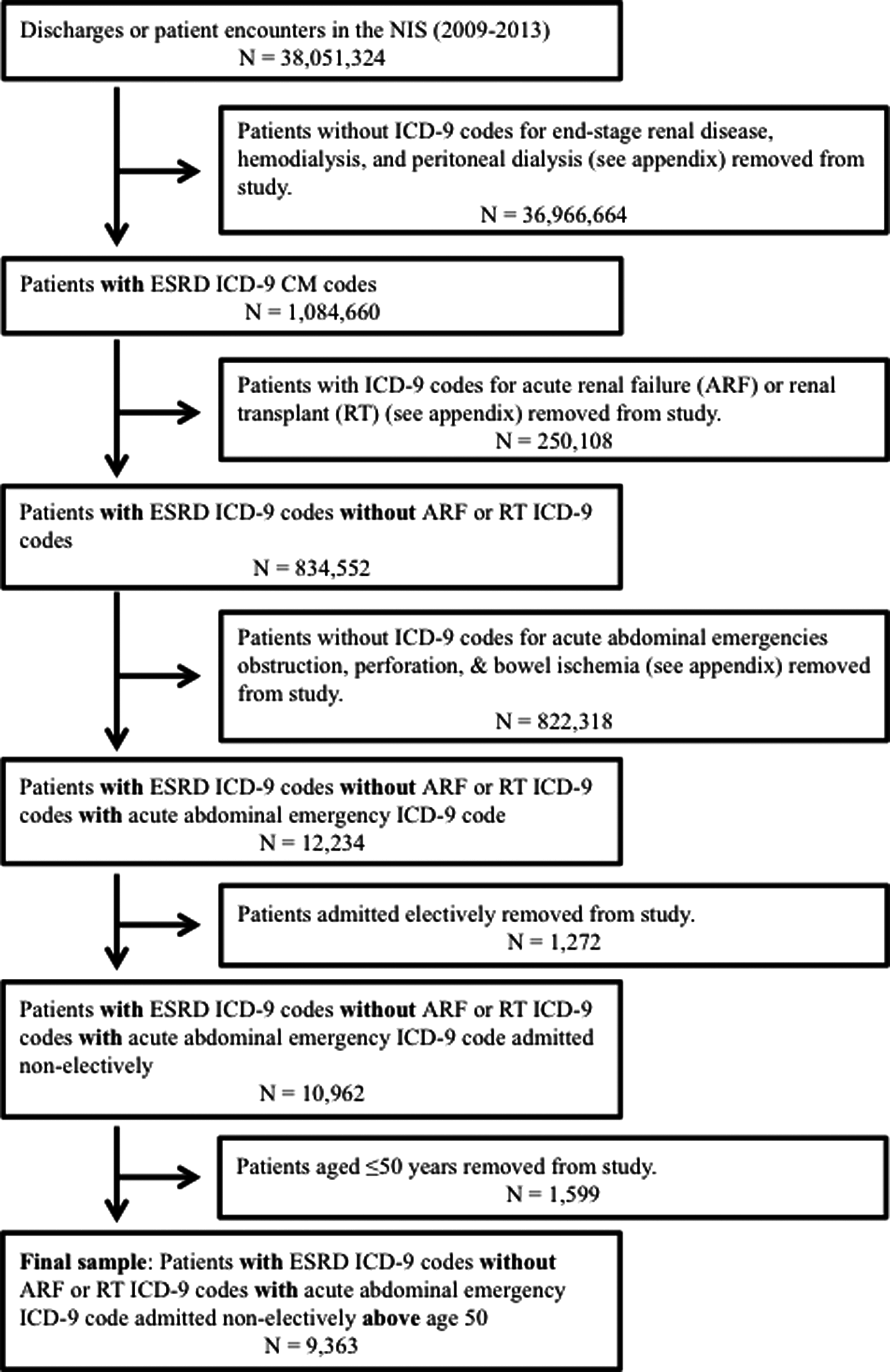
Establishment of the cohort from the NIS based on ICD-9-CM codes. ESRD, end-stage renal disease; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; NIS, National Inpatient Sample.
Measurements
Outcomes
Outcome variables included in-hospital mortality, discharge disposition, PC utilization, intensity of care, hospital length of stay (LOS), and total charges. Discharge disposition was categorized as either independent or dependent living among those who survived the hospitalization. Discharge to independent living is defined as discharge home to self-care with no additional health care services, whereas dependent living refers to transfer to facility, transfer to short-term hospital, and discharge with home health care services. Utilization of PC was defined by the ICD-9 diagnosis code v66.7, which may be used for any patient determined to be the recipient of PC, comfort care, end-of-life care, or hospice care. Intensity of care was defined as following interventions: ventilator support, dialysis, tracheostomy, or percutaneous endoscopic gastrostomy (PEG) tube placement. See Appendix Tables A1–A4 for pertinent ICD-9 codes.
Covariates
Patient covariates included surgical diagnosis (gastrointestinal perforation, gastrointestinal obstruction, bowel ischemia, and mixed, which includes any combination of the three diagnoses), age, gender, race, payer status, and socioeconomic status (based on zip code income quartiles). Hospital characteristics included bed size (small, medium, and large), region (Northeast, Midwest, South, and West), and location/teaching status (rural, urban nonteaching, and urban teaching). We described the patients' comorbidity burden using a summary count of Elixhauser comorbidities (0, 1, 2, 3, or more comorbidities). We used the Elixhauser comorbidities available in the NIS Severity Files provided by Healthcare Cost and Utilization Project (HCUP). A weighted Elixhauser comorbidity score was generated using previously published weights as a covariate in the regression analyses. The Elixhauser comorbidity score was preferred over the routinely used Charlson Comorbidity index as it has been proven to be more discriminative for in-hospital deaths. 15
Statistical analysis
We first described the patient-level and hospital-related characteristics of our cohort, using counts and proportions for categorical variables and means with standard deviations for continuous variables. Using cross tabulations, we then described primary outcomes by the type of diagnoses and treatment strategy (surgical vs. nonsurgical). Next, we performed subgroup analyses. Within each stratum of discharge disposition, we assessed the association between the treatment strategy and PC utilization using chi-square tests. We fit a multivariable logistic regression model using all study variables (full model) to identify independent predictors for PC. Adjusted odds ratios generated from the full multivariable logistic regression model were interpreted using a p-value of 0.05 as cutoff for assessing statistical significance. All statistical analyses were performed using SAS v. 9.4 (SAS Institute, NC). Given the complex multistage stratified design of the NIS, we used SAS's survey procedures to account to generate unbiased results using sampling weights provided by the HCUP.
Results
The NIS database from 2009 to 2013 linked 9363 hospitalizations to patients with ESRD who were admitted with our acute abdominal emergency diagnoses. Three patients were missing discharge disposition. Clinical and demographic characteristics are shown in Table 1. A majority of patients were <80 years old (82%), had Medicare (84%), and had four or more comorbidities (61%).
Patient Demographics and Hospital Characteristics
Missing data for payer status, median household income, hospital location/teaching status, hospital bed size, and discharge disposition were omitted; they account for <2% of the total for each category.
Elixhauser comorbidities excluded conditions associated with renal failure and only the Elixhauser comorbidity score was used for logistic regression.
To study the outcomes of patients with ESRD and acute abdomen, we characterized patient mortality and discharge disposition according to the treatment strategy (surgical vs. nonsurgical) and diagnosis (gastrointestinal obstruction, perforation, ischemia, or mixed pathology) (Table 2). Overall, 16% of patients died in hospital, and 43% were discharged to dependent living (26% were transferred to facilities, 14% were discharged with home health care services, and 3% were transferred to an acute hospital). Almost a quarter (24%) of patients underwent abdominal surgery. Mortality rate for the surgical patients was twice that of nonsurgical patients (26% vs. 13%; p < 0.0001), and fewer surgical patients were discharged to independent living (21% vs. 47%; p < 0.0001). Surgical patients had higher weighted Elixhauser comorbidity scores as compared with nonsurgical patients (median 7 vs. 5; p < 0.0001). Gastrointestinal obstruction (45%) was the most common surgical diagnosis among our patient cohort. Outcomes varied substantially based on surgical diagnosis, with bowel ischemia and mixed pathology diagnoses associated with increased mortality compared with perforation and obstruction (39% and 34% vs. 11% and 12%, respectively).
Discharge Disposition by Treatment Strategies and Surgical Diagnoses
Discharge to independent living refers to discharge home to self-care. Dependent living refers to transfer to facility, transfer to short-term hospital, discharge with home health care services, unknown discharge destination, or leaving against medical advice, as defined by National Inpatient Sample.
We examined associations between the treatment strategy and PC utilization stratified by discharge disposition (Table 3). Overall, only 5% of the cohort received PC. Among mortalities, 23% received PC, with a significantly more frequent PC in nonsurgical patients compared with surgical patients (24% vs. 20%; p = 0.029). Among patients who were discharged to dependent living, only 4% received PC. Nonsurgical patients utilized PC twice as frequently in this subcohort (4% vs. 2%; p = 0.003).
Palliative Care utilization and Treatment Strategies Stratified by Discharge Disposition
Fisher's exact test used.
The relationship of PC to intensity of care for the whole cohort was examined. (Table 4). Fifteen percent of the entire cohort received ventilatory support, and >80% underwent dialysis during the hospitalization. Only a small portion of the cohort underwent tracheostomy (1%) or PEG placement (1%). PC was associated with more ventilator utilization (35% vs. 14%), but less dialysis utilization than no PC (67% vs. 81%; p < 0.0001).
Intensity of Care and Palliative Care Utilization in the Entire Cohort
PEG, percutaneous endoscopic gastrostomy.
The relationship of PC to intensity of care and life support at the end of life was examined (Table 5). Among mortalities, patients who received PC had less ventilator utilization (45% vs. 53%; p = 0.02) and less surgery (34% vs. 40%; p = 0.03) than those who did not receive PC. However, PC had no association with utilization of dialysis or tracheostomy at the end of life. The mortalities who received PC had shorter hospital LOS (6 vs. 8 days; p = 0.057) and lower hospital charges than those without PC ($71,062.50 vs. $84,702.00; p = 0.006) (Table 6). Interestingly, PC was associated with decreased LOS and hospital charges among survivors who were discharged to dependent living. In addition, patients who received PC had a significantly shorter hospital stay and fewer charges, even though their Elixhauser comorbidity score was higher.
Intensity of Care and Palliative Care Utilization in Patients Who Died in Hospital (n = 1482)
Palliative Care Utilization and Hospital Length of Stay and Charges Stratified by Discharge Disposition
LOS, length of stay.
Lastly, we examined patterns of PC utilization with a multivariable logistic regression analysis (Table 7). The logistic regression analysis of patient characteristics revealed that patients who were older (age >70) and sicker (a higher weighted Elixhauser comorbidity score) were more likely to receive PC. Hispanics and blacks were less likely to receive PC compared with whites (adjusted odds ratio [aOR] 0.5; 95% confidence interval [CI] 0.4–0.8 and aOR 0.6; 95% CI 0.5–0.8, respectively). Patients with private or other payer status were more likely to receive PC than those on Medicare (aOR 1.6; 95% CI 1.1–2.2 and OR 2.2; 95% CI 1.1–4.5, respectively). Surgical diagnoses, such as bowel ischemia or mixed pathology, were predictors of PC, in comparison with obstruction (aOR 2.2; 95% CI 1.7–2.9 and aOR 2.1; 95% CI 1.4–2.9, respectively). The treatment strategy, whether surgical or nonsurgical, was not an independent predictor of PC utilization when adjusting for all other variables. Analyses of hospital characteristics revealed that patients treated in larger hospitals, hospitals in the Western region, or urban teaching hospitals were significantly more likely than their counterparts to utilize PC.
Predictors of Palliative Care Utilization Using Multivariate Logistic Regression
Statistically significant variables (p < 0.05).
CI, confidence interval; OR, odds ratio.
Conclusions
One in six ESRD patients with acute abdominal emergency died in hospital, highlighting a vulnerable patient population with high PC needs. Moreover, for those requiring surgical intervention, 25% died, and only 20% were discharged to independent living. Despite these poor outcomes, again, few received PC. Mortality rates at this level would certainly be consistent with accepted indications for PC among hospitalized patients, 16 suggesting that any patient with ESRD who presents for emergency abdominal surgery or acute abdomen should receive these services.
Predictors to receive PC were higher severity of underlying illness and older age, suggesting a general focus by physicians on traditional prognostic factors, or perceived futility and risk of death. The PC rate was significantly lower in patients who underwent surgery, which aligns with other studies that find that surgeons perceive a dichotomous relationship between surgery and PC 17 and reflects the traditional model of physicians offering PC only after aggressive treatment has failed. Despite this, the NIS dataset only has data on presence or absence of PC, but no data on the timing of PC during the hospitalization, which would be a more relevant measure of practice patterns for this population. The variability across race, US regions, hospitals, and payer are consistent with other population studies on PC utilization 18 and suggest that institutional and local practice culture has a significant impact on medical and surgical decisions for individual patients regarding PC. These all suggest potential target areas for efforts to improve access to and delivery of PC on the individual and systems levels.
Patients with ESRD, in general, face a high baseline mortality risk and significant health-related burdens. Despite these sequelae and most patients' desire to discuss their values, goals, and preferences with their treating physicians, these discussions occur rarely. 4 Indeed, although decisions about the initiation of dialysis represent a pivotal point in the health care trajectory of ESRD patients, dialysis is often begun without appropriate advance care planning and consideration of alternative supportive care strategies. 19 Barriers to such discussions include prognostic uncertainty, concerns about patients' or family's distress, and lack of clarity about the “right time” for initiating such a conversation. 20 In the context of an acute abdominal emergency, the challenges of acute surgical decision making are further compounded by the lack of advance directives and clear health care goals. 12 Our data provide another contribution to prognosis for ESRD patients when physicians are discussing goals of care. An acute surgical abdomen is one of the many emergencies that can arise in patients, others including cardiovascular, cerebrovascular, infectious, and traumatic cases. Although the outcomes evaluated in our study do not translate to other acute medical or surgical problems, the approach to patients with ESRD should be similar. The focus on prognosis, specifically with respect to outcomes that matter to patients, should be the goal and we should aim to engage PC as a conduit for allowing conversations to take place to ensure patients' goals remain the foundation of treatment plans. This study further delineates opportunities for advance care planning both before an emergency surgical intervention is contemplated and in the immediate perioperative period.
The National Consensus Project for Quality Palliative Care advocates for PC along the course of illness, concurrently with curative or life-prolonging therapy 21 and the subspecialty of surgical palliative care also advocates for this approach. Our study suggests that patients with ESRD who present with an acute abdomen represent a clear opportunity for PC integration from the time of admission in the emergency department. Even in institutions in which PC team and consultation are not available, these data can be used by the surgeons to provide “primary PC” when communicating with patients and their families by underpinning the implications of the acute surgical problem in the context of the underlying ESRD to reach goal-concordant treatment plans.
As expected, the rate of PC was the highest among patients who died. Interestingly, among the deaths, PC was associated with less nonbeneficial ventilator support and lower LOS and cost. This is consistent with other literature that shows that PC is associated with less nonbeneficial life support in a variety of populations.22,23 PC was not associated with less utilization of dialysis at the end of life in our study, and this is also consistent with other literature, which find that withdrawal of dialysis in ESRD patients involves complex decisions and is complicated by the Medicare benefits for dialysis. 24 The withdrawal from dialysis before death among patients with ESRD has increased for the past decade,1,25 and a case-control study showed that patients with ESRD with advance care planning were more likely to withdraw from dialysis in accordance with their preferences at the end of life. 26 Only two-thirds of the in-hospital deaths underwent dialysis, less frequently than the entire cohort. This suggests that patients who were approaching end of life chose not to pursue dialysis during hospitalization, regardless of whether formal PC was involved or not. However, as NIS does not distinguish patients who were on dialysis before admission and then had it withdrawn from those who did not undergo dialysis during the hospitalization, it is hard to draw a meaningful conclusion.
Despite no reduction in utilization of dialysis, our study demonstrates that patients with PC had decreased hospital stay and lower charges compared with those without PC. This was true for both mortalities and survivors discharged to dependent living. Our findings corroborate studies in many populations that PC was associated with shorter LOS and reduced hospital charges, 27 especially in dying patients in the ICU.8,22,28,29
There are limitations of this study due to the nature of the administrative dataset utilized. First, there is likely an overall underreporting of patients who received PC, of patients with an acute abdomen, and of patients who underwent surgery. Although the use of the v66.7 diagnosis code in large dataset analyses is limited by poor sensitivity (49% in a large single-center validation study 30 ), even doubling our detected rate to account for failure to capture would result in a rate of PC utilization that does not nearly approach the degree of demand. We were selective in the diagnosis codes used to define acute surgical abdomen, modeling our range after previously published studies, 9 and excluding other surgical diagnoses such as gastrointestinal hemorrhage and trauma. Finally, NIS data include no information on patient-centered outcomes, patient preferences, advance directives, or posthospitalization outcomes, which are subject to significant effects from PC.
In summary, our study reveals important prognostic information about outcomes in emergency abdominal surgical conditions for patients with ESRD and defines unmet PC needs in this population. It also highlights opportunities for further studies to better understand the barriers and systems issues to integrating surgical PC into hospital care in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
This study was funded by U.S. Department of Health and Human Services, Health Resources and Services Administration (D34HP26020) and Patient-Centered Outcomes Research Institute (PCORI-1502-27462).
Appendix
ICD-9-CM Procedure Codes to Represent Intensity of Care
| Ventilator | 96.7, 96.70, 96.71, 96.72 |
| Dialysis | 39.95, 54.98 |
| Tracheostomy | 31.1, 31.2, 31.21, 31.29 |
| Percutaneous endoscopic gastrostomy | 43.11 |